Introduction
Although the involvement of the oestrogen receptor
(ER) and progesterone receptor (PR) in breast cancer development
and growth is well-established, little is known about the relevance
and correlation of steroid hormone receptors with other members of
the related non-steroidal nuclear receptor family. The latter is
divided into two subfamilies (1),
the first including the oestrogen, androgen, progesterone and
mineralocorticoid receptors and the second including the thyroid
receptor (TR), vitamin D receptor (VDR), retinoic acid receptor
(RAR), peroxisome proliferator-activated receptor (PPAR) and
retinoid X receptor (RXR). The second group of receptors is able to
form heterodimers with each other, function through appropriate
ligands (2) and interact at the
genetic level (3).
The immunohistochemical expression of these
receptors in breast cancer cells is known (4) and their expression levels are higher
than in normal breast tissue or benign breast lesions (5–8).
The hormone dependency of the mammary gland and the
similarity of TR and ER/PR have led to the hypothesis that TR may
be a prognostic marker in breast cancer patients (9). The ER has two isoforms (α and β),
which are differentiated by their molecular construction yet
identical in their basic effect (10). In this study, which focuses on ER
detected at the time of first diagnosis of breast cancer, ER
isoform α expression was measured since this is the main isoform
for which the most authentic histopathological data have been shown
in previous studies (11). PR was
also detected at the time of the first breast cancer diagnosis.
In the case of the TRs, immunohistochemical staining
of the best known isoforms was conducted. The three main isoforms
are TRα1, TRα2 and TRβ1 (12),
which show high homology in amino acid composition.
Synthetic ligands of RXR have been reported to
induce arrest of growth and differentiation in breast cancer cells
in vitro and in animal models (13,14).
Ligand activation of RXR and PPAR induces antitumour effects in
breast cancer cells (15). For RXR,
three isoforms exist (α, β and γ). The best data on their detection
in malignant breast tumours are available for RXRα (8). For PPAR, most studies refer to the γ
isoform (13,16).
VDR is expressed in epithelial, stromal and immune
cells of the normal mammary gland and is dynamically regulated in
the epithelial compartment during hormonal changes (17). Furthermore, the receptor exists in
malignant dividing cell types which respond to 1,25 vitamin D3
(18).
The present study is an evaluation of the potential
correlations among different steroid hormone receptors following
their immunohistochemical detection.
Materials and methods
Patients and ethics
Patients with an initial diagnosis of anamnestic
sporadic breast cancer who received treatment in the Department of
Obstetrics and Gynaecology of the Ludwig-Maximilians-University
(Munich, Germany) and whose tissue samples were obtained at the
surgery in our institution between 1990 and 2000 were included.
Patients were stratified into groups according to lymph node
involvement, grading and histopathological type, as described
previously (19).
Ethical approval was obtained from the local ethics
committee at the University of Munich (Project No. 048-08). The
participants provided written informed consent. The study was
carried out according to the guidelines of the 1975 Declaration of
Helsinki. All samples and clinical information were used
anonymously.
TNM classification was conducted according to the
WHO criteria (20). The
histological grading classification proposed by Bloom and
Richardson was determined according to a modification of the Elston
and Ellis grading system (21).
Further clinical and histopathological parameters collected
included age, year of breast cancer diagnosis, tumour size,
histopathological type, axillary node involvement, histological
grading and oestrogen/progesterone receptor status. At the time of
the tissue extraction, Her-2/neu was not regularly investigated in
Germany. As far as possible, it has now been determined for the
existing slides. Values of 0 and 1 were considered to be negative,
values of 3+ were classified as positive and in cases of 2+, a
fluorescence in situ hybridisation (FISH) assay was
performed.
Histological diagnostic evaluation and staging were
performed by two experienced gynecologic pathologists.
Clinical data on the patients’ diseases were
available from patients’ charts, aftercare files and tumour
registry database information.
Immunohistochemistry
Immunohistochemistry was performed using a
combination of pressure cooker heating and the standard
streptavidin-biotin-peroxidase complex with the use of the
mouse/rabbit-IgG-Vectastain Elite ABC kit (Vector Laboratories,
Burlingame, CA, USA). The antibodies used for staining are listed
in Table I.
 | Table I.Antibodies and working
concentrations. |
Table I.
