Introduction
Lymphangiogenesis, the formation of new lymphatic
vessels, plays a critical role in the systemic metastasis of
malignant tumors. It is a complicated process tightly regulated by
a variety of direct and indirect growth factors (1,2). With
the discovery of antibodies against lymphatic endothelial cells in
the past decade, lymphangiogenesis has attracted increasing
interest and become a new area of cancer metastasis research.
Lymphangiogenesis has been demonstrated to be associated with lymph
node metastasis and negative prognosis in various types of cancer
(3,4). Lymphoma cells invade the lymph nodes
through the lymphatic vessels. However, few studies have been
performed on lymphangiogenesis and related factors in lymphoma.
Vascular endothelial growth factor-C (VEGF-C) is a
potent inducer of lymphangiogenesis. It is essential in the
formation of the first lymphatic vessel during embryonic
development (5) and in mediating
cancer metastasis through lymphatic vessels (6). VEGF-C promotes lymphangiogenesis by
binding to VEGFR-3, which is expressed on the lymphatic endothelial
cells of adults (6). Cyclooxygenase
(COX) plays an important role in the conversion of arachidonic acid
to prostaglandin. It has two isoforms, COX-1 and COX-2. COX-1
maintains the homeostatic level of prostaglandin (7) and COX-2 is induced by mitogenic or
inflammatory stimuli, including cytokines, growth factors and tumor
promoters (8). Increasing evidence
suggests that COX-2 participates in carcinogenesis and cancer
progression. COX-2 functions through activating carcinogens,
inhibiting apoptosis, promoting angiogenesis, modulating
immunological responses and influencing tumor invasion by
activation of matrix metalloproteinases (MMPs) (9). The correlation between COX-2 and tumor
lymphangiogenesis has been discovered in breast (10), gastric (11), prostate (12) and lung cancer (13), suggesting that COX-2 plays a role in
tumor lymphangiogenesis. However, whether COX-2 expression is
correlated with lymphangiogenesis in lymphoma has not been
reported.
The aims of the current study were to i) investigate
the expression of COX-2 and VEGF-C and lymphangiogenesis in
non-Hodgkin’s lymphoma (NHL) and their correlations with the
clinical features of patients and ii) investigate the correlations
among COX-2, VEGF-C and lymphangiogenesis in NHL.
Materials and methods
Patients and samples
Formalin-fixed and paraffin-embedded tissue blocks
of 75 patients diagnosed with NHL in Qingdao Municipal Hospital
(Qingdao, China) between 2002 and 2010 were used in the current
study. The NHL group included 46 males and 29 females. The median
age was 60.0 years (range, 17–86). The patients’ conditions were
staged according to the Ann Arbor staging system. Samples were
classified according to World Health Organization classification of
lymphomas. Samples were further grouped according to the
aggressiveness of the NHL subtypes. There were 14 cases of indolent
lymphoma (8 cases of small lymphocytic lymphoma, 1 case of
mucosa-associated lymphoid tissue lymphoma, 2 cases of follicular
lymphoma and 3 cases of lymphoplasmacytic lymphoma), 57 cases of
aggressive lymphoma (56 cases of diffuse large B-cell lymphoma and
1 case of extranodal NK/T-cell lymphoma, nasal type) and 4 cases of
very aggressive lymphoma (3 cases of Burkitt lymphoma and 1 case of
T-lymphoblastic lymphoma). Patients with aggressive or very
aggressive lymphoma were grouped as aggressive lymphoma in the
following analyses. Informed consent was obtained from each patient
or the patient’s family for use of the samples. This study was
approved by the local Ethics Committee.
Immunohistochemical staining and
assessment
A total of 75 NHL samples were examined for the
expression of lymph vessel endothelial hyaluronan receptor-1
(LYVE-1), VEGF-C and COX-2. Briefly, sections of 4-μm
thickness were cut from paraffin blocks and mounted on slides
coated with 3-aminopropyl-triethoxysilane (Maxin-bio, Fuzhou,
China). The slides were dewaxed in xylene and rehydrated through a
graded ethanol series. Antigen retrieval was performed by microwave
treatment at 98°C for 10 min in citric buffer (pH 6.0) for LYVE-1
and VEGF-C detection or EDTA (pH 9.0) for COX-2 detection. The
slides were then cooled at room temperature for 30 min. Endogenous
peroxidase activity was blocked by immersion in 3% hydrogen
peroxide for 10 min at room temperature. This was followed by
addition of rabbit anti-COX-2 monoclonal antibody (Maxin-bio,
Fuzhou, China) at a dilution of 1:200, rabbit anti-LYVE-1
polyclonal antibody (Abcam Ltd., Cambridge, UK) at a dilution of
1:200 or rabbit anti-VEGF-C polyclonal antibody (Zhongshan
Goldbridge Biotech, Beijing, China) at a dilution of 1:200. The
slides were then incubated overnight at 4°C. The secondary antibody
of the Maxvision system, peroxidase-labeled polymer conjugated to
anti-rabbit/mouse immunoglobulin antibody (Maxin-bio), was then
applied and incubated at room temperature for 15 min. Subsequently,
the chromogenic substrate 3,3′-diaminobezidine tetrahydrochloride
(DAB, Maxin-bio) was added. Finally, the slides were briefly
counterstained with hematoxylin. PBS was used as a negative control
in place of the primary antibody.
