Introduction
Merkel cell carcinoma (MCC) in the skin was first
described by Toker in 1972 (1). It
is an uncommon skin neoplasm of the elderly population (2). The majority of patients with MCC
present with localised disease at diagnosis and few patients have
regional lymph node (LN) involvement and distant metastases
(3). MCC was historically
considered to be an indolent skin tumour, but it has now been
demonstrated to be highly aggressive, with recurrence and
metastasis (4). Although it has
been previously reported in various anatomical sites (5), LN metastatic MCC in the absence of a
primary site is extremely rare (6)
and for this reason there is no standard approach to its
management.
Curative surgery, particularly Mohs micrographic
surgery, is commonly recommended to manage localised MCC (7,8).
Nevertheless, specific postoperative palliative treatments for MCC
have emerged, including radiotherapy (RT) or chemotherapy, due to
the high local failure rate and the aggressive nature of the
disease. Clinical investigators have performed a large number of
monotherapies or various combinations of surgery, RT and
chemotherapy, but the stage, size and location of the tumours
investigated has varied, making retrospective analysis difficult.
Therefore, conclusions with regard to these treatment regimens in
patients with MCC are controversial (9–11). It
is important to identify the contribution of the treatment
regimens.
In the present study we report the case of an Asian
patient with LN metastatic MCC in the absence of a primary site and
summarise 23 published cases of MCC with initial LN metastasis in