Antibodies and working
concentrations.
| Antibody | Species
isotype | Working
dilution | Source |
|---|
| TRα1/2 | Polyclonal rabbit
IgG | 1:200 | Abcam, Cambridge,
MA, USA |
| TRα1 | Polyclonal rabbit
IgG | 1:1000 | AbD Serotec Oxford,
UK |
| TRα2 | Monoclonal rabbit
IgG1 | 1:200 | AbD Serotec,
Oxford, UK |
| TRβ1/2 | Polyclonal rabbit
IgG | 1:200 | Zytomed, Berlin,
Germany |
| TRβ1 | Polyclonal rabbit
IgG | 1:200 | Millipore,
Schwalbach, Germany |
| TRβ2 | Polyclonal rabbit
IgG | 1:100 | Millipore,
Schwalbach, Germany |
| RXRα | Mouse monoclonal
IgG | 1:150 | Perseus Proteomics
Inc., Tokyo, Japan |
| PPARγ | Rabbit polyclonal
IgG | 1:1000 | Abcam, Cambridge,
MA, USA |
| VDR | Mouse monoclonal
IgG2a | 1:100 | AbD Serotec,
Oxford, UK |
Briefly, paraffin-fixed tissue sections were dewaxed
with xylol for 15 min and then rehydrated in descending
concentrations of alcohol (100, 75 and 50%). Endogenous peroxidase
activity was quenched by dipping the slides into 3% hydrogen
peroxide (Merck, Darmstadt, Germany) in methanol for 20 min. For
epitope retrieval, the sections were then incubated in a pressure
cooker using sodium citrate buffer (pH 6.0) containing 0.1 M citric
acid and 0.1 M sodium citrate in distilled water for 10 min. After
cooling, the slides were washed in phosphate-buffered saline (PBS)
twice. Non-specific binding of the primary antibodies was blocked
by incubating the sections with diluted normal serum (10 ml PBS
containing 150 μl horse/goat serum and 50 μl
secondary antibody; Vector Laboratories) for 20 min at room
temperature. Sections were incubated in diluted biotinylated
secondary antibody (10 ml PBS containing 150 μl horse/goat
serum and some secondary antibody; Vector Laboratories) for 30 min
and the avidin-biotin peroxidase complex (diluted in 10 ml PBS;
Vector Laboratories) for 30 min. Visualisation was performed using
the substrate and the chromogen 3,3′-diaminobenzidine (DAB; Dako,
Glostrup, Denmark). Sections were counterstained with Mayer’s
acidic haematoxylin, dehydrated in an ascending series of alcohol
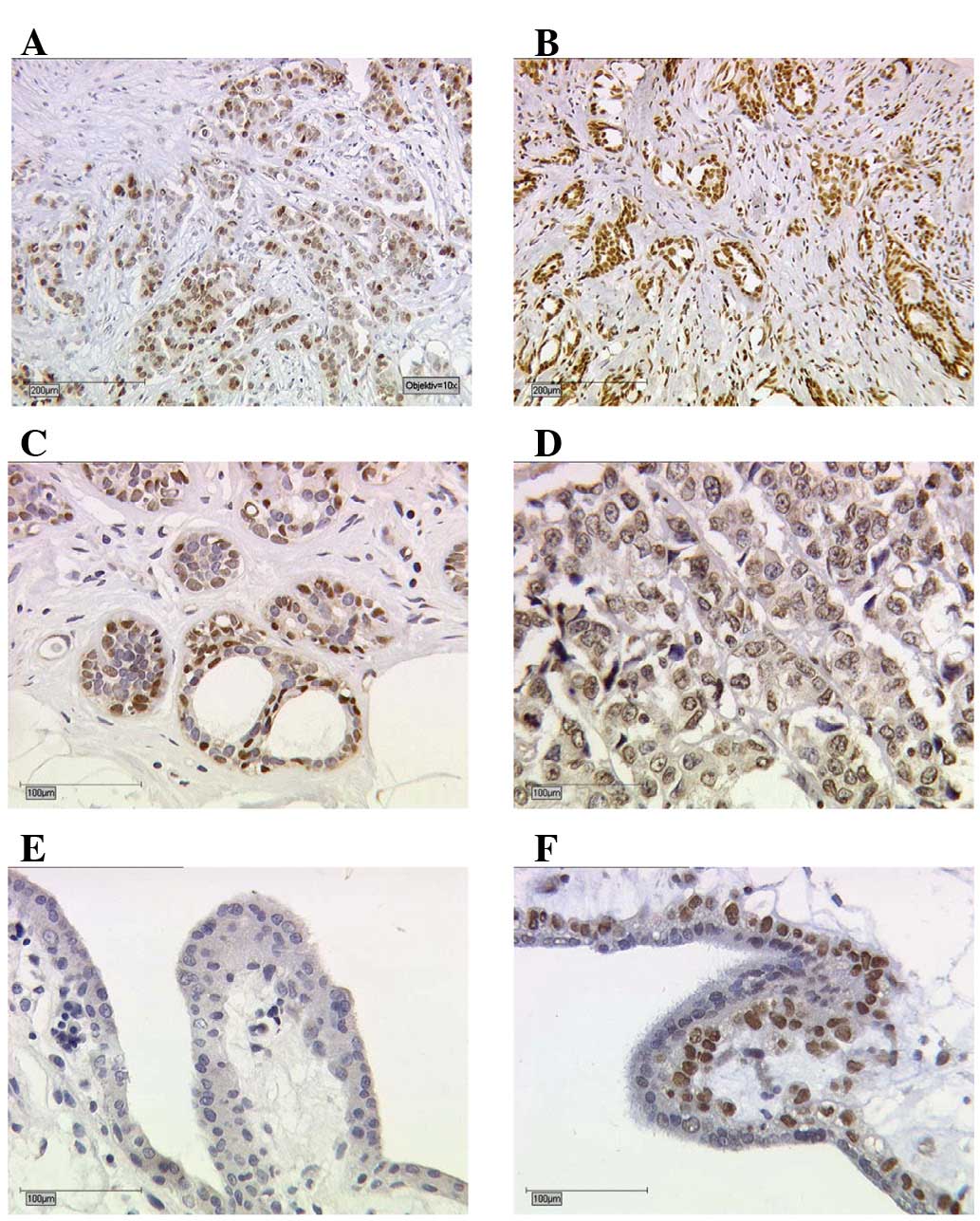
concentrations and then covered. The determination of the different
receptors is shown in Fig. 1A–D.
Negative and positive controls (placental tissue) were used to
assess the specificity of the immunoreactions. For negative
controls (coloured blue), isotype-matched control antibodies of the