COX-2 staining was considered to be positive when
>20% of the lymphoma cells showed positive cytoplasmic staining.
The definition of positive staining of VEGF-C was immunore-activity
in ≥10% of the lymphoma cells.
VEGF-C expression was evaluated using a scoring
system based on staining intensity and percentage of positive
lymphoma cells. The staining intensity was classified into four
categories: 0, negative; 1, weak; 2, moderate; 3, strong. The score
of a slide was calculated by multiplying the staining intensity by
the percentage of positive lymphoma cells. The median score was
used as the cut-off to divide samples into high and low VEGF-C
expression groups.
Lymphatic vessel density (LVD) was determined using
Weidner’s method (14) with minor
modifications. Any brown-stained endothelial cell or cell cluster
clearly separated from the adjacent cells, tissue elements and
microvessels was considered to be a lymph vessel. The sections were
first scanned at ×100 magnification to identify two regions with
the greatest number of distinct brown staining regions (hot spots).
The two hot spots were then counted at ×200 magnification with a
microscope ocular grid equal to 0.24 mm2 of the
examination area. The median LVD was used as a cut-off to separate
the NHL cases into negative and positive groups. The slides were
reviewed independently by two investigators blinded to clinical
details.
Statistical analysis
The Chi-square test was applied to analyze the
correlations among LVD, COX-2 and VEGF-C and their associations
with the clinical features of the patients. P<0.05 was
considered to indicate a statistically significant result.
Results
Expression of LYVE-1 and its correlation
with clinical variables
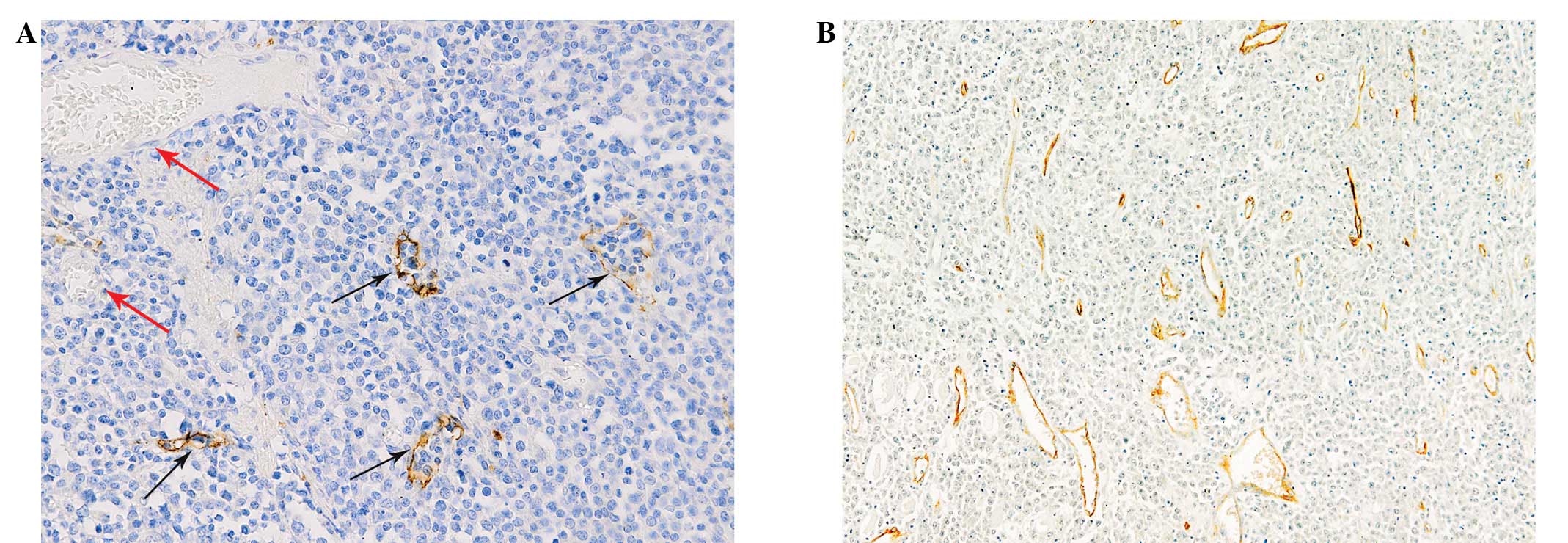
The lymphatic vessels were lined with a single layer
of LYVE-1-positive endothelial cells, while blood vessels
containing red blood cells were negative for LYVE-1 staining
(Fig. 1A). Lymphatic vessels with
open lumina and lymphatic endothelial cells or cell clusters
without a lumen structure were observed (Fig. 1B). The lymphatic vessels were
distributed unevenly throughout the sections investigated. The
median LVD in this study was 5.5 (range, 0–36). There were 40
(53.3%) cases of NHL with a LVD counting greater than or equal to
the median. LVD was positive in 59.0% of the cases with aggressive
morphology, while the LVD positive rate of indolent lymphoma was
only 28.6% (P=0.039). The 5 cases with LVD >25 were all of
aggressive histology. The LVD showed no correlation with the
clinical parameters, including gender, age, lactate dehydrogenase
(LDH) levels, β2 microglobulin (β2M) levels, extranodal
involvement, disease stage, B symptoms and international prognostic
index (IPI; Table I).
