Introduction
ERC/mesothelin is a glycoprotein which is expressed
on the surface of mesothelial cells covering body cavities such as
the pleura, pericardium and peritoneum. This protein is expressed
on various malignant tumors, including mesothelioma and pulmonary,
pancreatic and ovarian carcinomas. Recently, it has been recognized
that the measurement of blood N-ERC/mesothelin levels aids early
detection in and postoperative therapeutic monitoring of patients
with mesothelioma, who have been exposed to asbestos (1–3).
The early detection of mesothelioma by diagnostic
imaging is considered to be difficult; however, if N-ERC/mesothelin
is used as a tumor marker for mesothelioma, patient prognosis may
be improved. ERC/mesothelin has also been reported to be expressed
in ovarian carcinoma (4), however,
similar to mesothelioma, its early detection is also considered to
be difficult. Therefore, it is believed that if blood
N-ERC/mesothelin levels in patients with ovarian carcinoma
increase, it may be used as a tumor marker for early detection in
and therapeutic monitoring of patients with ovarian carcinoma,
similar to mesothelioma.
ERC/mesothelin is a homolog of the mesothelin/MPF
gene, which is preferentially expressed in hereditary rat renal
carcinoma, and its products are secreted in the blood (5). ERC/mesothelin, a 71-kDa precursor
protein, is also expressed on the surface of human cells and is
cleaved by catabolic enzymes. While the 40-kDa C-terminal fragment
remains bound to the cell membrane as it contains the GPI anchor
region, the 31-kDa N-terminal fragment is extracellularly secreted
as a soluble protein (6). The
C-terminal fragment or C-ERC/mesothelin has been reported to be
used as a tumor marker for mesothelioma and ovarian carcinoma
(7). Blood samples from patients
with mesothelioma have been examined for the N-terminal fragment or
N-ERC/mesothelin by enzyme-linked immunosorbent assay (ELISA). In
the present study, we determined serum N-ERC/mesothelin levels in
patients with ovarian carcinoma using sandwich ELISA. In addition,
we immunohistochemically evaluated surgically resected specimens
for C-ERC/mesothelin expression on the tumor cell membranes.
Subjects and methods
Human subjects
Our study for the tumor marker of ovarian carcinoma
was approved by the Institutional Review Broad of Juntendo Urayasu
Hospital and the hospital of Juntendo University School of
Medicine, Immuno-Biological Laboratories. Patients signed an
informed consent form.
Serum samples
Peripheral blood was obtained from patients who were
evaluated for possible participation in this study. Serum from 32
patients with ovarian tumors were evaluated in this study. The
median age of the patients with ovarian tumors was 51.2 years
(range, 20–75). Serum samples from the 32 patients with ovarian
tumors (18 carcinoma, 2 borderline tumors, 4 Krukenberg tumors, 3
sex-cord stromal tumors and 5 benign tumors) were evaluated in the
present study. Sera from healthy volunteers were also obtained.
Tissue sections were obtained from archival paraffin-embedded tumor
blocks from surgically resected specimens to evaluate the ovarian
tumors.
Immunohistochemistry
Tissue sections obtained from archival
paraffin-embedded tumor blocks from surgically resected specimens
were evaluated for C-ERC/mesothelin expression. Tissue sections
4-μm thick were prepared from formalin-fixed,
paraffin-embedded specimens. The detection of ERC/mesothelin was
performed using the anti-mesothelin monoclonal antibodies (mAbs)
22A31 or 5B2 (1,8). Following deparaffinization, the tissue
sections were heated in 10 mM citrate buffer for antigen retrieval.
Immunohistochemical detection was performed with the Ventana
automated staining system. C-ERC/mesothelin positivity was
identified by brownish staining of the tumor cell membranes and
graded as positive if ≥30% of the accessible tumor cells were
labeled.
Sandwich ELISA
Serum N-ERC/mesothelin was determined using the
sandwich ELISA system. The details of sandwich ELISA have been
previously described (1). The 7E7,
PoAb282 and 16K16 mAbs were used as the antibody. 7E7 mAb is the
common capture antibody and PoAb282 and 16K16 mAb were used as the
capture antibody. The epitope of PoAb282 is in the C-terminal side
[N(7-4)] and 16K16 mAb is in the N-terminal side [N(7-16)].