the absence of a primary site, in which the clinical
characteristics, natural history and pertinent therapy of this
uncommon tumour are described.
Case reports
Clinical presentation and diagnosis of
cancer
A 54-year-old male had complained of a palpable
subcutaneous mass in the right groin increasing in size for ∼4
months. Written consent for publication was obtained from the
patient. The mass was nontender, firm, painless, but not hard. The
patient had no other symptoms but had had psoriasis for 20 years.
Examination of the patient with enhanced computed tomography and
positron emission tomography-computed tomography (PET-CT)
demonstrated that the skull, chest and abdomen were normal, but
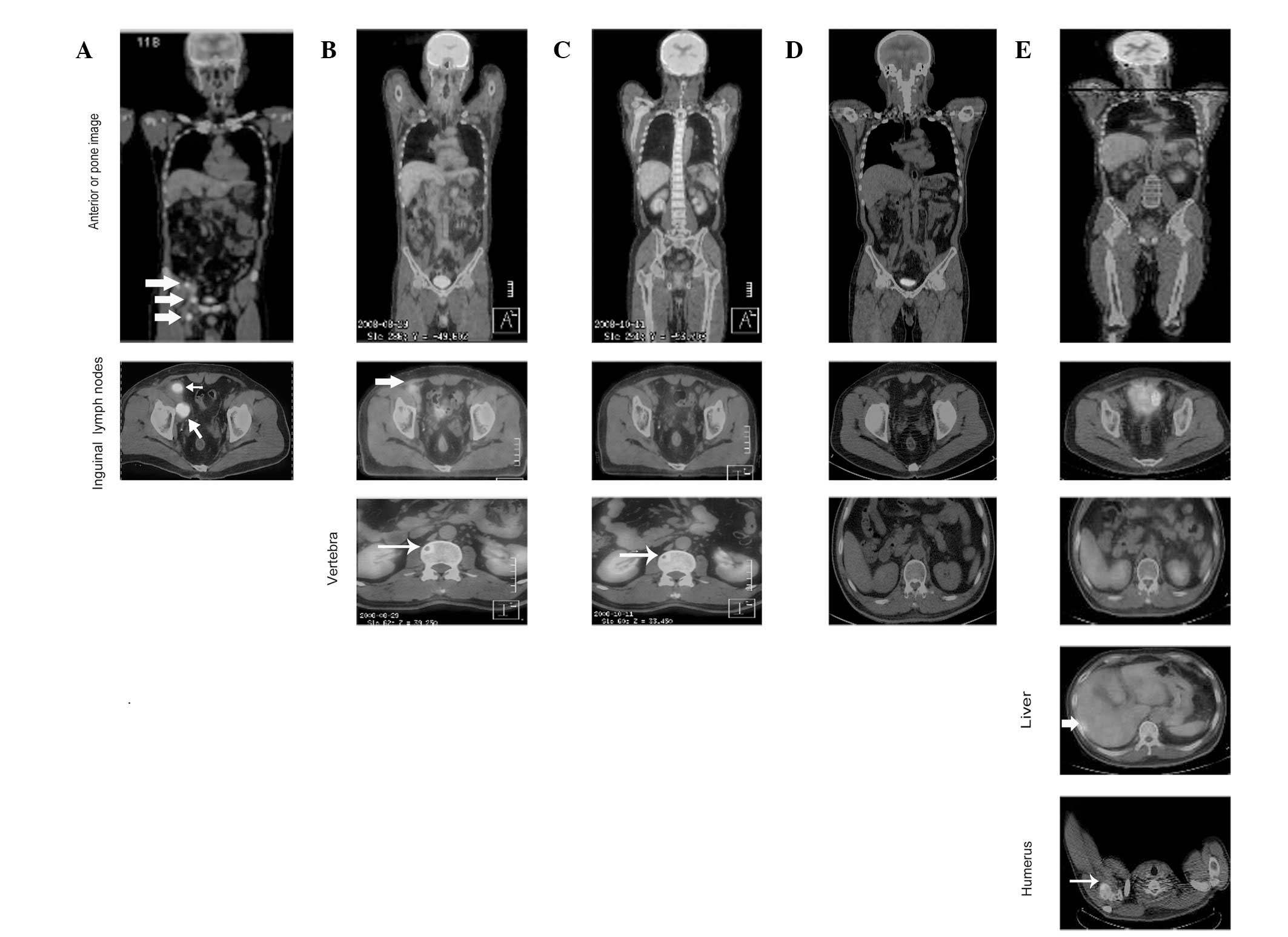
three masses were observed in the right groin (Fig. 1A). A biopsy was performed, leading
to a diagnosis of right inguinal LNs consistent with small cell
carcinoma metastasis from another organ, most probably the lung.
Serum tumour markers were negative for carcinoembryonic antigen,
α-fetoprotein, prostate-specific antigen, CA125, CA15-3 and CA19-9,
but positive for nonspecific esterase (NSE; 83.73 ng/ml; normal,
<16.30 ng/ml) and the tumour marker CYFRA (5.80 ng/ml; normal,
<3.30 ng/ml). The patient had a performance status of 0 and was
referred to our hospital.
A further histological examination of the biopsy
specimen was made, demonstrating metastatic small cell carcinoma
composed of small cells with oval to fusiform hyperchromatic nuclei
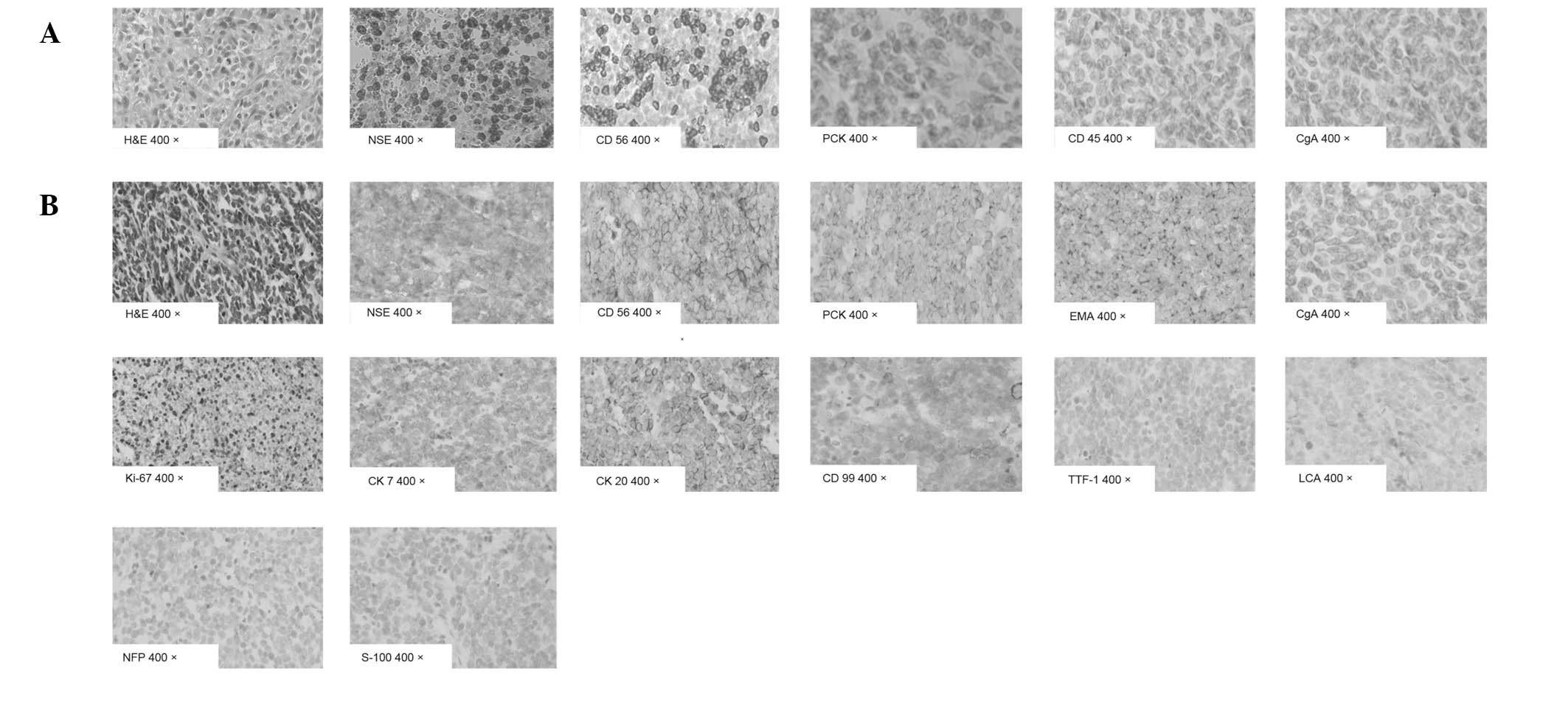
and indistinct nucleoli with frequent mitoses (Fig. 2A). Immunohistochemistry demonstrated
