Introduction
Pneumonectomy is a standard surgical approach for
central lung cancer patients. Extensive pulmonary resection offers
curative treatment in a large population of patients and has been
widely accepted. Postoperative adjuvant chemotherapy in non-small
cell lung cancer (NSCLC) patients has been reported to be an
efficient therapy, resulting in significant improvement in overall
survival (OS) (1–4). Previous studies have focused on
postoperative adjuvant chemotherapy, including mixed exploratory
thoracotomy, wedge resections, lobectomy and pneumonectomy with or
without extended resection of the chest wall (1–4).
However, no study focusing solely on pneumonectomy has been
published. Moreover, in one study, not all patients were treated
with third generation chemotherapy agents such as taxol,
vinorelbine and gemcitabine. As no studies on the effect of
adjuvant third generation chemotherapy agents for NSCLC after only
pneumonectomy have been performed, the role of post-pneumonectomy
adjuvant chemotherapy is unclear and more data are required.
Long-term respiratory complications have been
considered to be the most severe events after pneumonectomy, since
‘one-lung’ patients are at a high risk of respiratory failure.
Chemotherapy is an additional risk factor for respiratory
complications (5,6). Therefore, the administration of
adjuvant chemotherpy after pneumonectomy for NSCLC is
controversial.
In the present study, we investigated the effect of
adjuvant chemotherapy on NSCLC after pneumonectomy and identified a
population of patients who benefited from adjuvant chemotherapy
with TP/NP/GP. Our data may aid the identification of patients who
are likely to benefit from post-pneumonectomy adjuvant chemotherapy
in NSCLC. This is the first intensive observation of the effect of
adjuvant chemotherapy (third generation) combined with
pneumonectomy.
Patients and methods
Patients
A retrospective chart review analysis was performed
on NSCLC patients who underwent pneumonectomy. A total of 261 NSCLC
patients were treated with pneumonectomy at the Tianjin Cancer
Hospital of Tianjin Medical University (between January 2000 and
January 2007). A total of 6 patients (2.3%) who underwent
pneumonectomy succumbed within 30 days of surgery and 3 patients
(1.1%) underwent incomplete resection. Patients who had received
radiation therapy, biotherapy or induction therapy (stage pN2), who
were lost to follow-up or succumbed to postoperative complications
and patients with an ECOG performance status of 2–3 who did not
recover within 6 weeks of surgery were excluded from the study. The
remaining 217 patients who underwent pneumonectomy and had an ECOG
performance status of 0–1 6 weeks after surgery were identified for
this study. Among these patients, 130 underwent pneumonectomy as
the only therapy in the initial treatment of their disease; 79
patients underwent pneumonectomy and 3 or 4 cycles of adjuvant
chemotherapy of TP/NP/GP regimen [TP: taxol, 135–175
mg/m2, day 1 and carboplatin, area under the ROC curve
(AUC)=5, day 1; NP: Navelbine, 25 mg/m2, days 1 and 8
and carboplatin, AUC=5, day 1; GP: gemcitabine, 1250
mg/m2, days 1 and 8 and carboplatin, AUC=5, day 1]. A
total of 8 patients who were treated with only 1 or 2 cycles of
chemotherapy due to toxicity were also included into this study.
These two groups of patients had similar clinical stages of disease
and preoperative respiratory function. Blood count (WBC
>3.0×109 l−1; absolute neutrophil count
>1500×109 l−1; platelets >100×109
l−1), liver function (aspartate aminotransferase/alanine
aminotransferase and alkaline phosphatase ≤2 times the upper limit
of normal was accepted) and renal function (serum creatinine ≤2
mg/dl via biochemistry tests) were monitored in all patients prior
to adjuvant chemotherapy.
Informed consent was obtained either from the
patient or the patient’s family. The study was approved by the
ethics committee of Tianjin Medical University, Tianjin, China.
Diagnosis
All patients underwent preoperative computed
tomography (CT) scans of the thorax and upper abdomen or ultrasound
of the upper abdomen, fiber-optic bronchoscopy with cytological
specimens, bone scintigraphy and brain CT. Preoperative respiratory
function was assessed routinely by blood gas analysis, spirometry
and lung perfusion scan.