Results
Serum N-ERC/mesothelin levels
We measured serum N-ERC/mesothelin levels in 32
patients with ovarian tumors. Of these, 20 patients had primary
ovarian carcinoma and borderline tumors; 8 were at stage I, 1 was
at stage II and 11 were at either stage III or IV. Serum samples
were collected prior to surgery or chemotherapy from 11 patients
and during chemotherapy against carcinomatous pleural effusion or
ascites following surgery from 9. The cut-off levels of N(7-4) and
N(7-16) at 2.78 and 5.6 ng/ml, respectively, in the patients with
mesothelioma have been previously reported (2). Of the 20 patients with ovarian tumors,
one in the preoperative group showed increased N-ERC/mesothelin
levels [N-ERC/mesothelin: N(7-4) = 4.76 ng/ml, N(7-16) = 18.67
ng/ml; Table I]. The median serum
levels of the 4 Krukenberg tumor patients, 3 sex-cord stromal tumor
patients and 5 benign tumor patients were N(7-4) = 2.12, 1.6 and
1.9 ng/ml and N(7-16) = 4.2, 1.5 and 2.0 ng/ml, respectively.
 | Table I.ERC/mesothelin levels of ovarian
carcinoma and ERC/mesothelin expression observed by
immunohistochemical staining.a |
Table I.
ERC/mesothelin levels of ovarian
carcinoma and ERC/mesothelin expression observed by
immunohistochemical staining.a
| Histological
type | N(7-4) ng/ml | N(7-16) ng/ml | CA125(0–35.0) | 5B2 | 22A31 |
|---|
| Clear
adenocarcinoma | 1.06 | 1.26 | 124.70 | + | + |
