Introduction
Intrathoracic anastomotic leakage is an extremely
intractable complication that occurs following esophagectomy, with
an incidence that ranges from 1.3 to 5.1% (1–3). The
mortality rate is 12–46.2% (1–3). In
general, the effect of conservative treatments, including
conventional chest tube drainage, nasogastric decompression and
nutritional support, is often poor, particularly in patients with
adhesions of the pleural cavity and multiloculated empyema
(1–4). This study describes the combined
application of medical thoracoscopy followed by gastroscopy for the
treatment of an intrathoracic anastomotic leak in two patients. The
study was approved by the IRB of Sun Yat-sen University Cancer
Center. Consent was obtained from both of the patients.
Case reports
Case 1
A 58-year-old male patient with middle-third
thoracic esophageal squamous carcinoma was confirmed to have an
intrathoracic anastomotic leak 10 days after esophagectomy and a
right-sided contained empyema 4 weeks after esophagectomy. The
condition of the patient did not improve following jejunostomy,
conventional chest tube drainage and gastrointestinal decompression
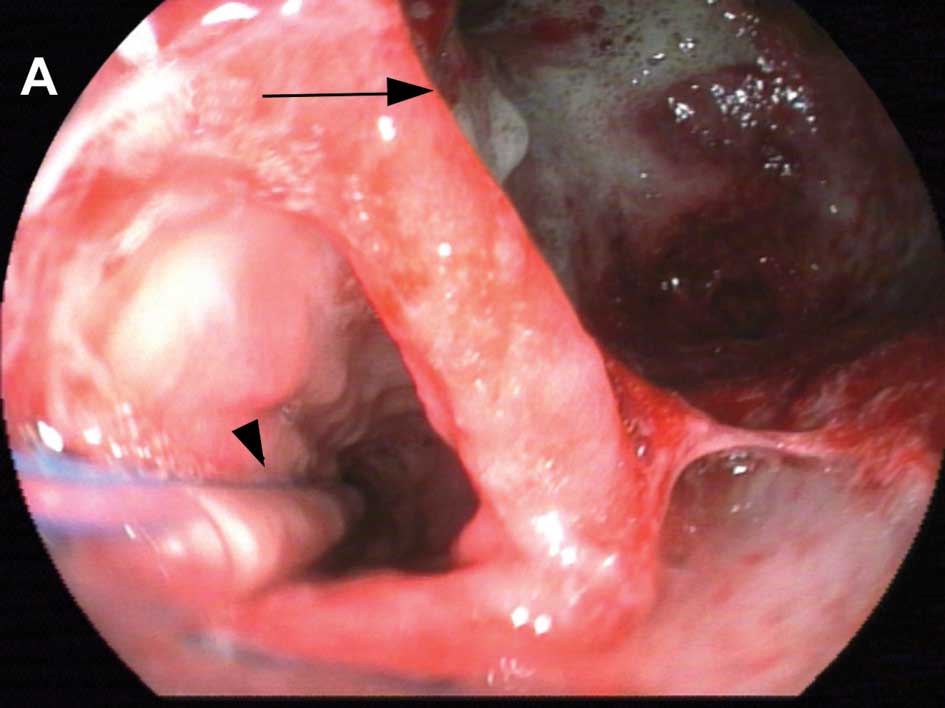
for 8 weeks. Gastroscopy (Fig. 1A)
confirmed that a large intrathoracic anastomotic leak existed in
the posterior right-sided wall of the esophagus. Two nasogastric
tubes were then respectively placed into the residual stomach and
the sump around the leak. A computed tomography scan was performed
prior to thoracoscopy in order to select the incision accurately to
facilitate exploration, debridement and drainage. Thoracoscopy was
then performed under continuous sedation and local anesthesia. The