same species (Dako, Hamburg, Germany) were applied to the breast
cancer tissue. The control tissue showed neither nuclear nor
cytoplasmic staining. Negative controls and unstained cells were
blue (Fig. 1E). Positive cells were
brown (Fig. 1F).
Slides were evaluated and digitalised with a Zeiss
photomicroscope (Axiophot; AxioCam, Zeiss, Jena, Germany). The
immunoreactive score (IRS) was assigned according to Remmele and
Stegner (22). The intensity and
distribution patterns of specific immunohistochemical staining were
evaluated using the semi-quantitative assay (23,24).
The IRS score was calculated by multiplying the optical staining
intensity (graded as 0, no staining; 1, weak staining; 2, moderate
staining; 3, strong staining) with the percentage of positively
stained cells (0, no staining; 1, <10% of cells stained; 2,
11–50% of cells stained; 3, 51–80% of cells stained; 4, >81% of
cells stained). Microscopic analysis was performed by two
independent observers.
Statistical analysis
Statistical analysis was performed using SPSS
version 19.0 (PASW Statistics; SPSS Inc., IBM, Chicago, IL, USA).
Correlation analysis of the receptor expression was performed using
the non-parametric Mann-Whitney U test and the non-parametric
Spearman’s rho. All statistical tests were two-sided and P<0.05
was considered to indicate a statistically significant result.
Results
Patient characteristics
The paraffin-embedded tissues of 82 patients were
available for analyses. The age at primary diagnosis ranged from
54–95 years. All patients had received an initial diagnosis of
breast cancer and had an invasive ductal histopathological type.
Patient characteristics are detailed in Table II.
| Table II.Baseline characteristics of
participants. |
Table II.
Baseline characteristics of
participants.
| Factor | n | % |
|---|
| Tumour size | 82 | 100 |
| pT1a | 1 | 1 |
| pT1b | 15 | 18 |
| pT1c | 44 | 54 |
| pT2 | 17 | 21 |
| pT3 | - | - |
| pT4 | 5 | 6 |
| LNI | 82 | 100 |
| Yes | 38 | 46 |
| No | 44 | 54 |
| Grading | 82 | 100 |
| 1 | 9 | 11 |
| 2 | 40 | 49 |
| 3 | 33 | 40 |
| TR | 82 | 100 |
| α1/2 | 78 | 95 |
| α1 | 78 | 95 |
| α2 | 79 | 96 |
| β1/2 | 77 | 94 |
| β1 | 79 | 96 |
| β2 | 76 | 93 |
| RXRα | 78 | 95 |
| PPARγ | 78 | 95 |
| VDR | 75 | 91 |
The detection of TR, RXR and PPAR expression was
limited to the nuclei. However, VDR expression was also found in
the cytoplasm of the tumours (Fig.