 | Table I.Correlation of LVD, COX-2 and VEGF-C
with clinical parameters in NHL. |
Table I.
Correlation of LVD, COX-2 and VEGF-C
with clinical parameters in NHL.
| Clinical
parameters | n | LVD
| P-value | COX-2
| P-value | VEGF-C
| P-value |
|---|
| + | − | + | − | High | Low |
|---|
| Age (years) | | | | | | | | | | |
| <60 | 36 | 17 | 19 | 0.308 | 17 | 19 | 0.308 | 17 | 19 | 0.725 |
| ≥60 | 39 | 23 | 16 | | 23 | 16 | | 20 | 19 | |
| Gender | | | | | | | | | | |
| Male | 46 | 23 | 23 | 0.466 | 24 | 22 | 0.800 | 23 | 23 | 0.884 |
| Female | 29 | 17 | 12 | | 16 | 13 | | 14 | 15 | |
| LDH | | | | | | | | | | |
| Normal | 18 | 9 | 9 | 0.637 | 10 | 8 | 0.930 | 9 | 9 | 0.754 |
| High | 46 | 26 | 20 | | 25 | 21 | | 25 | 21 | |
| β2M | | | | | | | | | | |
| Normal | 20 | 12 | 8 | 0.353 | 13 | 7 | 0.203 | 9 | 11 | 0.406 |
| High | 28 | 13 | 15 | | 13 | 15 | | 16 | 12 | |
| En inv | | | | | | | | | | |
| No | 31 | 16 | 15 | 0.777 | 16 | 15 | 0.777 | 19 | 12 | 0.116 |
| Yes | 40 | 22 | 18 | | 22 | 18 | | 17 | 23 | |
| Stagea | | | | | | | | | | |
| I | 15 | 7 | 8 | 0.737 | 7 | 8 | 0.517 | 5 | 10 | 0.383 |
| II | 18 | 9 | 9 | | 7 | 11 | | 9 | 9 | |
| III | 22 | 11 | 11 | | 11 | 11 | | 10 | 12 | |
| IV | 12 | 8 | 4 | | 8 | 4 | | 8 | 4 | |
| B symptoms | | | | | | | | | | |
| No | 35 | 20 | 15 | 0.893 | 20 | 15 | 0.712 | 16 | 19 | 0.407 |
| Yes | 36 | 20 | 16 | | 19 | 17 | | 20 | 16 | |
| IPI | | | | | | | | | | |
| 0–2 | 46 | 27 | 19 | 0.301 | 25 | 21 | 0.571 | 26 | 20 | 0.378 |
| 3–5 | 16 | 7 | 9 | | 10 | 6 | | 7 | 9 | |
| Histology | | | | | | | | | | |