Standard pneumonectomy was defined as the
intrapericardial or extrapericardial removal of the entire lung,
associated with radical mediastinal lymph node dissection without
any resection of mediastinal, chest wall or diaphragmatic
structure.
If there were any signs of metastasis to the
mediastinum (lymph nodes >1.5 cm), mediastinoscopy was performed
as routine. If the procedure yielded negative results, the patients
underwent thoracotomy. If the procedure had positive results, the
patients underwent induction therapy (excluded from the study).
However, certain patients were diagnosed as having pathological N2
disease following surgery. No patients had a positron emission
tomography scan due to the unavailability of this equipment in our
city prior to 2007. Pathological and clinical TNM staging was
determined according to the guidelines of the American Joint
Committee on Cancer (7,8). Histological subtypes included squamous
cell, adenocarcinoma and other types, such as bronchoalveolar
carcinoma, large cell carcinoma and adenosquamous.
Evaluation
Preoperative patient variables were collected in the
surgical database. Survival time was calculated from the date of
pathological diagnosis of lung cancer. OS was used as the primary
endpoint of the study. OS was compared between the adjuvant
chemotherapy and pneumonectomy only groups, taking into account
age, preoperative respiratory function and site of surgery.
Follow-up
Follow-up data were collected directly from our
outpatient clinic records. All patients followed a standardized
program of clinical and instrumental examinations. The median
follow-up time was 35 months (range, 3–125).
Statistical analysis
Actuarial survival analysis was calculated using the
Kaplan-Meier method. The log-rank test was used to compare the OS
between the groups. P<0.05 was considered to indicate a
statistically significant result All statistical analyses were
performed using SPSS software (version 13.0 for Windows).
Results
Patient population
Demographic data of the adjuvant chemotherapy and
pneumonectomy only groups are shown in Table I. The mean age of patients involved
in this study was 56 years (range, 32–75). The number of patients
treated with left pneumonectomy was 173. The number of patients
with preoperative forced expiratory volume in 1 sec (FEV1) ≥21 was
86. The tumor pathology stages included stage IB (13.8%), stage II
(34.5%) and stage IIIA (51.7%) in the adjuvant chemotherapy group
and stage IB (22.3%), stage II (40%) and stage IIIA (37.7%) in the
pneumonectomy only group. The histological type of the tumors was
squamous cell (77%), adenocarcinoma (17%) and other (6%) in the
adjuvant chemotherapy group and squamous cell (72%), adenocarcinoma
(23%) and other (5%) in the pneumonectomy only group. In summary,
the demographic data were similar in the two groups with regard to
age, gender, histological type of tumors, tumor P-stage, ECOG
performance status and preoperative respiratory function.
 | Table I.Demographics. |
Table I.
Demographics.
| Variable | Adjuvant
chemotherapy n=87 | Pneumonectomy only
n=130 | P-value |
|---|
| Male | 68 | 98 | 0.64 |
| Age ≥65 years | 34 | 35 | 0.06 |
| P-stage | | | 0.09 |
| IB | 12 | 29 | |
| II | 30 | 52 | |
| IIIA | 45 | 49 | |
| FEV1 (l), mean ±
SD | 1.95±0.43 | 1.88±0.38 | 0.21 |
Mortality and complications
During the follow-up period, 217 cases were analyzed
and 173 patients succumbed. Of the 173 patients, 89% succumbed to
cancer and 11% succumbed to other causes. Of the 6 patients in the
surgery group who succumbed to other causes, 4 succumbed to
respiratory failure, 1 to myocardial infarction and 1 to unknown
causes. Of the 13 patients in the chemotherapy group who succumbed
to other causes, 1 succumbed to myocardial infarction and 12 to
respiratory failure (6 from the right pneumonectomy group, 6 from
the left pneumonectomy group). Complications of post-pneumonectomy
adjuvant chemotherapy included bronchopleural fistula (2 cases),
pneumonia (11 cases) and interstitial lung disease (4 cases). No
unusual associated toxicity was recorded during the chemotherapy.