| Endometrioid
adenocarcinoma | 1.06 | 1.62 | - | − | − |
| Serous
adenocarcinoma | 7.16 | 8.06 | 793.20 | + | + |
| Clear
adenocarcinoma | 1.54 | 2.11 | 104.70 | − | − |
| Serous
adenocarcinoma | 4.33 | 3.89 | 4.10 | − | − |
| Clear
adenocarcinoma | 2.69 | 1.79 | 33.20 | − | − |
| Endometrioid
adenocarcinoma | 1.91 | 2.69 | 6.40 | − | − |
| Clear
adenocarcinoma | 1.00 | 0.56 | 14.40 | − | − |
| Serous
adenocarcinoma | 2.66 | 1.84 | 33.00 | + | + |
| Mucinous
adenocarcinoma | 1.21 | 2.76 | 22.60 | − | − |
| Endometrioid
adenocarcinoma | 1.55 | 2.39 | 264.5 | − | − |
| Serous borderline
tumor | 1.99 | 2.23 | 58.6 | + | + |
| Clear
adenocarcinoma | 2.22 | 4.02 | 19 | + | + |
| Serous
adenocarcinoma | 2.37 | 2.09 | 91.8 | + | + |
| Serous
adenocarcinoma | 4.76 | 18.67 | 577.3 | + | + |
| Clear
adenocarcinoma | 3.83 | 3.88 | 641.8 | + | + |
| Serous
adenocarcinoma | 1.32 | 1.56 | 565.3 | + | + |
| Mucinous borderline
tumor | 2.54 | 3.32 | 5.1 | − | − |
| Serous
adenocarcinoma | 1.07 | 1.67 | 206.7 | − | − |
| Endometrioid
adenocarcinoma | 1.31 | 2.50 | 80.2 | − | − |
ERC/mesothelin expression observed by
immunohistochemical staining
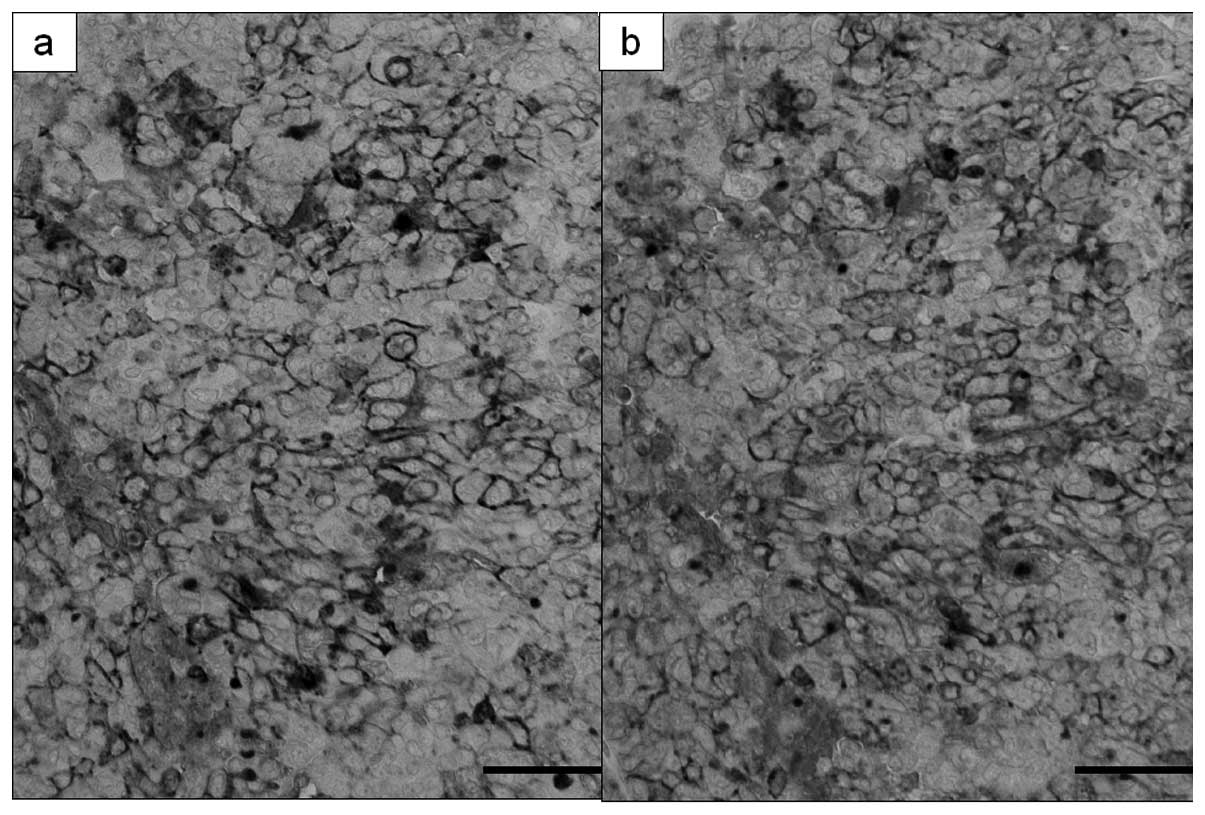
Of the 20 ovarian tumor (carcinoma and borderline
tumor) specimens evaluated for serum N-ERC/mesothelin, 9 (45.0%)
were positive for C-ERC/mesothelin while the remaining 11 (55.0%)