1A–D). Positive immunohistochemical results (Table III) and correlations with known
histopathological markers were identified (Table IV).
| Table III.Immunohistochemical staining results
of all receptors. |
Table III.
Immunohistochemical staining results
of all receptors.
| Antigen | IRS negative
(0–1)
n (%) | IRS positive
(2–12)
n (%) |
|---|
| TR | | |
| α1 | 23 (29) | 55 (71) |
| α2 | 25 (32) | 54 (78) |
| α1/2 | 59 (76) | 19 (24) |
| β1 | 36 (46) | 43 (54) |
| β2 | 16 (21) | 60 (79) |
| β1/2 | 44 (57) | 33 (43) |
| RXRα | 11 (14) | 74 (86) |
| PPARγ | 33 (42) | 45 (58) |
| VDR | 6 (8) | 89 (92) |
| Table IV.Correlations of antibodies with
histopathological data. |
Table IV.
Correlations of antibodies with
histopathological data.
| Antigen | Tumour size
(pT) | LNI | Differentiation
grade | ER/PR | Her-2/neu |
|---|
| TRα1/2 | ns | ns | ns | ns | ns |
| TRα1 | cc=−0.357,
P=0.001 | ns | ns | ns | ns |
| TRα2 | cc=−0.329,
P=0.003 | cc=−0.487,
P=0.002 | cc=−0.542,
P=0.009 | cc=0.248,
P=0.028 | ns |
| TRβ1/2 | ns | ns | ns | cc=−0.349,
P=0.002 | ns |
| TRβ1 | cc=−0.293,
P=0.009 | ns | ns | cc=0.252,
P=0.025 | ns |
| TRβ2 | cc=−0.314,
P=0.006 | ns | ns | ns | ns |
| RXRα | ns | ns | cc=−0.248,
P=0.029 | ns | ns |
| PPARγ | ns | cc=0.318,
P=0.005 | cc=0.225,
P=0.047 | ns | ns |
| VDR | cc=−0.278,
P=0.016 | cc=0.411,
P<0.01 | ns | ns | ns |
The results of the single TRα1/2 antibodies with a
median IRS of 4 (range, 0–12) differed from the combined antibody
TRα1/2. For TRα1/2, the IRS median was 0 (range, 0–6).
As for TRα1/2, the median IRS values of the
individual TRβ1 and TRβ2 antibodies were higher with values of 2
and 3, respectively (range, 0–12). The TRβ1/2 results were
comparable to those for TRα1/2 with a median IRS of 1 (range,
0–9).
For RXR, the median IRS value was 4 (range, 0–8) and
for PPAR it was 2 (range, 0–12). VDR showed the highest value with
an IRS of 8 (range, 0–12).
Correlation analysis among the
histopathological parameters
Tumour size, lymph node involvement and grading were
significantly correlated with each other (data not shown). ER/PR
had no significant associations with tumour size, lymph node
involvement or grading.
Correlation analysis of steroid family
members with histopathological findings
Tumour size. Tumour size was negatively
correlated with TRα1 [correlation coefficient (cc)= −0.357,
P=0.001], TRα2 (cc=−0.329, P=0.003), TRβ1 and TRβ2 expression
(cc=−0.293, P= 0.009; cc= −0.314, P= 0.006). TRα2 levels were
higher in pT1 tumours (median IRS, 6) compared with pT2-4 tumours
(P=0.024; Fig. 2). RXR and PPAR
were not associated with tumour size. In correlation analyses, VDR
was negatively associated with tumour size (cc=−0.278,
P=0.016).
Axillary lymph node involvement. Lymph node
involvement was negatively correlated with TRα2 (cc=−0.487,
P=0.002) and VDR (cc=−0.411, P<0.01). However, only PPARγ had a
positive significant correlation with lymph node involvement
(cc=0.318, P=0.005).
Differentiation grading. Differentiation
grading was negatively correlated with TRα2 (cc=−0.542, P=0.009)
and RXRγ (cc=−0.248, P=0.029). Positive correlations of grading
were only observed with PPARγ (cc=0.236, P=0.038).
Furthermore, the correlation analysis of ER/PR
expression (data shown in Table IV)
showed positive results for TRα2 expression in the tumours
(cc=0.248, P=0.028) and also for TRβ1 (cc=0.252, P=0.025). A
negative correlation was found between TRβ1/2 expression and ER/PR
expression (cc=−0.349, P=0.002). For RXR, PPAR and VDR, the
correlation analysis showed no significant values for ER/PR
expression.
Her-2/neu. As determined by retrospective
analyses, most patients had a negative Her-2 status (60/82, 80%).