No patients succumbed to treatment-related toxicity during
chemotherapy.
Survival analysis
The 5-year actuarial OS rate of the patients was
32.1% in the present study. The 5-year actuarial OS rates of the
left and right pneumonectomy groups were 34.3 and 26.2%,
respectively (P=0.35). The 5-year actuarial OS rates of the
adjuvant chemotherapy and pneumonectomy only groups were 36.2 and
30.1%, respectively (P=0.067) .
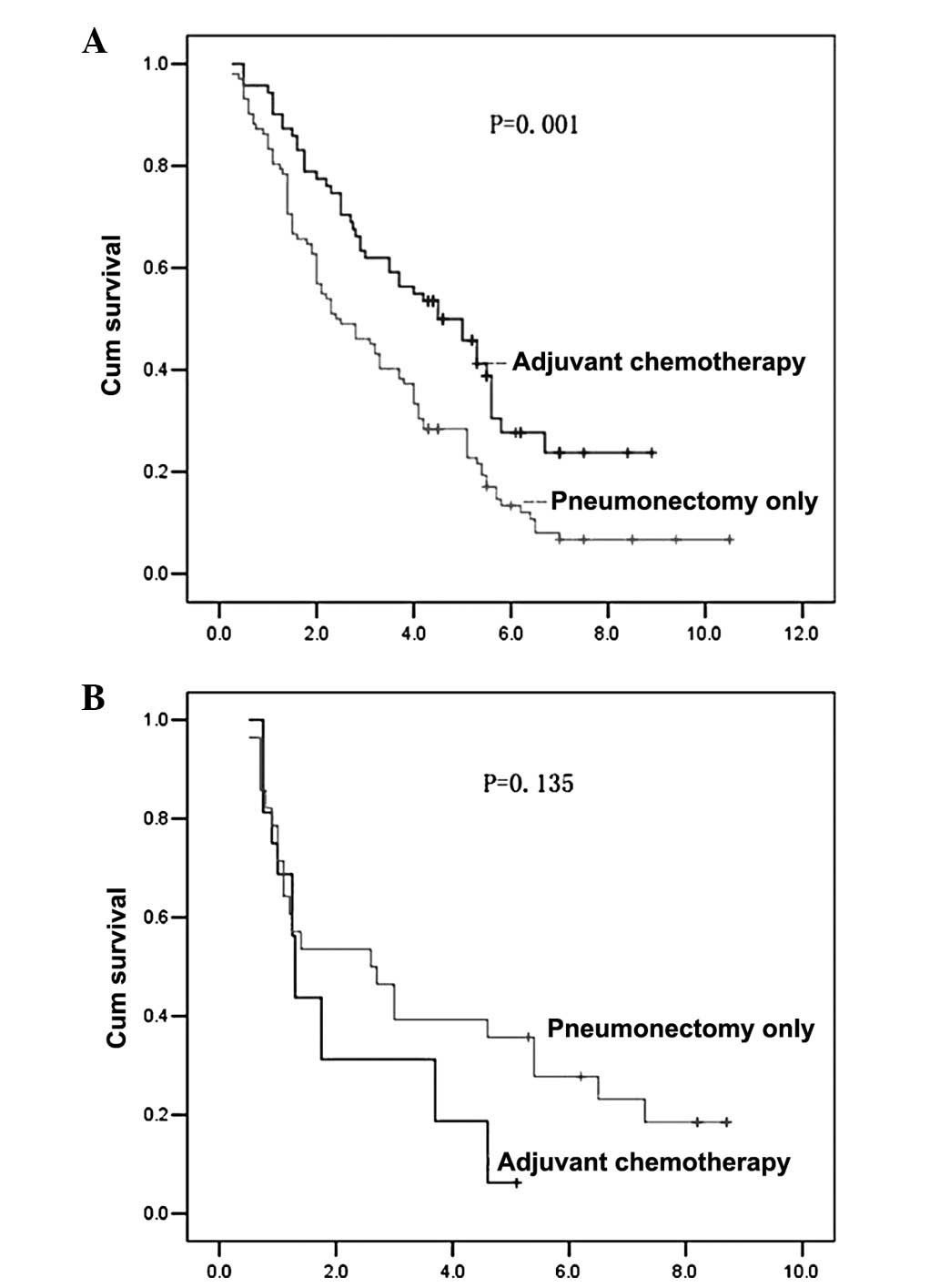
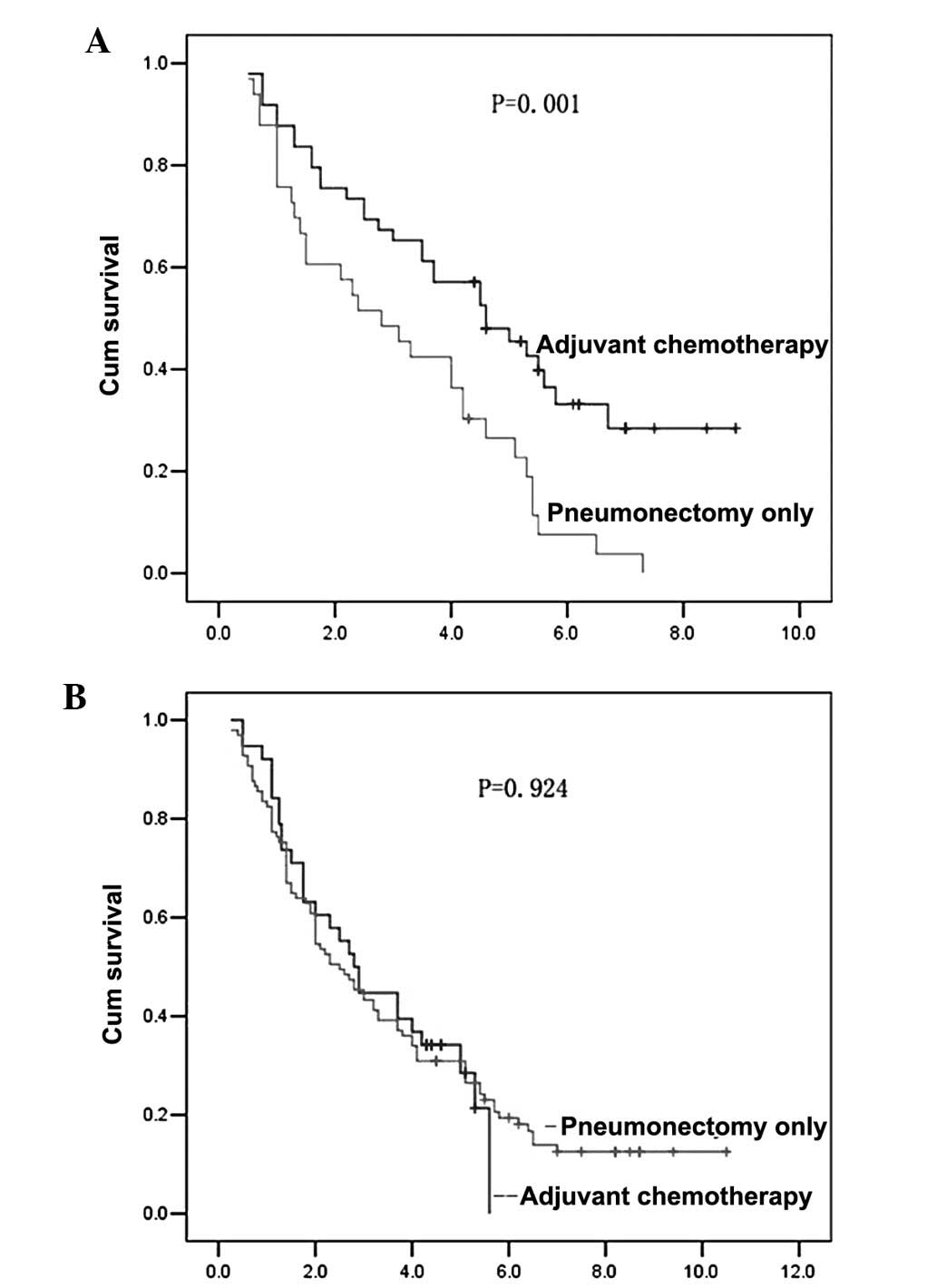
The univariate analysis of OS demonstrated that
postoperative adjuvant chemotherapy significantly increased the
survival rate in patients who underwent left pneumonectomy
(P=0.001; Fig. 1A) and in patients
with preoperative FEV1 ≥21 (P=0.001; Fig. 2A).