were negative. Of the 18 ovarian carcinoma specimens, 8 (44.4%)
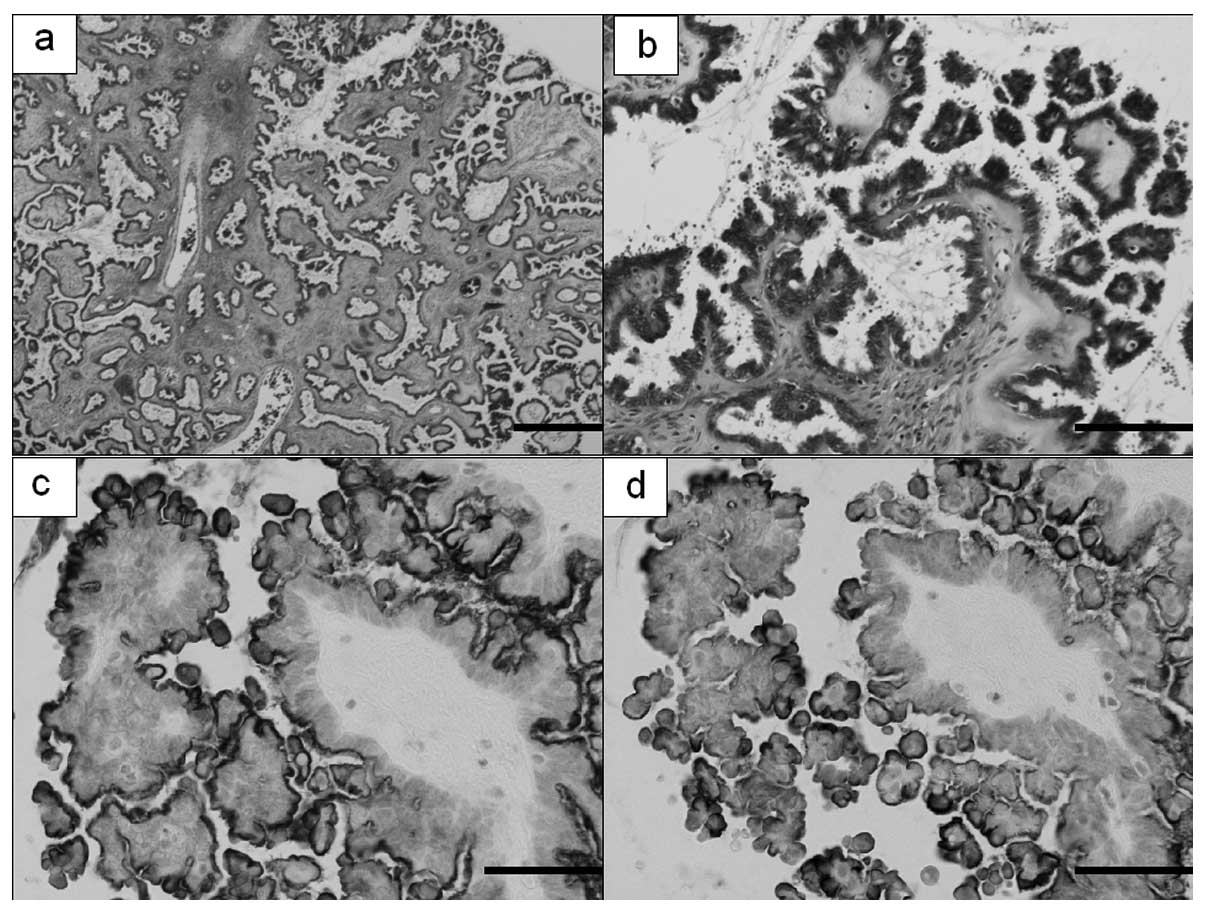
were positive for C-ERC/mesothelin (Fig. 1). Of the 2 borderline tumor
specimens, the serous borderline tumor was positive for
C-ERC/mesothelin on the luminal side of the cell membrane of the
tumor while the mucinous borderline tumor was negative (Fig. 2). When cases positive for
C-ERC/mesothelin were sorted by tissue type, 5 of the 7 serous
adenocarcinoma cases (71.4%) and 3 of the 6 clear cell
adenocarcinoma cases (50.0%) were positive, whereas 1 mucinous
adenocarcinoma and 4 endometrioid adenocarcinoma cases were
negative. Thus, when sorted by tissue type, ovarian carcinomas that
were immunohistochemically C-ERC/mesothelin-positive were found to
be serous and clear cell adenocarcinomas. The tissue specimen of
one patient with serous adenocarcinoma, who had increased serum
N-ERC/mesothelin levels, was also positive for C-ERC/mesothelin. Of
the 10 cases that were immunohistochemically
C-ERC/mesothelin-positive, 1 (10%) had increased serum
N-ERC/mesothelin levels. The cell membranes of all the positive
cases were stained and no difference was found in stainability
between those with increased serum N-ERC/mesothelin levels and
those with constant levels.
A case of serous adenocarcinoma in which
serum N-ERC/mesothelin levels increased