In 7 patients it was not possible to determine Her-2 expression. No
significant correlations were demonstrated with other
clinicopathological parameters (Table
IV).
Correlations among the members of the steroid
hormone receptor family. The results of the correlations among
the single functionally related steroid hormone receptors are
listed in detail in Table V.
| Table V.Correlations among TR, RXR, PPAR and
VDR antibodies. |
Table V.
Correlations among TR, RXR, PPAR and
VDR antibodies.
| Antigen | TRα1/2 | TRα1 | TRα2 | TRβ1/2 | TRβ1 | TRβ2 | RXRα | PPARγ | VDR |
|---|
| TRα1/2 | - | cc=0.300
P=0.009 | ns | ns | cc=0.247
P=0.032 | cc=0.287
P=0.014 | cc=0.274
P=0.018 | ns | ns |
| TRα1 | cc=0.300
P=0.009 | - | ns | ns | ns | cc=0.291
P=0.013 | cc=0.399
P=0.000 | ns | ns |
| TRα2 | ns | ns | - | ns | ns | cc=0.282
P=0.014 | cc=0.316
P=0.006 | ns | cc=0.433
P=0.000 |
| TRβ1/2 | ns | ns | ns | - | ns | ns | ns | ns | ns |
| TRβ1 | cc=0.247
P=0.032 | ns | ns | ns | - | cc=0.557
P=0.000 | ns | cc=0.270
P=0.017 | cc=0.403
P=0.000 |
| TRβ2 | cc=0.287
P=0.014 | cc=0.291
P=0.013 | cc=0.282
P=0.014 | ns | cc=0.557
P=0.000 | - | ns | cc=0.458
P=0.000 | cc=0.370
P=0.001 |
| RXRα | cc=0.274
P=0.018 | cc=0.399
P=0.000 | cc=0.316
P=0.006 | ns | ns | ns | - | ns | ns |
| PPARγ | ns | ns | ns | ns | cc=0.270
P=0.017 | cc=0.458
P=0.000 | ns | - | ns |
| VDR | ns | ns | cc=0.433
P=0.000 | ns | cc=0.403
P=0.000 | cc=0.370
P=0.001 | ns | ns | - |
Thyroid receptors. For the combined TRα1/2, a
correlation was demonstrated with TRα1, TRβ1, TRβ2 and RXR. TRα1
expression was correlated with TRα1/2, TRβ2 and RXR. TRα2 showed
positive correlations with TRβ2, RXR and VDR. No correlations with
other steroid factors were found for TRβ1/2. TRβ1 correlated
positively with TRβ2, PPAR and VDR. TRβ2 showed positive
correlations with almost all receptors (TRα1/2, TRα1, TRα2, TRβ1,
PPAR and VDR).
RXR. RXRα was positively correlated with
TRα1, TRα2 and TRα1/2.
PPAR. PPARγ showed two correlations, with
TRβ1 and TRβ2.
VDR. For VDR, significant correlations were
demonstrated with TRα2, TRβ1 and TRβ2.
Discussion
The present study demonstrated significant
correlations between the known histopathological parameters,
including tumour size, lymph node involvement, differentiation
grade, ER, PR and other members of the nuclear receptor family.
Furthermore, significant correlations among different steroid
receptors (excluding the combined TRβ1/2) were shown. To the best
of our knowledge, this is the first study to examine the
coexpression and thus the immunohistochemical correlation between
members of steroid receptors in a cohort of breast cancer
patients.
The rationale for this study was the known
significance of immunohistochemical ER/PR expression in breast
cancer and the similarity of these receptors with the surface of
the other members of the nuclear receptor family. In the latter,
ER/PR detection in breast cancer is associated with prognostic
relevance (25), and it has long
been known that overexpression is treatable with antihormonal
therapy (26), regardless of the
oestrogen and progesterone blood levels.
Certain authors have focused on thyroid receptors
due to an assumed correlation between thyroid dysfunction and
breast cancer (9,27,28).
Few studies have reported clear results demonstrating associations,
although in these studies, TRs and other histopathological findings
were not further differentiated; for example, a negative
correlation between the TR receptor level and the axillary
involvement of lymph nodes (29).
By contrast, Silva et al did not find clear correlations
between single TRβ1 expression and other histopathological factors
(30). The inconsistency between
the results of different TRs may be attributable to different
distributions of the TRs in the examined tissue (certain sections
had mainly mixed epitopes of TRs, while other sections had mainly
single TRs). Taking this into account, as was demonstrated in our
study, clear associations between different TRs and
histopathological findings support the assumption that the
interactions identified may have inherent prognostic relevance.