The univariate analysis of OS demonstrated that
postoperative adjuvant chemotherapy did not significantly increase
the survival rate in patients with right pneumonectomy (Fig. 1B), preoperative FEV1 <21
(Fig. 2B), age ≥65 years (P=0.105)
and age <65 years (P=0.091; data not shown).
To clarify our analysis, multivariate analysis was
performed. The Cox proportional hazards ratio model revealed that
adjuvant chemotherapy was an independent prognostic factor for
better survival in patients with preoperative FEV1 ≥21 and patients
who underwent left pneumonectomy (Tables II and III).
| Table II.Cox proportional hazard ratio model
showed that adjuvant chemotherapy was an independent prognostic
factor in patients with preoperative FEV1 ≥21. |
Table II.
Cox proportional hazard ratio model
showed that adjuvant chemotherapy was an independent prognostic
factor in patients with preoperative FEV1 ≥21.
| Variable | Hazard ratio | 95% confidence
interval | P-value |
|---|
| Adjuvant
chemotherapy (yes/no) | 0.49 | 0.28–0.86 | 0.012 |
| P-stage (IB/II,
IIIA) | 0.33 | 0.15–0.70 | 0.004 |
| Age, years
(<65/≥65) | | | 0.265 |
| Gender
(male/female) | | | 0.776 |
| Pneumonectomy
(left/right) | | | 0.209 |
| Table III.Cox proportional hazard ratio model
showed that adjuvant chemotherapy was an independent prognostic
factor in patients who underwent left pneumonectomy. |
Table III.
Cox proportional hazard ratio model
showed that adjuvant chemotherapy was an independent prognostic
factor in patients who underwent left pneumonectomy.
| Variable | Hazard ratio | 95% confidence
interval | P-value |
|---|
| Adjuvant
chemotherapy (yes/no) | 0.61 | 0.42–0.88 | 0.009 |
| P-stage (IB/II,
IIIA) | 0.34 | 0.21–0.57 | 0.000 |
| Age, years
(<65/≥65) | | | 0.599 |
| Gender
(male/female) | | | 0.999 |
| FEV1, l
(<2/≥2) | | | 0.236 |
Discussion
The present study is the first to evaluate the
effect of adjuvant third generation chemotherapy agents on NSCLC
after only pneumonectomy and analyze the population of patients who
are likely to benefit from adjuvant chemotherapy. We have
demonstrated that a low respiratory capacity, assessed as FEV1,
appears to be the most important predictor of a high risk of
complications following lung resection (9). The British Thoracic Society (BTS)
guidelines state that no further respiratory function tests are
required for a pneumonectomy if the post-bronchodilator FEV1 is
above 2.0 1, provided that there is no evidence of interstitial
lung disease or unexpected disability due to shortness of breath
(10). The preoperative FEV1 is
likely to be the most important marker of respiratory
functions.
Postoperative cardiopulmonary function and exercise
capacity have been examined following pulmonary resection and
demonstrated to be persistently decreased only after pneumonectomy
(11,12). The impairment of respiratory
function after a pneumonectomy may be explained by overdistention
and emphysematous changes of the contralateral lung (which may show
evidence of histological hyperplasia and loss of elasticity), an
increase in the airway resistance resulting in alveolar gas mixing,
arterial desaturation or late pulmonary failure. Consistent with
this point, it has been reported that the impairment of the
alveolocapillary membrane is more likely to occur after
chemotherapy (13) which may be
synergic with other risk factors, including age or fluid overload
causing lung damage (14).