a marked positive reaction for NSE, CD56 and protein kinase C
(PKC), but was negative for CD45 and chromogranin A (CgA). The
Ki-67 staining index was ∼85% (Fig.
2A). The morphological and immunohistochemical features were in
keeping with metastatic small cell carcinoma. However, no primary
tumour was identified in any sites following extensive
investigations. A diagnosis of metastatic small cell carcinoma in
right inguinal LNs without a primary site was made.
The patient received therapy (as described in the
treatment and clinical course section) and a PET-CT scan was
performed at the end of therapy, which revealed a complete
response. Following 4 months with no evidence of disease, a
subcutaneous mass developed. Clinical examination disclosed a
rapidly growing, painless, firm, grey skin nodule in the right
dorsal thigh measuring 3.5x4.5x1.5 cm. PET-CT demonstrated
metastatic disease in the liver and humerus. Mohs micrographic
surgery was performed. Histological examination of a biopsy
specimen demonstrated nodules and diffuse sheets of basophilic
cells with imperceptible cytoplasm and round or oval vesicular
nuclei and dispersed chromatin with a pathognomonic watery
appearance (Fig. 2B).
Immunohistochemistry demonstrated a marked positive reaction for
NSE, CD56, PKC, epithelial membrane antigen, CK7, CK20 and CD99.
Tumour cells were negative for CgA, thyroid transcription factor-1
(TTF-1), leucocyte common antigen (LCA), neurofilament protein and
S100. The Ki-67 staining index was ∼70% (Fig. 2B). This combined evidence confirmed
a final diagnosis of MCC with multiple metasases in inguinal LNs,
bone and liver.