| Indolent | 14 | 4 | 10 | 0.039b | 5 | 9 | 0.143 | 4 | 10 | 0.085c |
| Aggressive | 61 | 36 | 25 | | 35 | 26 | | 33 | 28 | |
Expression of COX-2 and its correlation
with clinical variables
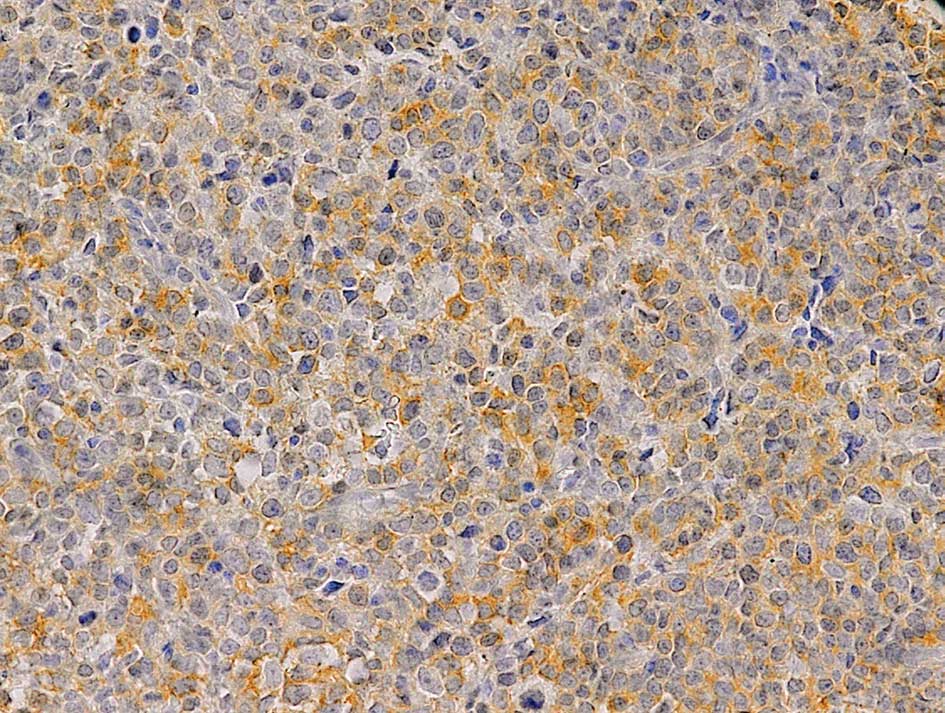
Positive expression of COX-2 was observed in 40
(53.3%) of the NHL samples. COX-2 was expressed in the cytoplasm of
lymphoma cells (Fig. 2). In
addition, inflammatory cells, especially plasma cells, were also
positive for COX-2. COX-2 expression was not correlated with the
gender, age, LDH levels, β2M levels, extranodal involvement,
disease stage, B symptoms or IPI of the patients (Table I). COX-2 expression showed no
difference between the indolent and aggressive subtypes of NHL.
Expression of VEGF-C and its correlation
with clinical variables
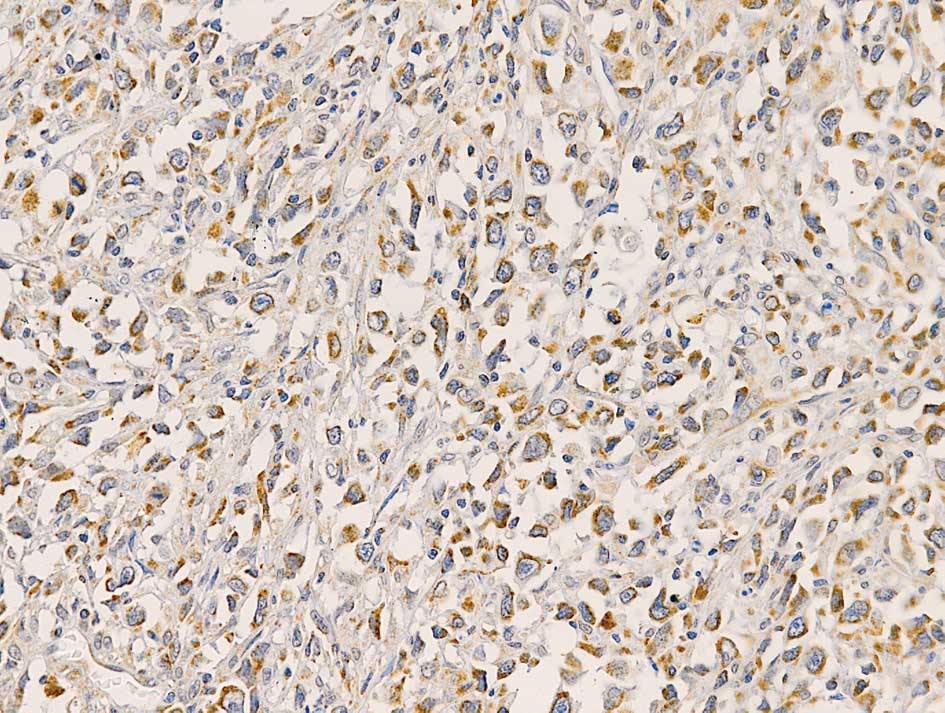
Positive VEGF-C staining was observed in 72 (96%) of
the NHL samples. VEGF-C was expressed in the cytoplasm of lymphoma
cells (Fig. 3). A total of 37
(49.3%) cases were graded as showing high expression and 38 (50.7%)
cases were graded as low expression of VEGF-C. In addition to
lymphoma cells, macrophages and stromal cells positively stained
for VEGF-C were also observed. VEGF-C expression showed a trend of
association with the morphology of NHL (P=0.085), with VEGF-C high
expression rates of 54.1% in aggressive lymphoma and 40% in
indolent lymphoma. VEGF-C expression was not correlated with the
gender, age, LDH levels, β2M levels, extranodal involvement,
disease stage, B symptoms, or IPI of the patients (Table I).