The patient with ovarian carcinoma whose serum
N-ERC/mesothelin levels increased presented with a sense of
abdominal fullness. An exploratory laparotomy was performed due to
the presence of a pelvic tumor and a large amount of ascites. On
surgery, it was found that the tumor had spread in and around both
ovaries in the pelvic cavity, resulting in the adhesion of the
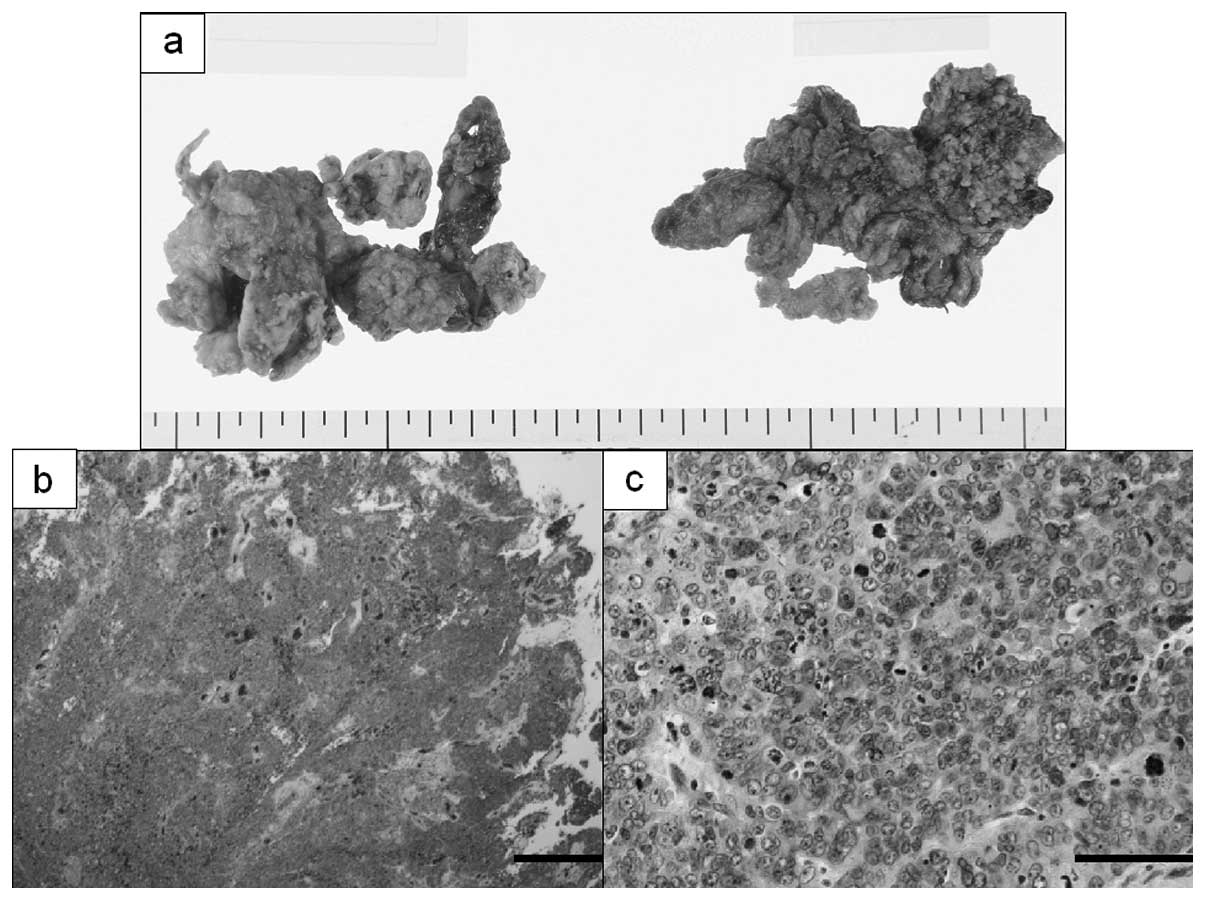
bilateral ovaries to the surrounding organs. The bilateral ovarian
tumor and greater omentum were extirpated. The resected bilateral
ovaries had collapsed, and hence the nature of the tumor was
unclear, but it was solid and partly cystic (Fig. 3). Histologically, atypia and mitotic
figures were predominant and neoplastic cells containing large
nuclei were found to be mixed with multi-nucleated giant cells.
Some neoplastic cells were found to be growing solidly, forming
cysts in places, while others were found to be growing in partial
papillary and tubular patterns. Immunohistochemical staining
revealed that the neoplastic cells were AE1/AE3-positive and
vimentin/calretinin-negative. Subsequently, the patient was
diagnosed with serous adenocarcinoma. Similar invasion by
adenocarcinoma cells was also observed in the greater omentum.
After the ovarian tumor was removed, 6 cycles of chemotherapy were
administered for residual lesions in the pelvic and peritoneal
cavities.