port was inserted through a trocar via an incision on the right
mid-clavicular line, between the second and third inter-costal
spaces. These adhesions and septations were dissected with biopsy
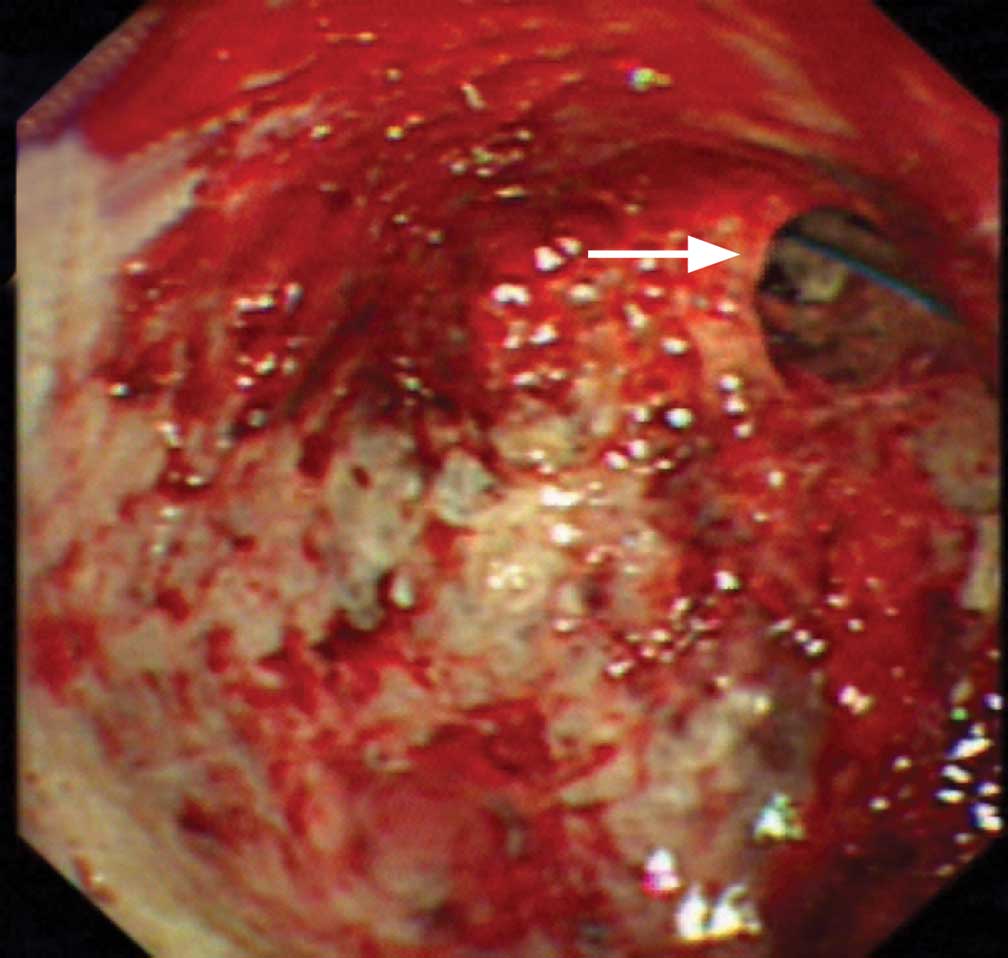
forceps and electrocautery. After removing the infected focus, the
anastomotic leak could be observed at the upper pole of the empyema
cavity with some refluxed stomach content. The lateral side of the
nasogastric tube entering the sump around the leak could also be
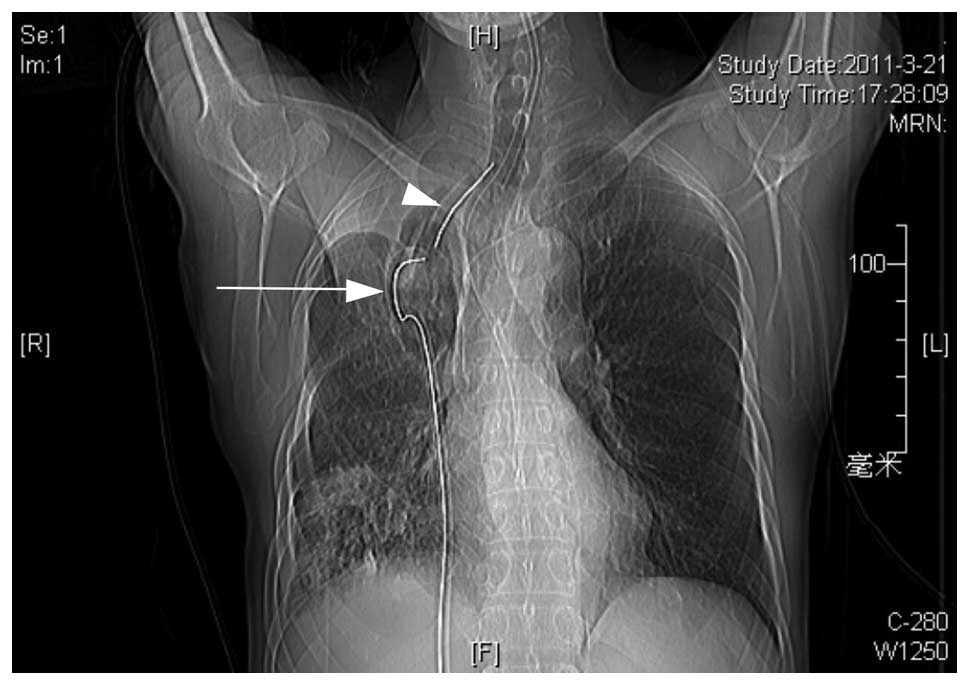
visualized through the anastomotic leak (Fig. 2). After the infected focus and
digestive secretions around the anastomotic leak were completely
removed, a chest tube was placed into the sump around the
anastomotic leak (Fig. 3). The
correct orientation of the chest tube was attained by slowly
adjusting the head direction of the flexible thoracoscope and the
chest tube replaced a cytology brush catheter via the thoracoscope.
Postoperatively, the patient continued to receive conservative
treatments and chest lavage. A barium and chest radiography
confirmed the closure of the anastomotic leak and right lung
re-expansion 3 months after the combined procedure. Gastroscopy
revealed closure of the anastomotic leak and a small residual sump
(Fig. 1B) 5 months after the
combined procedure.
Case 2
A 50-year-old male patient with middle-third
thoracic esophageal squamous carcinoma was confirmed to have an
intrathoracic anastomotic leak and a right-sided contained empyema
13 days after esophagectomy. Therefore, the combined application of
thoracoscopy and gastroscopy was performed, as described in Case 1.