As with TRs, most of the literature for RXR and PPAR
does not refer to in vivo but in vitro data (31,32).
In our study, the expression of RXR, which is known for its
antitumour effects, was negatively correlated with differentiation
grade (33).
For PPARγ, an inverse association with tumour size
was found (34). In contrast to our
previous findings (35), which
demonstrated a correlation between PPAR and positive lymph node
involvement, discrepant results have also been reported (34). These current conflicting results
need to be resolved in larger trials. Hence, drawing clinical
conclusions from these findings is considered premature at this
time.
In a previous study (36), an immunohistochemical expression of
VDR in most of the tumour cells was shown. Nonetheless, data based
on the correlation between VDR and ER/PR were inconsistent and
contradictory (36–39). Furthermore, the presence of ER/PR
and VDR was only partially correlated with other clinical features
of tumour stage (36).
We cannot underline the finding of a clear
association of VDR and ER/PR but, in contrast to previous findings,
our data demonstrated a correlation between VDR, tumour size and
lymph node involvement. A single study (40) demonstrated a role for vitamin D and
its receptor in breast cancer in humans. As previous data have
shown (41,42), an improved outcome was achieved in
patients with high VDR-IRS than in patients with low IRS. Taken
together, the current findings support the assumption that VDR is a
factor with prognostic relevance in breast cancer.
The immunohistochemical association of these
receptors supports the knowledge of interactions at the molecular
level (43). Hence, these results
await confirmation in larger trials. Unfortunately, HER2/neu status
was not routinely determined in the cohort investigated at the time
of initial diagnosis. Given the high prognostic value of HER2/neu
status, it was of significant interest whether this prognosticator
also interacts with other receptors. Although selection bias cannot
be excluded and the number of patients was small, results may have
significance for malignant breast tumour diseases and may be of
interest for future innovative therapeutic approaches.
We have demonstrated significant correlations for
all the major isoforms of TRs, and furthermore, between RXR, PPAR
and VDR. Significantly, and in contrast to TRβ2, TRα2 demonstrated
significant correlations with each of the known independent
histopathological markers in breast cancer. It was unusual that,
with larger tumour size, higher differentiation grade and axillary
lymph node involvement, TRα2 became negative, but with high ER/PR
values, TR increased. This may lead to the assumption that high
expression, particularly of TRα2, is associated with a better
prognosis at higher values of ER/PR and therefore protects breast
cancer cells from de-differentiation. Furthermore, TRβ2, RXR and
VDR were significantly correlated, the latter two of which are
known to be of prognostic importance in breast cancer.
Acknowledgements
We thank the patients for providing
samples for this study. We acknowledge the excellent technical
assistance of M. Rübekeil, S. Hofmann, S. Kunze and C.H. Kuhn.
References
|
1.
|
H EscrivaS BertrandV LaudetThe evolution
of the nuclear receptor superfamilyEssays Biochem4011262004
|
|
2.
|
M SchräderS NayeriJP KahlenKM MüllerC
CarlbergNatural vitamin D3 response elements formed by inverted
palindromes: polarity-directed ligand sensitivity of vitamin D3
receptor-retinoid X receptor heterodimer-mediated
transactivationMol Cell Biol15115411611995
|
|
3.
|
JH SegarsMS MarksS HirschfeldPH DriggersE
MartinezJF GrippoW WahliK OzatoInhibition of estrogen-responsive
gene activation by the retinoid X receptor beta: evidence for
multiple inhibitory pathwaysMol Cell Biol42258226819938384307
|
|
4.
|
T TanakaBL DanchekLC TrifilettiRE
BirnkrantBJ TaylorSH GarfieldU ThorgeirssonLM De LucaAltered
localization of retinoid X receptor α coincides with loss of
retinoid responsiveness in human breast cancer MDA-MB-231 cellsMol
Cell Biol24397239822004
|
|
5.
|
P TontonozE HuBM SpiegelmanStimulation of
adipogenesis in fibroplasts by PPARγ2, a lipid-activated
transcription factorCell79114711561994
|
|
6.
|
RC SmallridgeKR LathamNuclear thyroid
hormone receptor in human breast tumoursClin Res284211980
|
|
7.
|
M FriedrichR Axt-FliednerC
Villena-HeinsenW TilgenW SchmidtJ ReichrathAnalysis of vitamin
D-receptor (VDR) and retionoid X-receptor α in breast
cancerHistochem J3435402002
|
|
8.