Correlation of COX-2, VEGF-C and LVD
LVD was positive in 65% of cases in the
COX-2-positive group, whereas the LVD positive rate in the
COX-2-negative group was only 40% (P=0.030). The LVD positive rates
in the VEGF-C high and low expression groups were 75.7 and 31.6%,
respectively (P=0.000; Table II).
The expression levels of VEGF-C and COX-2 were significantly
correlated in NHL (P=0.015; Table
III).
| Table II.Correlation of LVD and COX-2 or
VEGF-C in NHL. |
Table II.
Correlation of LVD and COX-2 or
VEGF-C in NHL.
| n | LVD
| P-value |
|---|
| + | − |
|---|
| COX-2 | | | | |
| + | 40 | 26 | 14 | 0.030a |
| − | 35 | 14 | 21 | |
| VEGF-C | | | | |
| + | 37 | 28 | 9 | 0.000a |
| − | 38 | 12 | 26 | |
| Table III.Correlation between COX-2 and VEGF-C
in NHL. |
Table III.
Correlation between COX-2 and VEGF-C
in NHL.
| n | COX-2
| P-value |
|---|
| + | − |
|---|
| VEGF-C | | | | |
| + | 37 | 25 | 12 | 0.015a |
| − | 38 | 15 | 23 | |
Discussion
To date, the lymphangiogenesis in lymphoma has only
been investigated by two studies. Kadowaki et al showed that
LVD in lymphoma was significantly higher than that in non-reactive
normal lymph node (15). Wróel
et al showed that lymphatic sinus density (LSD) was not
different between aggressive and indolent lymphomas (16). The mean LSD in reactive lymph nodes
was found to be significantly higher than that in NHL (16). The correlation between VEGF-C and
LVD (LSD) was demonstrated in both studies. In the two studies,
lymphatic vessels with lumen structure were identified as lymphatic
vessels. However, when LVD and microvessel density (MVD) were
evaluated in solid tumors (13,14,17,18)
and MVD assessed in lymphomas (19,20),
lymphatic vessels were usually quantitated by counting endothelial
cells or cell clusters clearly separated from the adjacent cells,
tissue elements and microvessels regardless of whether a lumen
structure was observed. In adults, new lymphatic vessels form
primarily by sprouting from pre-existing vessels (21). Detry et al (22) disclosed the process of
lymphangiogenesis in adults using in vivo (lymphangiogenic
corneal assay and lymphangioma) and in vitro (lymphatic ring
assay) models. The authors showed that the lymphatic endothelial
cells migrate and organize into a cord-like structure.
Subsequently, the matrix degrades to generate space and a lumen
forms in the intercellular space (22). This suggests that a lumen structure
may not form in the initial stage of adult lymphangiogenesis. In
addition, it is possible that only lymphatic endothelial cells
could be observed even when a lumen structure existed, since only a
single slide, not a series of slides, was used to investigate LVD.
Therefore, we calculated LVD by counting LYVE-1 brown-stained
endothelial cells or cell clusters regardless of whether a lumen
structure was observed. We showed that the LVD positive rate in
aggressive lymphoma was higher than that in indolent lymphoma.
However, no difference in LSD was identified between these two
histological subtypes in the study by Wróel et al (16). The difference in definition of
lymphatic vessels between the current study and that by Wróel et
al may be the reason for the discrepant results obtained by the
two studies. This contradiction suggests that there are more
immature lymphatic vessels in aggressive than indolent lymphomas.
Our results also indicate that lymphangiogenesis plays a role in
the progression of NHL.
The correlation between COX-2 and lymphangiogenesis
has been demonstrated in a variety of types of cancer (10–13).