Treatment and clinical course
The patient was initially treated with a combination
of etoposide (100 mg/m2, days 1–5) and cisplatin (50
mg/m2, days 1–3) every 3 weeks. A partial response was
achieved in the LNs but progressive metastatic disease was present
in T6 and T12-L2 following two cycles (Fig. 1B). The patient then received
chemotherapy with irinotecan (100 mg/m2, day 1, 8, 15)
and cisplatin (40 mg/m2, days 1–3) every 3 weeks as well
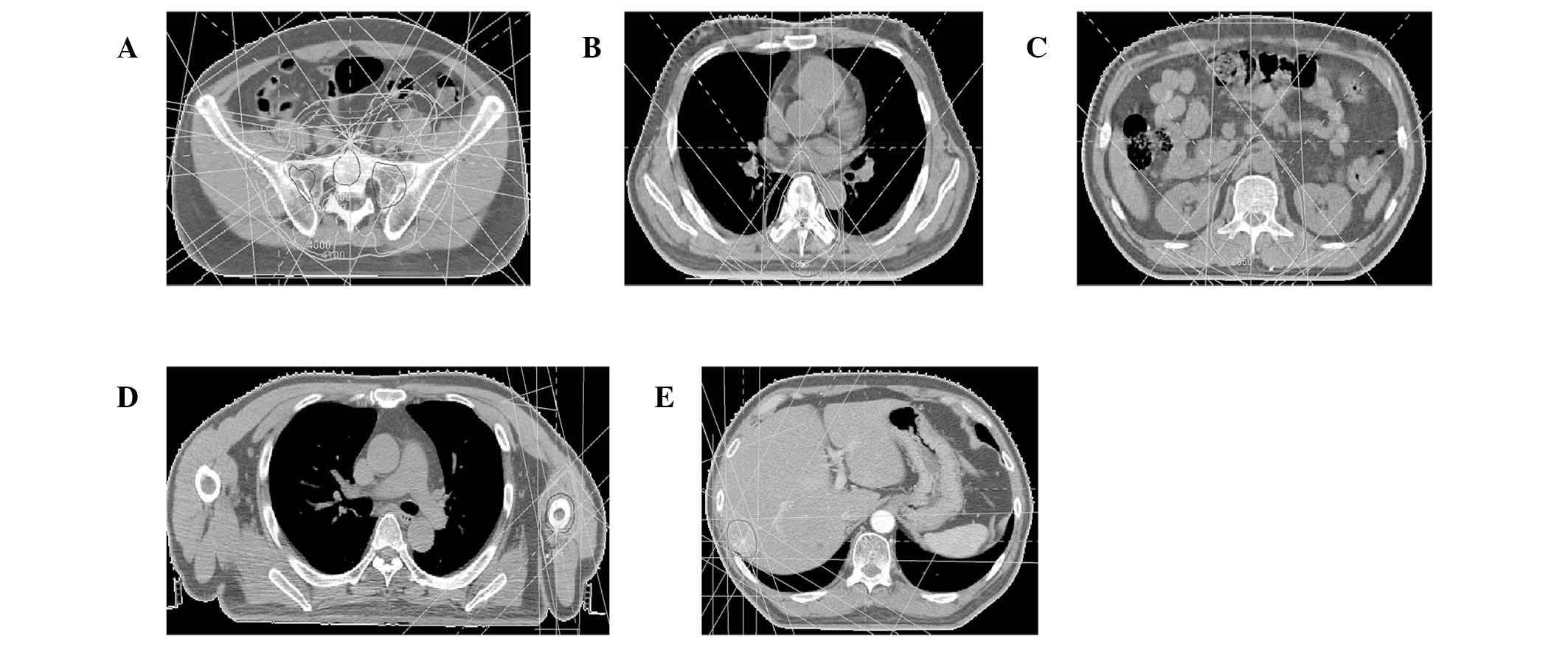
as RT with 54 Gy/30 fractions/6 weeks to inguinal LNs (Fig. 3A) and 30 Gy/10 fractions/2 weeks to
T6 and T12-L2, respectively (Fig. 3B
and C). A partial response was achieved following two cycles
(Fig. 1C).
The patient tolerated only two cycles of
chemotherapy concomitant with RT, following which his condition
deteriorated due to grade IV bone marrow suppression and poor
performance status. Thereafter, the patient was treated with a
third cycle of chemotherapy with reduced concentrations of
irinotecan (70 mg/m2, days 1, 8, 15) and cisplatin (30
mg/m2, days 1–3). Following five cycles of chemotherapy
concomitant with RT, the mass in his right groin resolved, the
metastatic diseases disappeared and complete response was observed
(Fig. 1D).
The patient demonstrated no evidence of disease for
4 months when a subcutaneous mass was identified. Subsequently,
PET-CT follow-up revealed that the patient’s liver and humerus had
metastatic disease (Fig. 1E). Mohs
micrographic surgery and salvage chemotherapy plus RT (Fig. 3D and E) were then instituted, but
the patient succumbed to liver failure 21 months following the
onset of his illness.
Literature review
Search strategy
Articles were identified by searching PUBMED/MEDLINE
between January 1966 and April 2012 using the key words: ‘Merkel
cell carcinoma’ or ‘Merkel cell cancer’ or ‘MCC’ without language
restriction. Computer searches were supplemented with hand
searching journals up to April 2012. We also hand searched the
general reviews and references from published clinical trials.