Therefore, chemotherapy after pneumonectomy may aggravate lung
damage. Our data show that postoperative adjuvant chemotherapy
significantly improves the survival rate of patients with
preoperative FEV1 greater than or equal to 21, but has no effect on
patients with preoperative FEV1 of less than 21. Preoperative
respiratory functions affect the results of chemotherapy following
pneumonectomy. The better respiratory function of the NSCLC
patients before pneumonectomy, the better the effect of
postoperative adjuvant chemotherapy. This is most likely due to
patients with good respiratory functions rarely succumbing to
respiratory failure caused by postoperative adjuvant chemotherapy.
Winton et al (15) reported
that adjuvant treatment with third generation chemotherapy agents
may be safely administered in the outpatient setting with limited
toxicity and is beneficial for NSCLC patients; 25% of the patients
accepted pneumonectomy. This report is in line with our results. In
summary, chemotherapy in NSCLC patients with good performance
status after complete resection is beneficial.
It is well known that the impairment of respiratory
function after right pneumonectomy is more serious than that
following left pneumonectomy. Martin et al reported that
pneumonectomy on the right side is associated with a mortality rate
of 24% at 3 months, whereas there was no mortality following left
pneumonectomy (16). The safety of
pneumonectomy, especially right pneumonectomy after induction
therapy, has been questioned in several studies (16,17).
In the present study, 37% (6/16) of the patients with right
pneumonectomy succumbed to respiratory failure in the adjuvant
chemotherapy group, whereas only 8% (6/71) of patients with left
pneumonectomy succumbed to respiratory failure in the adjuvant
chemotherapy group. Respiratory failure was one of the main causes
of mortality in patients who underwent right pneumonectomy
following adjuvant chemotherapy in the present study. Our data show
that postoperative adjuvant chemotherapy significantly improved the
survival rate of patients who underwent left, but not right,
pneumonectomy.
Since the impairment of respiratory function after
right pneumonectomy is more serious than that following left
pneumonectomy and the mortality rate of right pneumonectomy is
high, between January 2000 and January 2007, a total of 44 NSCLC
patients treated with right pneumonectomy were identified in our
hospital. As the number is low, it is possible to generate
statistical errors. This is a preliminary study, further study will
continue in the future with an increasing number of patients who
underwent right pneumonectomy.
In the present study, we investigated the
correlation between age and the effect of chemotherapy following
pneumonectomy. We found that there was no significant difference
between the survival rate in patients with or without postoperative
adjuvant chemotherapy (P>0.05) in patients aged 65 years or over
or those younger than 65. In conclusion, the age of the patients
does not affect the result of chemotherapy following
pneumonectomy.
This is a retrospective study, which allows the
analysis of the outcomes of a large number of patients treated in a
relatively uniform manner. The results of our study suggest that
adjuvant chemotherapy following pneumonectomy benefits patients
with preoperative FEV1 of 21 or above or patients who undergo left
pneumonectomy. The age of patients is not a significant factor.
Acknowledgements
We would like to thank Dr Hong Yang
for assistance in editing this manuscript. We also thank the
Division of Medical Records, Cancer Hospital of Tianjin Medical
University for technical assistance with the project.
References
|
1.
|
A NiiranenS Niitamo-KorhonenM KouriA
AssendelftK MattsonS PyrhönenAdjuvant chemotherapy after radical
surgery for non-small-cell lung cancer: a randomized studyJ Clin
Oncol101927193219921333518
|
|
2.
|
H WadaS HitomiT TeramatsuAdjuvant
chemotherapy after complete resection in non-small-cell lung
cancer. West Japan Study Group for Lung Cancer SurgeryJ Clin
Oncol14104810541996
|
|
3.