However, other studies failed to demonstrate this correlation
(23,24). Lymphangiogenesis is a complicated
multi-step process regulated by a group of growth factors,
cytokines and chemokines (1). In
addition to VEGF-C, other factors, including VEGF-A,
angioprotein-1, hepatocyte growth factor (HGF), insulin-like growth
factor 1 and 2 (IGF-1 and -2) and platelet-derived growth factors
(PDGFs), may also promote lymphangiogenesis (25). Although the correlation between
COX-2 and VEGF-C has been studied in diffuse large B-cell lymphoma
(DLBCL) (26), the correlation
between COX-2 and lymphangiogenesis in lymphoma is yet to be
elucidated. To the best of our knowledge, this is the first study
to demonstrate that the expression of COX-2 is significantly
correlated with LVD in NHL. This suggests that COX-2 is an inducer
of lymphangiogenesis and implies that lymphoma cells induce local
lymphangiogenesis. In this study, the expression of VEGF-C was also
associated with LVD. This is in agreement with the results of
previous studies (15,16) which estimated LVD by counting
lymphatic vessels with lumen structure. In this study, we counted
lymphatic vessels regardless of whether a lumen structure was
observed. Therefore, our results demonstrate that VEGF-C induces
lymphangiogenesis in lymphoma from a different angle from the
previous studies.
In the current study, VEGF-C expression showed a
trend of association with aggressive histology but was not
correlated with any of the clinical features investigated. VEGF-C
has been shown to be correlated with prognosis but not with
histology or any clinical features in NHL (27) and DLBCL (28). However, Ganjoo et al revealed
that VEGF-C is correlated with LDH and IPI score, but not with
progression-free or overall survival in DLBCL (29). The correlation between COX-2
expression and clinical features is also inconsistent in NHL. COX-2
expression was shown to be correlated with aggressive histology by
Paydas et al (30) whereas
the study by Hazar et al revealed that COX-2 was correlated
with disease stage (31). In the
present study, COX-2 expression was not found to be correlated with
any of the clinical features investigated. Variations in patients’
characteristics, immunostaining methods or biological heterogeneity
among individuals from different countries may be responsible for
the discrepancies. More studies are needed to decide the true roles
of VEGF-C and COX-2 in lymphomas.
In the present study, the expression levels of COX-2
and VEGF-C were correlated in NHL. However, no correlation between
COX-2 and VEGF-C was identified in DLBCL in the study by Paydas
et al (26). Staining for
VEGF-C was positive in 96% of the samples investigated in the
current study. This is in agreement with the positive rates in the
studies by Kadowaki et al, Pazgal et al and Ganjoo
et al, which were 92.3, 100 and 98%, respectively (15,28,29).
However, the VEGF-C positive rate was 36.4% in the study by Paydas
et al (26). The apparent
discrepant positive rates may be the reason for the contradicting
results of the correlation between COX-2 and VEGF-C obtained by the
two studies. The results of the current study are in agreement with
those of studies on esophageal (32,33),
head and neck (34), gastric
(11), prostate (12) and lung carcinoma (13). The correlation between COX-2 and
VEGF-C may be due to the expression of the two genes being
co-regulated or the expression of one gene being regulated by the
other. Using a human lung adenocarcinoma cell line (CL1.0)
transfected with a COX-2 expression system, Su et al
demonstrated that COX-2 regulated the expression of VEGF-C in lung
adeno-carcinoma (35). A similar
regulatory function of COX-2 has also been observed in breast
cancer cells (10,36). Therefore, the results in this study
suggest that a lymphangiogenic pathway, i.e. COX-2 upregulating
VEGF-C expression, may exist in NHL.
In conclusion, lymphangiogenesis is correlated with
aggressive histology in NHL. COX-2 and VEGF-C are inducers of
lymphangiogenesis and their expression levels are correlated in
NHL.
Acknowledgements
We are grateful for Dan Xie and Ping
Ji for their assistance in preparing slides.
References
|
1.
|
RC JiLymphatic endothelial cells, tumor
lymphangiogenesis and metastasis: New insight into intratumoral and
peritumoral lymphaticsCancer Metastasis Rev25677694200617160713
|
|
2.
|
Y CaoW ZhongTumor-derived lymphangiogenic
factors and lymphatic metastasisBiomed
Pharmacother61534539200710.1016/j.biopha.2007.08.00917904785
|
|
3.
|
M RaicaD RibattiTargeting tumor
lymphangiogenesis: an updateCurr Med
Chem17698708201010.2174/09298671079051447120088760
|
|
4.
|
T TammelaK AlitaloLymphangiogenesis:
Molecular mechanisms and future
promiseCell140460476201020178740
|
|
5.