Common characteristics
Six studies were identified which reported 23
patients with LN metastatic MCC in the absence of a primary site
(12–17). Of these patients, 8/23 (34.8%) came
from Italy and the rest from the USA. The average ages of the
patients were between 50 and 80 years; the majority were elderly,
but two were aged <40 years. There were similar numbers of males
and females: 13 males, 10 females. The most common sites of origin
were the inguinal LNs (17/23, 73.9%), 3 cases demonstrated axillary
LNs (3/23, 13.0%). The other sites of origin were neck area LNs
(2/23, 8.7%), the submandibular lymph (1/23, 4.3%), the cervical LN
(1/23, 4.3%) and the upper jugular area LN (1/23, 4.3%). Three
histological patterns of MCC were reported: a solid (8/23, 34.8%),
a diffuse (4/23, 17.4%) and a trabecular type (1/23, 4.3%). Local
recurrences were identified in 5 patients (21.7%), 6 (26.1%)
sustained extraregional metastases and 5 (21.7%) had distant
spreading (Table I).
 | Table I.Clinical findings of Merkel cell
carcinoma with lymph node metastasis in absent of a primary
site. |
Table I.
Clinical findings of Merkel cell
carcinoma with lymph node metastasis in absent of a primary
site.
| First author
(Ref.) | Case no. | Age (years) | Gender | Site | Histol. type | Skin site of
primary | Local recur.
(months) | Extraregio. or
distant spread (months) | Treatment | Follow-up
(months) |
|---|
| Kaplan et al
(12) | 1 | Elderly | M | Axilla LN, L and
R
Cervical LN, R | S | UK | UK | Brain, liver and
adrenal gland, syn. | RT | DOD (4) |
| Pilotti et
al (13) | 2 | 50 | M | Inguinal LN, R | D | UK | UK | Retroperit. and
pancreas, syn. | RT | ED 6) |
| 3 | 58 | M | Inguinal LN, R | S | UK | UK | UK | SE | NED (5) |
| 4 | 65 | M | Inguinal LN, R | S | UK | UK | UK | SE | NED (18) |
| 5 | 73 | M | Inguinal LN, R | S | UK | UK | UK | SE | ED (36) |
| 6 | 66 | M | Inguinal LN, R | D | UK | UK | UK | SE | DOC (168) |
| 7 | 65 | F | Inguinal LN, R | T | UK | UK | UK | UK | Cons |
| 8 | 39 | F | Inguinal LN, R | S | UK | UK | UK | SE | Cons |
| 9 | 53 | F | Inguinal LN, L | S | UK | 6 | UK | SE | NED (8) |
| 10 | 78 | M | Inguinal LN, L | D | UK | UK | Supraclav. LN, L
(48) | CT | DOD (60) |
| 11 | 52 | F | Axilla LN, R | D | UK | UK | UK | SE | NED (30) |
| Eusebi et al
(14) | 12 | 65 | F | Axilla LN, L | UK | UK | UK | UK | RT+CT | NED (6) |
| 13 | 46 | M | Inguinal LN, L | UK | UK | UK | UK | UK | NED (10) |
| 14 | 37 | M | Inguinal LN, R | UK | UK | 6 | Pelvic LN, R
(12)
Cervical LN, R (15) | RT+CT | DOD (25) |
| 15 | 46 | F | Inguinal LN, L | UK | UK | UK | UK | UK | NED (19) |
| 16 | 64 | M | Inguinal LN, L | UK | UK | 11 | UK | UK | NED (25) |
| 17 | 68 | F | Inguinal LN, L | UK | UK | UK | Paraortic LN, R
(3)
Parailliac LN, L (3) | UK | DOD (8) |
| 18 | 80 | F | Submandibular LN,
L | UK | UK | UK | UK | UK | NED (26) |
| 19 | 54 | F | Inguinal LN, L | UK | UK | 5 | Iliac LN, L
(12) | RT+CT | ED (12) |
| Rice et al
(15) | 20 | 76 | M | Upper jugular area
LN, R | S | UK | UK | UK | SE+RT | NED (23) |
| Yang et al
(16) | 21 | 74 | M | Neck LN, R | UK | UK | UK | Submandibular
gland, syn. | SE+RT | DOD (12) |
| Straka and Straka
(17) | 22 | 71 | F | Neck LN in zone II,
R | UK | UK | 10 | Submandibular
gland, syn. brain (10) | SE+RT+CT | DOD (12) |
| 23 | 52 | M | Inguinal LN, L | S | UK | UK | UK | SE+CT | UK |
| Zhao and Meng
(TS) | 24 | 54 | M | Inguinal LN, R | S | Dorsi-thigh, R | UK | Vertebrae
(1)
Humerus and liver (12) | SE+RT+CT | DOD (21) |
Treatment schedule
Of the 23 patients included in this study, 7 (30.4%)
underwent surgical excision alone and the remaining patients were
treated with chemotherapy alone (1/23, 4.3%), surgical excision
plus chemotherapy (1/23, 4.3%), surgical excision plus RT (2/23,
8.7%), RT plus chemotherapy (3/23, 13.0%), surgical excision plus
chemotherapy plus RT (2/23, 8.7%) and unknown (6/23, 26.1%).