After surgery and chemotherapy, imaging demonstrated
that the tumor had disappeared and serum N-ERC/mesothelin levels
decreased [N(7-4) = 2.00 ng/ml, N(7-16) = 2.50 ng/ml and CA125 =
5.2 U/ml; Table II]. Subsequently,
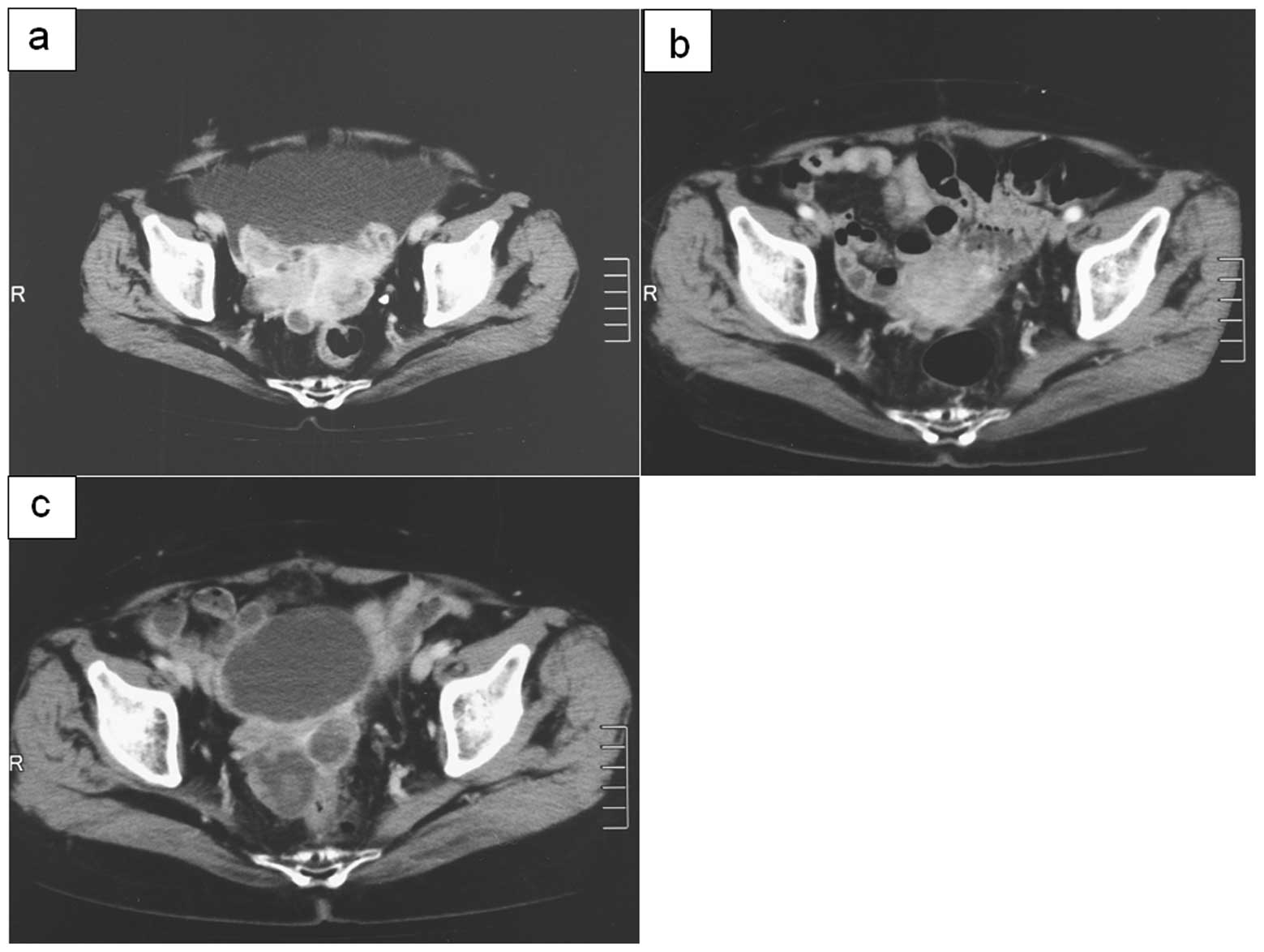
the wait and see approach was adopted and blood tests performed 6
months after the end of chemotherapy revealed increased serum
N-ERC/mesothelin levels and CA125 [N(7-4) = 3.33 ng/ml, N(7-16) =
9.95 ng/ml and CA125 = 108.5 U/ml]. Furthermore, imaging revealed
an enlarged tumor in the peritoneal cavity (Fig. 4). It was determined to be a
recurrence and chemotherapy was initiated again. After 4 cycles of
chemotherapy, serum N-ERC/mesothelin and CA125 levels increased
further [N(7-4) = 5.00 ng/ml, N(7-16) = 26.80 ng/ml and CA125 =
303.7 U/ml] and imaging revealed an enlarged tumor. These results
were consistent with the clinical course.
| Table II.Change in serum ERC/mesothelin levels
in serous adenocarcinoma. |
Table II.