|
MJ KarkkainenP HaikoK SainioJ PartanenJ
TaipaleTV PetrovaM JeltschDG JacksonM TalikkaH RauvalaVascular
endothelial growth factor C is required for sprouting of the first
lymphatic vessels from embryonic veinsNat
Immunol57480200410.1038/ni101314634646
|
|
6.
|
H RoyS BhardwajS Ylä-HerttualaBiology of
vascular endothelial growth factorsFEBS
Lett58028792887200616631753
|
|
7.
|
T HlaD Bishop-BaileyCH LiuHJ SchaefersOC
TrifanCyclooxygenase-1 and cyclooxygenase-2 isoenzymesInt J Biochem
Cell Biol31551557199910.1016/S1357-2725(98)00152-6
|
|
8.
|
WL SmithRM GaravitoDL DeWittProstaglandin
endoperoxide H synthases (cyclooxygenases)-1 and -2J Biol
Chem2713315733160199610.1074/jbc.271.52.331578969167
|
|
9.
|
N GhoshR ChakiV MandalS MandalCox-2 as a
target for cancer chemotherapyPharmacol
Rep62233244201010.1016/S1734-1140(10)70262-020508278
|
|
10.
|
RN BhattacharjeeAV TimoshenkoJ CaiPK
LalaRelationship between cyclooxygenase-2 and human epidermal
growth factor receptor 2 in vascular endothelial growth factor C
up-regulation and lymphangiogenesis in human breast cancerCancer
Sci10120262032201010.1111/j.1349-7006.2010.01647.x
|
|
11.
|
J ZhangJ JiF YuanL ZhuC YanYY YuBY LiuZG
ZhuYZ LinCyclooxygenase-2 expression is associated with VEGF-C and
lymph node metastases in gastric cancer patientsBiomed
Pharmacother59Suppl
2S285S288200510.1016/S0753-3322(05)80047-216507394
|
|
12.
|
JM DiJ ZhouXL ZhouX GaoCQ ShaoJ PangQP
SunY ZhangXX RuanCyclooxygenase-2 expression is associated with
vascular endothelial growth factor-C and lymph node metastasis in
human prostate cancerArch Med
Res40268275200910.1016/j.arcmed.2009.03.00219608016
|
|
13.
|
X GuoY ChenZ XuZ XuY QianX YuPrognostic
significance of VEGF-C expression in correlation with COX-2,
lymphatic microvessel density, and clinicopathologic
characteristics in human non-small cell lung cancerActa Biochim
Biophys Sin (Shanghai)41217222200910.1093/abbs/gmp00419280060
|
|
14.
|
N WeidnerJP SempleWR WelchJ FolkmanTumor
angiogenesis and metastasis - correlation in invasive breast
carcinomaN Engl J
Med32418199110.1056/NEJM1991010332401011701519
|
|
15.
|
I KadowakiR IchinohasamaH HarigaeK
IshizawaY OkitsuJ KameokaT SasakiAccelerated lymphangiogenesis in
malignant lymphoma: possible role of VEGF-A and VEGF-CBr J
Haematol130869877200510.1111/j.1365-2141.2005.05695.x16156857
|
|
16.
|
T WróelG MazurP DziegielM JeleńA SzubaK
KuliczkowskiM ZabelDensity of intranodal lymphatics and VEGF-C
expression in B-cell lymphoma and reactive lymph nodesFolia
Histochem Cytobiol444347200616584091
|
|
17.
|
TC MineoV AmbrogiA BaldiC RabittiP
BolleroB VincenziG ToniniPrognostic impact of VEGF, CD31, CD34, and
CD105 expression and tumor vessel invasion after radical surgery
for IB-IIA non-small cell lung cancerJ Clin
Pathol57591597200410.1136/jcp.2003.01350815166262
|
|
18.
|
M LinSP MaHZ LinP JiD XieJX YuIntratumoral
as well as peritumoral lymphatic vessel invasion correlates with
lymph node metastasis and unfavorable outcome in colorectal
cancerClin Exp
Metastasis27123132201010.1007/s10585-010-9309-020195706
|
|
19.
|
EC CitakA OguzC KaradenizN
AkyurekImmunohistochemical expression of angiogenic cytokines in
childhood Hodgkin lymphomaPathol Res
Pract2048996200810.1016/j.prp.2007.11.00518207652
|
|
20.
|
D GratzingerS ZhaoRJ MarinelliAV KappRJ
TibshiraniAS HammerS Hamilton-DutoitY NatkunamMicrovessel density
and expression of vascular endothelial growth factor and its
receptors in diffuse large B-cell lymphoma subtypesAm J
Pathol17013621369200710.2353/ajpath.2007.06090117392174
|
|
21.