The trocar was inserted through an incision on the right
parasternal line between the third and fourth intercostal spaces.
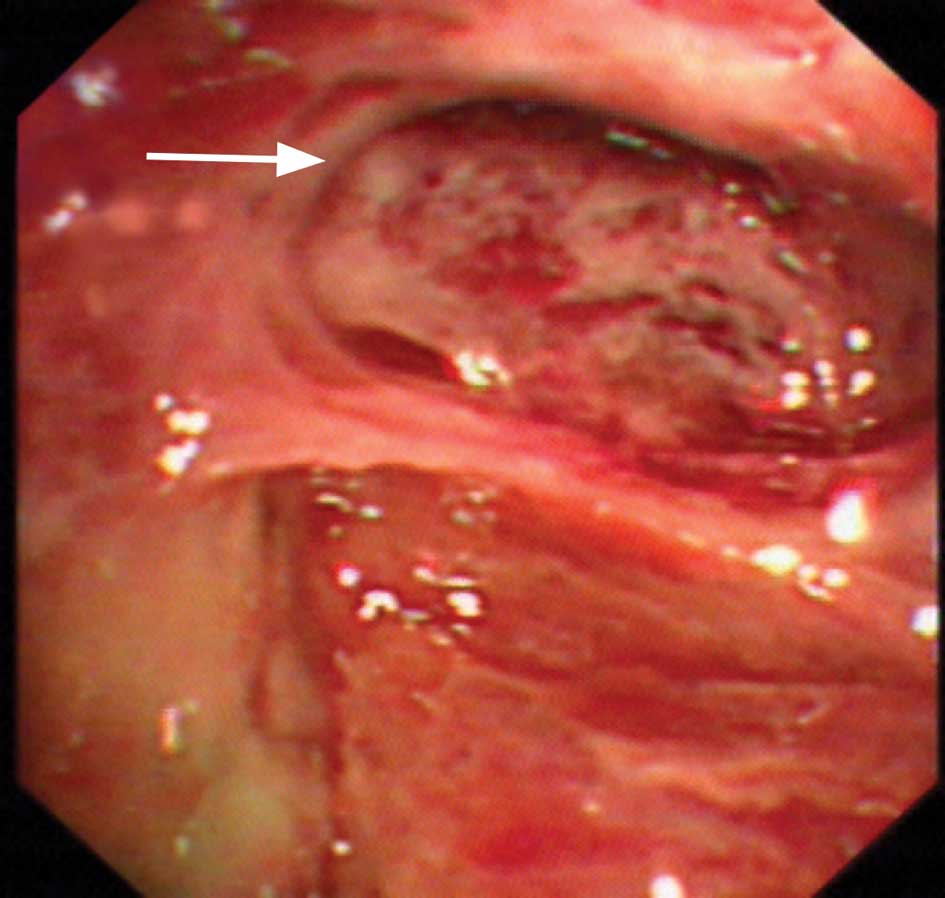
The purulent pleural effusion and fibrinopurulent focus were
completely removed under direct vision. The sump around the
anastomotic leak could then be observed at the superiolateral pole
of the empyema cavity (Fig. 4). A
chest tube was placed at the lowest aspect of the empyema cavity.
Pleural cavity lavage was then performed through the chest tube.
The condition of the patient improved 2 weeks after the combined
procedure.
Discussion
Intrathoracic anastomotic leaks may easily cause
multi-loculated and contained empyemas. In general, the effect of
conservative treatments, including conventional chest tube
drainage, nasogastric decompression and nutritional support, is
poor in such patients (1–4). This study describes two patients with
an anastomotic leak post-esophagectomy, who underwent medical
thoracoscopy. The septations in the multiloculated empyema were
reliably dissected under direct vision, and the fibrinopurulent
debris and digestive fluids were completely removed. Additionally,
thoracoscopy enabled the chest drainage tubes to be placed in
suitable sites and the chest lavage could therefore be
appropriately performed intra- and postoperatively. Combined
thoracoscopic and gastroscopic interventions led to favorable
environments both intra- and extraluminally, which facilitated
healing and removed the majority of infection within the pleural
cavity. This promoted lung re-expansion and improvements in lung
function.
Medical thoracoscopy compared with visually-assisted