Chemotherapy was administered to a total of 7
patients (30.4%) with LN metastatic MCC in the absence of primary
site. A two-drug regimen was recieved by 5 patients, 1 received
single-agent chemotherapy and in 1 patient, the chemotherapy
regimen was unknown. Etopoplatin with either cisplatin or
carboplatin were used for combination chemotherapy and the majority
of patients had chemotherapy following surgical excision (Table I).
Overall survival rate and
recurrence
With a median follow-up of 18 months, a total of 12
patients (52.17%) survived to the final follow-up: 10 patients were
alive with no evidence of disease, 2 were alive with disease and
the remaining 11 had succumbed to the disease. Of the 23 total
patients, 5 experienced recurrences during follow-up. Due to the
small sample size, no prognostic factor was identified to be
correlated with poor survival rates by univariate and multivariate
analyses. The survival rate of patients ranged from 4 to 168 months
and the median was estimated to be 60 months (Table I).
Discussion
To the best of our knowledge, this is the first case
report of an Asian patient with MCC and multiple metastases in the
absence of a primary site. LN metastases as the initial clinical
manifestation of MCC were unexpected, suggesting that diagnosis may
difficult. Outcomes of our patient and those of the other 23
reported cases demonstrated that although multi-modal treatment
with surgery, RT and chemotherapy provides excellent local control,
local recurrence and distant metastases commonly develop in this
uncommon tumour. Therefore, LN metastatic MCC in the absence of a
primary site is a highly malignant disease and the role of adjuvant
postoperative RT and/or chemotherapy remains to be fully
determined.
At the time of diagnosis, patients with MCC
typically present with a flesh-coloured, red or blue, firm,
nontender, intracutaneous mass, which may be ulcerated (18). Owing to its nonspecific appearance,
diagnosis of MCC is often made by biopsy. In the present case, an
initial histological examination of a biopsy specimen from the
right inguinal LNs demonstrated a metastatic small cell carcinoma.
However, histological examination of a biopsy specimen from the
right dorsal thigh revealed nodules and diffuse sheets of
basophilic cells with imperceptible cytoplasm and round or oval
vesicular nuclei, the dispersed chromatin yielding a pathognomonic
watery appearance. To confirm the diagnosis, immunohistochemistry
studies, including staining for CK20, CK7, TTF-1, LCA, S100 and
CD99, were performed. In general, MCC cases express CK20 rather
than CK7, the latter identifying bronchial small cell carcinoma
(19). Notably, in the present case
CK20 and CK7 were identified, an unusual presentation of this rare
tumour. Immunohistochemistry produced a negative result for TTF-1,
which is expressed at high levels in small cell carcinoma of the
lung. Immunohistochemistry also demonstrated a marked positive
reaction for CD99 rather than TTF-1, LCA, S100 in cutaneous
tissues, which indicated that the differential diagnosis includes
small cell carcinoma of the lung, lymphoma, peripheral primitive
neuroectodermal tumour and small cell melanoma. However, an
extensive analysis revealed no primary tumour at any site in the
patient. Therefore, the morphology of the small cell tumour in this
case, ultrastructural evidence of its neuroendocrine granules and
the immunohistochemistry results were indicative of MCC.
Currently, there is no standard approach to the
management of MCC in the absence of a primary site. Mohs
micrographic surgery is currently considered as the primary and
complementary measure for controlling this serious disease. Since
the disease is highly aggressive and the high failure rate
following surgery alone, RT is usually administered as temporary
support for numerous patients with MCC. MCC cell lines have been
demonstrated to be radiosensitive in vitro (20). Results have indicated that adjuvant
RT, following initial surgery and resection for recurrent MCC and
palliation is beneficial (21). A
previous study reported that a radiation dose of 45 Gy had
significant impact on local control and prolonged survival in nine
patients, whereas a subset of 7 patients who received <45 Gy had
a poorer outcome (22). Our patient
received 54, 30, 50, 30 and 30 Gy for inguinal LNs, vertebrae,
right dorsal thigh, humerus and liver, respectively.