|
T HolopainenM BryK AlitaloA
SaaristoPerspective on lymphangiogenesis and angiogenesis in
cancerJ Surg Oncol103484488201110.1002/jso.2180821480240
|
|
22.
|
B DetryF BruyèreC ErpicumJ PaupertF
LamayeC MaillardB LenoirJ FoidartM ThiryA NoëlDigging deeper into
lymphatic vessel formation in vitro and in vivoBMC Cell
Biol122939201110.1186/1471-2121-12-2921702933
|
|
23.
|
A Longatto-FilhoC PinheiroSM PereiraD
EtlingerMA MoreiraLF JubéGS QueirozF BaltazarFC SchmittLymphatic
vessel density and epithelial D2-40 immunoreactivity in
pre-invasive and invasive lesions of the uterine cervixGynecol
Oncol1074551200710.1016/j.ygyno.2007.05.02917604828
|
|
24.
|
HF GouXC ChenJ ZhuM JiangY YangD CaoM
HouExpression of COX-2 and VFGF-C in gastric cancer: correlations
with lymphangiogenesis and prognostic implicationsJ Exp Clin Cancer
Res301421201110.1186/1756-9966-30-1421272377
|
|
25.
|
V MumprechtM DetmarLymphangiogenesis and
cancer metastasisJ Cell Mol
Med1314051416200910.1111/j.1582-4934.2009.00834.x19583813
|
|
26.
|
S PaydasM ErginG SeydaogluS ErdoganS
YavuzPrognostic significance of angiogenic/lymphangiogenic,
anti-apoptotic, inflammatory and viral factors in 88 cases with
diffuse large B cell lymphoma and review of the literatureLeuk
Res3316271635200910.1016/j.leukres.2009.02.015
|
|
27.
|
S PaydasG SeydaogluM ErginS ErdoganS
YavuzThe prognostic significance of VEGF-C and VEGF-A in
non-Hodgkin lymphomasLeuk
Lymphoma50366373200910.1080/1042819080270666519347725
|
|
28.
|
I PazgalO BoycovO ShpilbergE OkonO
BaireyExpression of VEGF-C, VEGF-D and their receptor VEGFR-3 in
diffuse large B-cell lymphomasLeuk
Lymphoma4822132220200710.1080/1042819070163282217926187
|
|
29.
|
KN GanjooAM MooreA OraziJA SenCS JohnsonCS
AnThe importance of angiogenesis markers in the outcome of patients
with diffuse large B cell lymphoma: a retrospective study of 97
patientsJ Cancer Res Clin
Oncol134381387200810.1007/s00432-007-0294-x17694324
|
|
30.
|
S PaydasM ErginS ErdoganG
SeydaogluCyclooxygenase-2 expression in non-Hodgkin’s lymphomasLeuk
Lymphoma483893952007
|
|
31.
|
B HazarM ErginE SeyrekS ErdoğanI TuncerS
HakverdiCyclooxygenase-2 (Cox-2) expression in lymphomasLeuk
Lymphoma4513951399200410.1080/1042819031000165403215359639
|
|
32.
|
BHA Von RahdenHJ SteinF PuhringerI KochR
LangerG PiontekJR SiewertH HoflerM SarbiaCoexpression of
cyclooxygenases (COX-1, COX-2) and vascular endothelial growth
factors (VEGF-A, VEGF-C) in esophageal adenocarcinomaCancer
Res6550385044200515958546
|
|
33.
|
JS ByeonHY JungYJ LeeD LeeGH LeeSJ MyungSK
YangWS HongJH KimYI MinJS KimClinicopathological significance of
vascular endothelial growth factor-C and cyclooxygenase-2 in
esophageal squamous cell carcinomaJ Gastroenterol
Hepatol19648654200410.1111/j.1440-1746.2004.03348.x15151619
|
|
34.
|
PA KyzasD StefanouNJ AgnantisCOX-2
expression correlates with VEGF-C and lymph node metastases in
patients with head and neck squamous cell carcinomaMod
Pathol18153160200510.1038/modpathol.380024415272284
|
|
35.
|
JL SuJY ShihML YenYM JengCC ChangCY
HsiehLH WeiPC YangML KuoCyclooxygenase-2 induces EP1- and
HER-2/Neu-dependent vascular endothelial growth factor-C
up-regulation: a novel mechanism of lymphangiogenesis in lung
adenocarcinomaCancer
Res64554564200410.1158/0008-5472.CAN-03-130114744769
|
|
36.
|
AV TimoshenkoC ChakrabortyGF WagnerPK
LalaCOX-2-mediated stimulation of the lymphangiogenic factor VEGF-C
in human breast cancerBr J
Cancer9411541163200610.1038/sj.bjc.660306716570043
|