|
H KatoM TsuboiM OhtaE HataN TsubotaN
HamajimaA randomized phase III trial of adjuvant chemotherapy with
UFT for completely resected pathological stage I (T1N0M0, T2N0M0)
adenocarcinoma of the lungProc Am Soc Clin Oncol22abstract
2498200315598942
|
|
4.
|
R ArriagadaB BergmanA DunantT Le
ChevalierJP PignonJ VansteenkisteInternational Adjuvant Lung Cancer
Trial Collaborative GroupCisplatin-based adjuvant chemotherapy in
patients with completely resected non-small-cell lung cancerN Engl
J Med350351360200410.1056/NEJMoa03164414736927
|
|
5.
|
JR RobertsC EustisR DevoreD CarboneH ChoyD
JohnsonInduction chemotherapy increases perioperative complications
in patients undergoing resection for non-small cell lung cancerAnn
Thorac Surg72885888200110.1016/S0003-4975(01)02836-3
|
|
6.
|
N NovoaG VarelaMF JimenezMorbidity after
surgery for non-small cell lung carcinoma is not related to
neoadjuvant chemotherapyEur J Cardiothorac
Surg20700704200110.1016/S1010-7940(01)00876-4
|
|
7.
|
CF MountainValue of the new TNM staging
system for lung cancerChest961
Suppl47S49S198910.1378/chest.96.1_Supplement.47S2544360
|
|
8.
|
CF MountainRevisions in the International
System for Staging Lung
CancerChest11117101717199710.1378/chest.111.6.17109187198
|
|
9.
|
J WangJ OlakRE UltmannMK
FergusonAssessment of pulmonary complications after lung
resectionAnn Thorac
Surg6714441447199910.1016/S0003-4975(99)00255-610355428
|
|
10.
|
British Thoracic SocietySociety of
Cardiothoracic Surgeons of Great Britain and Ireland Working
PartyBTS guidelines: guidelines on the selection of patients with
lung cancer for
surgeryThorax5689108200110.1136/thorax.56.2.8911209097
|
|
11.
|
AM NugentIC SteeleAM CarragherK McManusJA
McGuiganJR GibbonsEffect of thoracotomy and lung resection on
exercise capacity in patients with lung
cancerThorax54334338199910.1136/thx.54.4.33410092695
|
|
12.
|
KR LarsenUG SvendsenN MilmanJ BrenøeB
PetersenCardiopulmonary function at rest and during exercise after
resection for bronchial carcinomaAnn Thorac
Surg64960964199710.1016/S0003-4975(97)00635-89354509
|
|
13.
|
DE StoverRJ KanerAdverse effects of
treatment: pulmonary toxicityCancer Principles & Practice of
OncologyVT De VitaS HellmanAA Rosenberg7th editionLippincott
Williams & WillkinsPhiladelphia253925452004
|
|
14.
|
L ChapR ShpinerM LevineL NortonM LillJ
GlaspyPulmonary toxicity of high-dose chemotherapy for breast
cancer: a non-invasive approach to diagnosis and treatmentBone
Marrow Transplant2010631067199710.1038/sj.bmt.17010289466279
|
|
15.
|
T WintonR LivingstonD JohnsonJ RigasM
JohnstonC ButtsNational Cancer Institute of Canada Clinical Trials
GroupNational Cancer Institute of the United States Intergroup
JBR.10 Trial InvestigatorsVinorelbine plus cisplatin vs.
observation in resected non-small-cell lung cancerN Engl J
Med35225892597200510.1056/NEJMoa043623
|
|
16.
|
J MartinRJ GinsbergA AbolhodaMS BainsRJ
DowneyRJ KorstMorbidity and mortality after neoadjuvant therapy for
lung cancer: the risks of right pneumonectomyAnn Thorac
Surg7211491154200110.1016/S0003-4975(01)02995-211603428
|
|
17.
|
C DoddoliF BarlesiD TrousseS RobitailS
YenaP AstoulOne hundred consecutive pneumonectomies after induction
therapy for non-small cell lung cancer: an uncertain balance
between risks and benefitsJ Thorac Cardiovasc
Surg130416425200510.1016/j.jtcvs.2004.11.022
|