|
I CondeMVT LoboJ ZamoraJ PérezFJ GonzálezE
AlbaB FraileR PaniaguaMI ArenasHuman pregnane X receptor is
espressed in breast carcinomas, potential heterodimers formation
between hPXR and RXR-αBMC Cancer8174200818565212
|
|
9.
|
J LiQ LinHG YoonZQ HuangBD StrahlCD AllisJ
WongInvolvement of histone methylation and phosphorylation in
regulation of transcription by thyroid hormone receptorMol Cell
Biol2256885697200210.1128/MCB.22.16.5688-5697.200212138181
|
|
10.
|
J Carlstedt-DukePE StrömstedtB PerssonE
CederlundJA GustafssonH JörnvallIdentification of
hormone-interacting amino acid residues within the steroid-binding
domain of the glucocorticoid receptor in relation to other steroid
hormone receptorsJ Biol Chem263684268461988
|
|
11.
|
J Carlstedt-DukeCellular estrogen
activity: implications for pulsed estrogen therapyMaturitas38Suppl
1S7S13200110.1016/S0378-5122(01)00199-211390119
|
|
12.
|
Y LingX XuJ HaoX LingX DuX LiuX
ZhaoAberrant methylation of the TRB gene in tissue and plasma of
breast cancer patientsCancer Genet
Cytogenet196140145201010.1016/j.cancergencyto.2009.09.01020082849
|
|
13.
|
E MuellerP SarrafP TontonozRM EvansKJ
MartinM ZhangC FletcherS SingerBM SpiegelmanTerminal
differentiation of human breast cancer through PPARγMol
Cell14654701998
|
|
14.
|
N SuhY WangCR WilliamsR RisingsongT
GilmerTM WillsonMB SpornA new ligand for the peroxisome
proliferator activated receptor gamma (PPARgamma), GW7845, inhibits
rat mammary carcinogenesisCancer Res5956715673199910582681
|
|
15.
|
E ElstnerEA WilliamsonC ZangJ FritzD
HeberM FennerK PossingerHP KoefflerNovel therapeutic approach:
ligands for PPARγ and retinoid receptors induce apoptosis in
bcl-2-positive human breast cancer cellsBreast Cancer Res
Treat741551652002
|
|
16.
|
MW KilgorePL TateS RaiE SengokuTM
PriceMCF-7 and T47 D human breast cancer cells contain a functional
peroxisomal responseMol Cell
Endocrinol129229235199710.1016/S0303-7207(97)04057-49202406
|
|
17.
|
GM ZinserJE WelshAccelerated mammary gland
development during pregnancy and delayed post-lactational
involution in vitamin D3 receptor null miceMol
Endocrinol1822082223200410.1210/me.2003-046915178742
|
|
18.
|
AF GombartQT LuongHP KoefflerVitamin D
compounds: activity against microbes and cancerAnticancer
Res264A25312542200616886661
|
|
19.
|
D DianW JanniC KuhnD MayrU KarstenI
MylonasK FrieseU JeschkeEvaluation of a novel anti-mucin 1 (MUC1)
antibody (PankoMab) as a potential diagnostic tool in human ductal
breast cancer; comparison with two established
antibodiesOnkologie32238244200910.1159/000209280
|
|
20.
|
A FritzC PercyA JackK ShanmugaratnamL
SobinDM ParkinS WhelanInternational Classification of Diseases for
Oncology3rd editionWorld Health OrganizationGeneva2000
|
|
21.
|
EW ElstonIO EllisMethod for grading breast
cancerJ Clin Pathol46189190199310.1136/jcp.46.2.189-b8459046
|
|
22.
|
W RemmeleHE StegnerRecommendation for
uniform definition of an immunoreactive score (IRS) for
immunohistochemical estrogen receptor detection (ER-ICA) in breast
cancer tissuePathologe81381401987(In German)
|
|
23.
|
U JeschkeA BischofR SpeerDevelopment of
monoclonal and polyclonal antibodies and an ELISA for the
determination of glycodelin in human serum, amniotic fluid and
cystic fluid of benign and malignant ovarian tumoursAnticancer
Res25158115892005
|
|
24.
|
I MylonasJ MakovitzkyU JeschkeV BrieseK
FrieseB GerberExpression of Her2/neu, steroid receptors (ER and
PR), Ki67 and p53 in invasive mammary ductal carcinoma associated
with ductal carcinoma in situ (DCIS) versus invasive breast cancer
aloneAnticancer Res2517191723200516033090
|
|
25.
|
WA KnightRB LivingstonEJ GregoryWL
McGuireEstrogen receptor as an independent prognostic factor for
early recurrence in breast cancerCancer Res37466946711977922747
|
|
26.