MCC was initially considered to be resistant to
chemotherapy, however, various agents have been used to treat MCC
with variable results; the most commonly used chemotherapy regimen
is etoposide/cisplatin (EP regimen) (23). However, our patient responded
successfully to an irinotecan/cisplatin (IP) regimen with RT,
previously following an EP regimen alone. The majority of patients
with MCC are elderly and may be intolerant of high doses of
chemotherapy (24). For example,
our patient tolerated only two cycles of the IP regimen concomitant
with RT, following which his condition deteriorated owing to grade
IV bone marrow suppression. As his general condition gradually
improved, the patient received a third cycle of the IP regimen but
at decreased concentrations, which may have affected treatment
efficacy. Although multi-modal treatment with surgery, RT and
chemotherapy results in excellent local control, local recurrence
and distant metastases ultimately developed, possibly owing to the
characteristics of MCC or inadequate treatment. Therefore, the role
of adjuvant postoperative chemotherapy and/or RT in MCC remains to
be determined in a future controlled trial.
Since 2001, PET-CT has rapidly replaced standalone
PET (25,26). The diagnostic capability of PET-CT
in the staging of cancer is improved compared with that of CT alone
or PET alone (27) as it enables
more accurate assignment of tumour stage and, to a lesser extent,
definition of the lymph-node stage. In the present study,
identifying the primary tumour aided the determination of the
appropriate treatment and was essential for prognosis (27). The patient was followed-up for 15
months by PET-CT following the initial treatment and we identified
that adding a PET-CT examination to the diagnostic regimen improved
sensitivity in determining the primary tumour and metastases. To
summarise, although MCC may be suggested by immunohistochemistry
and electron microscopic features, caution should be exercised in
making this diagnosis in the absence of a known primary skin
tumour. Multimodal treatment with surgery, RT and chemotherapy
provides excellent local control, however, local recurrence and
distant metastases commonly develop in patients with metastatic MCC
in the absence of a primary site. Finally, metastatic MCC in the
absence of a primary site is a highly malignant disease and the
role of adjuvant postoperative RT and/or chemotherapy in MCC
remains to be determined in a controlled trial.
Acknowledgements
The authors thank the doctors
responsible for the care of the patient in the present case study
and an anonymous referee for his/her helpful comments, which
considerably improved the quality of this manuscript.
References
|
1.
|
C TokerTrabecular carcinoma of the
skinArch
Dermatol105107110197210.1001/archderm.1972.01620040075020
|
|
2.
|
RW MillerCS RabkinMerkel cell carcinoma
and melanoma: Etiological similarities and differencesCancer
Epidemiol Biomarkers Prev8153158199910067813
|
|
3.
|
U Meyer-PannwittK KummerfeldtP BoubarisJ
CaselitzMerkel cell tumour or neuroendocrine skin
carcinomaLangenbecks Arch Chir3823493581997(In German)
|
|
4.
|
M PoulsenMerkel-cell carcinoma of the
skinLancet Oncol5593599200410.1016/S1470-2045(04)01593-1
|
|
5.
|
ML HaagLF GlassNA FenskeMerkel cell
carcinoma: diagnosis and treatmentDermatol
Surg21669683199510.1111/j.1524-4725.1995.tb00269.x7633811
|
|
6.
|
JL DeneveJL MessinaSS MarzbanMerkel cell
carcinoma of unknown primary originAnn Surg
Oncol1923602366201210.1245/s10434-011-2213-222271206
|
|
7.
|
R GollardR WeberMP KostyHT GreenwayV
MassulloC HumbersonMerkel cell carcinoma: Review of 22 cases with
surgical, pathologic and therapeutic
considerationsCancer8818421851200010.1002/(SICI)1097-0142(20000415)88:8%3C1842::AID-CNCR13%3E3.0.CO;2-P10760761
|
|
8.
|
WJ O’ConnorRK RoenigkDG BrodlandMerkel
cell carcinoma: Comparison of Mohs micrographic surgery and wide
excision in eighty-six patientsDermatol Surg2392993319979357504
|
|
9.
|
A YiengpruksawanDG CoitHT ThalerC
UrmacherWK KnapperMerkel cell carcinoma: Prognosis and
managementArch
Surg12615141519199110.1001/archsurg.1991.014103600880141842182
|
|
10.