Change in serum ERC/mesothelin levels
in serous adenocarcinoma.
| Marker | Prior to surgery or
chemotherapy | Following surgery
or chemotherapy | 6 months after
chemotherapy | Following 4 cycles
of chemotherapy |
|---|
| N(7-4), ng/ml | 4.76 | 2.00 | 3.33 | 5.00 |
| N(7-16), ng/ml | 18.67 | 2.50 | 9.95 | 26.80 |
| CA125, U/ml | 577.3 | 5.2 | 108.5 | 303.7 |
Discussion
In clinical practice, measuring tumor markers is an
important method to detect tumors and monitor therapeutic effects.
For ovarian carcinoma, CA125, CA19-9 and CEA are the most commonly
used markers. However, these tumor markers have low specificity and
their levels may increase due to adenocarcinomas in other organs or
ascites. ERC/mesothelin, a protein that is expressed by mesothelial
cells, has been found not only in mesothelioma but also in ovarian
carcinoma (4). We examined the
serum of patients with ovarian carcinoma and measured
N-ERC/mesothelin expression in neoplastic cells by ELISA. Of the 32
patients with ovarian tumor, one showed increased serum
ERC/mesothelin levels. In a study conducted by Hassan et al,
an increase in serum C-ERC/mesothelin levels was observed in 67% of
patients with ovarian carcinoma (7), markedly higher than the percentage
obtained in our study. We determined serum N-ERC/mesothelin levels
using ELISA. Further studies are required to investigate the
difference between these positive rates.
In the present study, the serous adenocarcinoma
which was associated with increased serum N-ERC/mesothelin levels
severely adhered to the periovular organs and its shape was
ill-defined. Histologically, the tumor had spread from the ovaries
and the neoplastic cells grew solidly in a papillary pattern. It is
often necessary to differentiate advanced ovarian carcinoma from
Fallopian tube and peritoneal carcinomas. Although the carcinoma in
question, with macroscopically ill-defined ovary shapes, had to be
differentiated from the other carcinomas, the tumor was most
predominant in the ovaries and neoplastic cells were present in the
ovarian parenchyma. Immunohistochemically, the tumor was
AE1/AE3-positive and vimentin/calretinin-negative. Cytologically,
no definite difference from other serous adenocarcinomas was
observed. Immunohistochemical staining for C-ERC/mesothelin in
various ovarian tumors resulted in the neoplastic cell membranes
being stained in every C-ERC/mesothelin-positive case. Every
ovarian carcinoma with a positive result was either serous or clear
cell adenocarcinoma. Serous adenocarcinoma was once considered to
be a de novo carcinoma developing directly from the surface
epithelium or inclusion cysts. However, the disease is currently
considered to be of 2 types, one being adenocarcinoma with
low-grade atypia in which a serous borderline tumor transforms as a
result of malignant progression, and the other being adenocarcinoma
with high-grade atypia emerging from de novo carcinogenesis.
In addition, it has been suggested that certain cases belonging to
the latter type involve adenocarcinoma developing in the distal
Fallopian tube and spreading to the ovaries and pelvic cavity
(9). As ERC/mesothelin is a protein
which is expressed on mesothelial cells, it may be surmised that
C-ERC/mesothelin emerging directly from the surface epithelia of
the ovaries has its origin in serous adenocarcinoma. We found that
C-ERC/mesothelin in serous borderline tumors was expressed not
circumferentially, but on the luminal side of the neoplastic cell
membranes. The mucinous tumor, despite being another variety of
borderline tumor, was negative for C-ERC/mesothelin.
It has been suggested that ovarian endometriosis is
the origin of clear cell adenocarcinomas since one is frequently
concomitant with the other (10).
However, it should be noted that we found C-ERC/mesothelin
expressed in clear cell adenocarcinoma, but not in endometrioid
adenocarcinoma, while ovarian endometriosis is suspected to be the
origin of both. As we used a cut-off value of C-ERC/mesothelin
expression of at least 30% of tumor cells to define tumor
ERC/mesothelin positivity, some of the ERC/mesothelin-negative
tumors could have weak or partial ERC/mesothelin expression
(7). Studies have been conducted on
serum ERC/mesothelin levels in patients with ovarian carcinoma
(4,7,11), but
none have sorted ovarian carcinomas by tissue type. Our finding
that C-ERC/mesothelin was expressed in 2 different tissue types of
carcinoma, the causes of which also appeared to differ, is valuable
in clarifying the histogenesis of ovarian carcinoma. Further
investigation into the various tissue types of ovarian carcinoma is
needed to understand the etiological differences between the types
and their correlation with ERC/mesothelin expression.