thoracic surgery is minimally invasive and inexpensive. It does not
require general anesthesia and double-lumen intubation, which leads
to shorter hospitalization times and yields better cosmetic
results. Above all, it is a more advisable procedure in frail
patients who have high levels of surgical risk (4,5).
Although our study presents a small number of patients, the
combined application of gastroscopy and thoracoscopy for the
treatment of intrathoracic anastomotic leak may be an effective,
safe and minimally-invasive procedure.
References
|
1
|
Jiang F, Yu MF, Ren BH, et al: Nasogastric
placement of sump tube through the leak for the treatment of
esophagogastric anastomotic leak after esophagectomy for esophageal
carcinoma. J Surg Res. 171:448–451. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Turkyilmaz A, Eroglu A, Aydin Y, et al:
The management of esophagogastric anastomotic leak after
esophagectomy for esophageal carcinoma. Dis Esophagus. 22:119–126.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Junemann-Ramirez M, Awan MY, Khan ZM, et
al: Anastomotic leakage for esophageal post-esophagogastrectomy
carcinoma: retrospective analysis of predictive factors, management
and influence on long-term survival in a high volume centre. Eur J
Cardiothorac Surg. 27:3–7. 2005.
|
|
4
|
Tassi GF, Davies RJ and Noppen M: Advanced
techniques in medical thoracoscopy. Eur Respir J. 28:1051–1059.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kern L, Robert J and Brutsche M:
Management of parapneumonic effusion and empyema: medical
thoracoscopy and surgical approach. Respiration. 82:193–196. 2011.
View Article : Google Scholar : PubMed/NCBI
|