|
P SavageD ConstenlaC FisherJM ThomasME
GoreThe natural history and management of Merkel cell carcinoma of
the skin: A review of 22 patients treated at the Royal Marsden
HospitalClin Oncol (R Coll
Radiol)9164167199710.1016/S0936-6555(97)80073-89269548
|
|
11.
|
D PectasidesM PectasidesA PsyrriA
KoumarianouN XirosE PectasidesCisplatin-based chemotherapy for
merkel cell carcinoma of the skinCancer
Invest24780785200610.1080/0735790060106235417162559
|
|
12.
|
GP KaplanMJ BookbinderDR HoodSL
BridgersMerkel cell tumour of the skinHum
Pathol19615616198810.1016/S0046-8177(88)80219-3
|
|
13.
|
S PilottiF RilkeC BartoliA
GrisottiClinicopathologic correlations of cutaneous neuroendocrine
Merkel cell carcinomaJ Clin Oncol161863187319883199169
|
|
14.
|
V EusebiC CapellaA CossuJ
RosaiNeuroendocrine carcinoma within lymph nodes in the absence of
a primary tumour with special reference to Merkel cell carcinomaAm
J Surg
Pathol16658666199210.1097/00000478-199207000-000041530107
|
|
15.
|
RD RiceGD ChonkichKS ThompsonDR
ChaseMerkel cell carcinoma of the head and neck. Five new cases
with literature reviewArch Otolaryngol Head Neck
Surg119782786199310.1001/archotol.1993.018801900780168318209
|
|
16.
|
GC YangMJ SchneckRE HaydenPK GuptaMerkel
cell tumour-like neuroendocrine carcinoma associated with the
submandibular glandActa Cytol3874274619948091909
|
|
17.
|
JA StrakaMB StrakaA review of Merkel cell
carcinoma with emphasis on lymph node disease in the absence of a
primary siteAm J
Otolaryngol185556199710.1016/S0196-0709(97)90050-89006679
|
|
18.
|
CL HitchcockKI BlandRG Laney IIID
FranziniB HarrisEM Copeland IIINeuroendocrine (Merkel cell)
carcinoma of the skin: Its natural history, diagnosis and
treatmentAnn
Surg207201207198810.1097/00000658-198802000-000153277546
|
|
19.
|
W CheukMY KwanS SusterJK
ChanImmunostaining for thyroid transcription factor 1 and
Cytokeratin 20 aids the distinction of small cell carcinoma from
Merkel cell carcinoma, but not pulmonary from extrapulmonary small
cell carcinomasArch Pathol Lab Med125228231200111175640
|
|
20.
|
JH LeonardJR RamsayJH KearsleyGW
BirrellRadiation sensitivity of Merkel cell carcinoma cell linesInt
J Radiat Oncol Biol
Phys3214011407199510.1016/0360-3016(94)00610-W7635780
|
|
21.
|
W GoesslingPH McKeeRJ MayerMerkel cell
carcinomaJ Clin Oncol20588598200210.1200/JCO.20.2.588
|
|
22.
|
MJ OttKK TanabeMA GaddP StarkBL SmithDM
FinkelsteinMultimodality management of Merkel cell carcinomaArch
Surg134388393199910.1001/archsurg.134.4.38810199311
|
|
23.
|
PG AllenWB BowneDP JaquesMF BrennanK
BusamDG CoitMerkel cell carcinoma: prognosis and treatment of
patients from a single institutionJ Clin
Oncol2323002309200510.1200/JCO.2005.02.32915800320
|
|
24.
|
PT TaiE YuE WinquistA HammondL StittJ
TonitaJ GilchristChemotherapy in neuroendocrine/Merkel cell
carcinoma of the skin: Case series and review of 204 casesJ Clin
Oncol1824932499200010856110
|
|
25.
|
T BeyerDW TownsendT BrunPE KinahanM
CharronR RoddyA combined PET/CT scanner for clinical oncologyJ Nucl
Med4113691379200010945530
|
|
26.
|
GK von SchulthessCost considerations
regarding an integrated CT-PET systemEur Radiol10Suppl
3S377S380200011001451
|
|
27.
|
D LardinoisW WederT HanyEM KamelS KoromB
SeifertStaging of non-small-cell lung cancer with integrated
positron-emission-tomography and computed tomographyN Engl J
Med34825002507200310.1056/NEJMoa02213612815135
|
|
28.
|
G AntochJ StattausAT NematS MarnitzT
BeyerH KuehlNon-small cell lung cancer: dual-modality PET/CT in
preoperative
stagingRadiology229526533200310.1148/radiol.229202159814512512
|