We found no clear difference in stainability between
serous adenocarcinoma cases with increased serum N-ERC/mesothelin
levels and those with constant levels. The difference in serum
N-ERC/mesothelin levels, despite their identical C-ERC/mesothelin
expression on the cell surfaces, may be attributed to the size of
the proteins degraded by protease in serum or the presence and size
of the lesions of the peritoneal cavity. The 8 other ovarian
carcinomas had extraovarian lesions but did not increase the serum
N-ERC/mesothelin levels. We measured the N(7-4) and N(7-16) levels
for N-ERC/mesothelin. In serous adenocarcinoma N(7-16) levels
increased more markedly than N(7-4) levels. We used a cut-off value
established by serum N-ERC/mesothelin levels in healthy individuals
and patients with mesothelioma, but the validity of using the same
value for patients with ovarian carcinoma is not certain. Further
studies with larger sample sizes are required.
It has been reported that blood N-ERC/mesothelin
levels are useful for the early detection of mesothelioma and
postoperative monitoring for its recurrence (3).
In a case of ovarian serous adenocarcinoma, we found
increased serum N-ERC/mesothelin levels and changes corresponding
to therapeutic effects. If serum N-ERC/mesothelin, which is
considered useful for early detection in and therapeutic monitoring
of patients with mesothelioma, may also be used for ovarian
carcinoma monitoring, it may be a valuable serum tumor marker for
the early detection of ovarian carcinoma.
Acknowledgements
We thank Masaaki Abe, Naoko Aoki and
Tetsuya Okazaki for assistance with the management of this
study.
References
|
1.
|
K ShiomiH MiyamotoT SegawaNovel ELISA
system for detection of N-ERC/mesothelin in the sera of
mesothelioma patientsCancer
Sci97928932200610.1111/j.1349-7006.2006.00246.x16776777
|
|
2.
|
K ShiomiY HagiwaraK SonoueSensitive and
specific new enzyme-linked immunosorbent assay for N-ERC/mesothelin
increases its potential as a useful serum tumor marker for
mesotheliomaClin Cancer
Res1414311437200810.1158/1078-0432.CCR-07-161318316566
|
|
3.
|
K ImashimizuK ShiomiM MaedaFeasibility of
large-scale screening using N-ERC/mesothelin levels in the blood
for the early diagnosis of malignant mesotheliomaExp Ther
Med2409411201122977518
|
|
4.
|
M HoR HassanJ ZhangQ WangM OndaT BeraI
PastanHumoral immune response to mesothelin in mesothelioma and
ovarian cancer patientsClin Cancer
Res1138143820200510.1158/1078-0432.CCR-04-230415897581
|
|
5.
|
O HinoE KobayashiM NishizawaRenal
carcinogenesis in the Eker ratJ Cancer Res Clin
Oncol121602605199510.1007/BF011977777559744
|
|
6.
|
R HassanT BeraI PastanMesothelin: a new
target for immunotherapyClin Cancer
Res1039373942200410.1158/1078-0432.CCR-03-080115217923
|
|
7.
|
R HassanAT RemaleyML SampsonDetection and
quantitation of serum mesothelin, a tumor marker for patients with
mesothelioma and ovarian cancerClin Cancer
Res12447453200610.1158/1078-0432.CCR-05-147716428485
|
|
8.
|
K IshikawaT SegawaY HagiwaraM MaedaM AbeO
HinoEstablishment of novel mAb to human ERC/mesothelin useful for
study and diagnosis of ERC/mesothelin-expressing cancersPathol
Int59161166200910.1111/j.1440-1827.2009.02344.x19261093
|
|
9.
|
RJ KurmanIM ShinThe origin and
pathogenesis of epithelial ovarian cancer: a proposed unifying
theoryAm J Surg
Pathol34433443201010.1097/PAS.0b013e3181cf3d7920154587
|
|
10.
|
RE ScullyJF Barlow“Mesonephroma” of ovary.
Tumor of Müllerian nature related to the endometrioid
carcinomaCancer20140514171967
|
|
11.
|
I HellstromJ RaycraftS KananNY SardesaiT
VerchY YangKE HellstromMesothelin variant 1 is released from tumor
cells as a diagnostic markerCancer Epidemiol Biomarker
Prev1510141020200610.1158/1055-9965.EPI-05-033416702385
|