|
CK OsborneWL McGuireThe use of steroid
hormone receptors in the treatment of human breast cancer: a
reviewBull Cancer662032101979385079
|
|
27.
|
PPA SmythThe thyroid and breast cancer: a
significant association?Ann
Med29189191199710.3109/078538997089993359240623
|
|
28.
|
N DitschS LiebhardtF von KochM LenhardM
VogeserC SpitzwegJ GallwasB TothThyroid function in breast cancer
patientsAnticancer Res3017131717201020592366
|
|
29.
|
M LemaireL Baugnet-MahieuNuclear thyroid
hormone receptors in human cancer tissuesAnticancer
Res669570019863019222
|
|
30.
|
JM SilvaG DomínguezJM González-SanchoJM
GarcíaJ SilvaC García-AndradeA NavarroA MuñozF BonillaExpression of
thyroid hormone receptor/erbA genes is altered in human breast
cancerOncogene2143074316200210.1038/sj.onc.120553412082618
|
|
31.
|
K WuY ZhangXC XuJ HillJ CelestinoHT KimThe
retinoid X receptor-selective retinoid, LGD1069, prevents the
development of estrogen receptor-negative mammary tumours in
transgenic miceCancer Res6263766380200212438218
|
|
32.
|
HP KoefflerPeroxisome
proliferator-activated receptor gamma and cancersClin Cancer
Res919200312538445
|
|
33.
|
D BonofiglioE CioneH QiA PingitoreM PerriS
CatalanoD VizzaML PannoG GenchiSA FuquaS AndoCombined low doses of
PPARgamma and RXR ligands trigger an intrinsic apoptic pathway in
human breast cancer cellsAm J
Pathol17512701280200910.2353/ajpath.2009.08107819644018
|
|
34.
|
T SuzukiS HayashiY MikiY NakamuraT MoriyaA
SugawaraT IshidaN OhuchiH SasanoPeroxisome proliferator-activated
receptor gamma in human breast carcinoma: a modulator of estrogenic
actionsEndocr Relat
Cancer13233250200610.1677/erc.1.0107516601291
|
|
35.
|
N DitschT VrekoussisM LenhardI RühlJ
GallwasT WeissenbacherK FrieseD MayrA MakrigiannakisU
JeschkeRetinoid X receptor alpha (RXRα) and peroxisome
proliferator-activated recptor gamma (PPARγ) expression in breast
cancer: an immunohistochemical studyIn vivo2687922012
|
|
36.
|
U BergerRA McClellandP WilsonGL GreeneMR
HausslerJW PikeK ColstonD EastonRC CoombesImmunocytochemical
determination of estrogen receptor, progesterone receptor, and
1,25-dihydroxyvitamin D3 receptor in breast cancer and relationship
to prognosisCancer Res512392441991
|
|
37.
|
HC FreakeG AbeyasekeraJ IwasakiC MarcocciI
MacIntyreRA McClellandRA SkiltonDF EastonRC CoombesMeasurement of
1,25-dihydroxyvitamin D3 receptors in breast cancer and their
relationship to biochemical and clinical indicesCancer
Res441677168119846322984
|
|
38.
|
BH MasonIM HoldawayPR MullinsLH YeeRG
KayProgesterone and estrogen receptors as prognostic variables in
breast cancerCancer Res432985299019836850609
|
|
39.
|
JM HowatM HarrisR SwindellDM BarnesThe
effect of oestrogen and progesterone receptors on recurrence and
survival in patients with carcinoma of the breastBr J
Cancer51263270198510.1038/bjc.1985.383966982
|
|
40.
|
ML McCulloughRM BostickTL MayoVitamin D
gene pathway polymorphisms and risk of colorectal, breast, and
prostate cancerAnnu Rev
Nutr29111132200910.1146/annurev-nutr-080508-14124819400699
|
|
41.
|
U BergerP WilsonRA McClellandK ColstonMR
HausslerJW PikeRC CoombesImmunocytochemical detection of
1,25-dihydroxyvitamin D3 receptor in breast cancerCancer
Res476793679919872824042
|
|
42.
|
N DitschB TothD MayrM LenhardJ GallwasT
WeissenbacherC DanneckerK FrieseU JeschkeThe association between
vitamin D receptor and prolonged overall survival in breast cancerJ
Histochem Cytochem60121129201210.1369/002215541142915522108646
|
|
43.
|
R Sanchez-MartinezA ZambranoAI CastilloA
ArandaVitamin D-dependent recruitment of corepressors to vitamin
D/retinoid X receptor heterodimersMol Cell
Biol2838173829200710.1128/MCB.01909-0718362166
|