Introduction
Multiple primary cancers are relatively uncommon.
The present study reports a case in which synchronous
nasopharyngeal undifferentiated non-keratinizing carcinoma and
cardia adenocarcinoma were diagnosed. During the therapy course,
progressive painless symmetric proximal muscle weakness and a skin
rash emerged and were accompanied with dysphasia. In addition,
suspected dermatomyositis (DM) was diagnosed. DM developed
progressively in spite of application of methylprednisolone until
the patient succumbed to nutritional deterioration on May 6, 2012.
We present this case with two noteworthy aspects. Firstly,
synchronous nasopharyngeal undifferentiated non-keratinizing
carcinoma and cardia adenocarcinoma are relatively uncommon; and
secondly the coexistance of multiple primary cancers with DM is
extremely rare and indicative of poor prognosis.
Case reports
Clinical presentation
The patient was a 64-year-old male from Sichuan,
China. Prior to admittance in January 2012, the patient had
experienced tinnitus of the right ear for one year and bloody nasal
mucus for two months. A tumor was identified on the right and top
wall of the nasopharynx by magnetic resonance imaging (MRI) and
nasopharyngeal mirror. MRI also revealed that the right pharynx was
absent and the right base of the skull had been destroyed by the
tumor. Pathological results of the tumor confirmed that it was
nasopharyngeal undifferentiated non-keratinizing carcinoma. Two
hard lymph nodes in the right neck, with an approximate diameter of
2 cm, were identified by physical examination. Comprehensive
examination of the patient was performed. Abdominal computer
tomography (CT) revealed multiple nodules in the liver, indicative
of metastasized lesions. The diameter of these nodules ranged
between 2 and 3 cm. In addition, CT revealed a thicker than normal
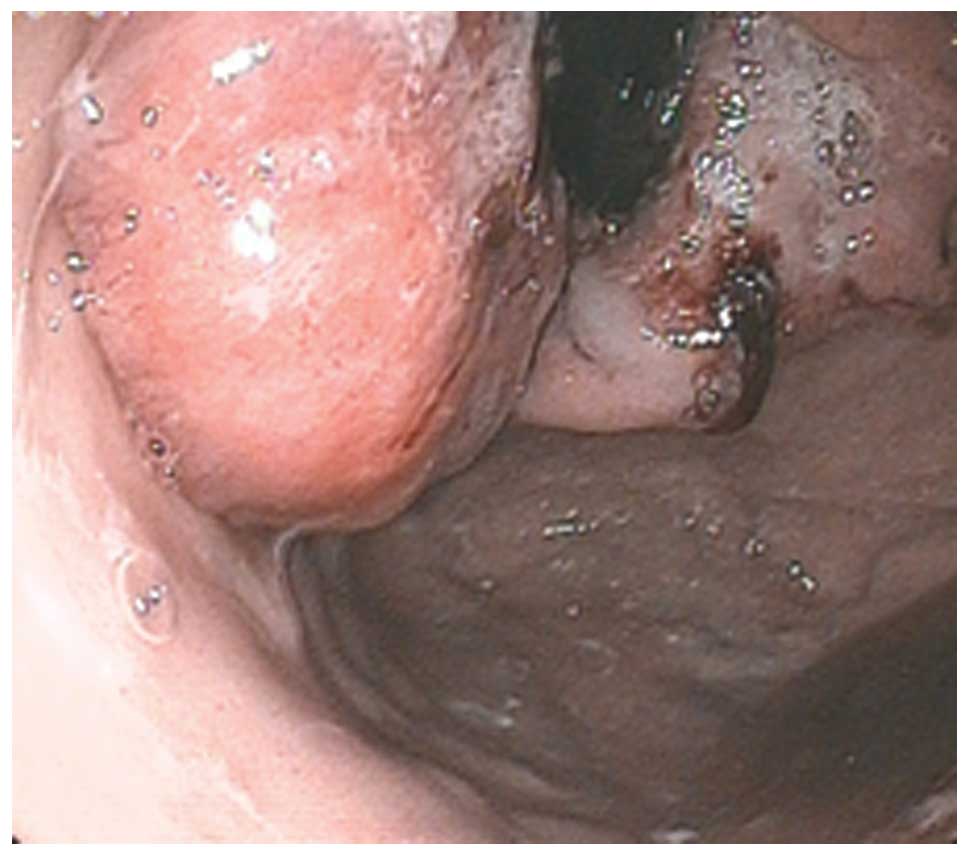
cardia tube wall. Gastroscopy was performed and a large neoplasm
was identified surrounding almost the entire diameter of the cardia
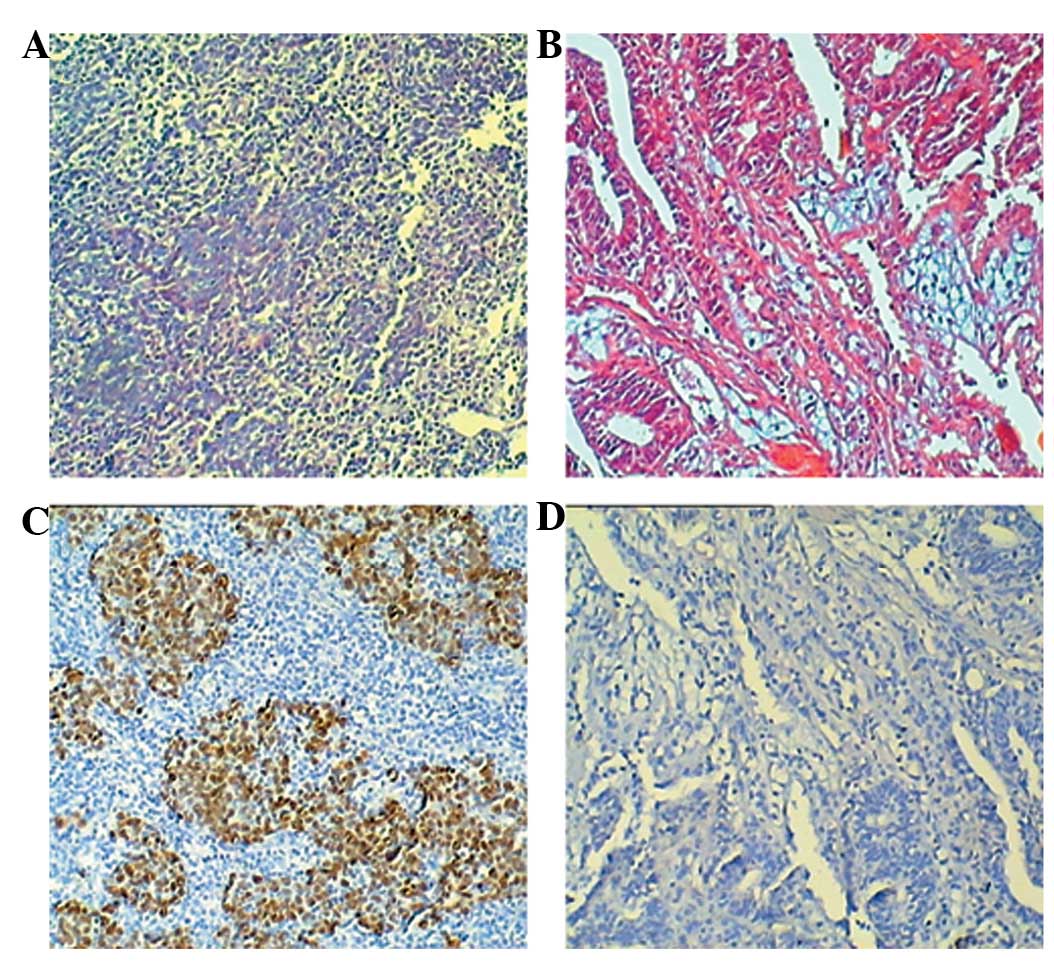
(Fig. 1). Pathological analyses
were consistent with the diagnosis of cardia adenocarcinoma. In
situ Epstein-Barr virus (EBV)-encoded small RNA (EBER)
detection demonstrated that the nasopharyngeal carcinoma cells were
positive and cardia carcinoma cells were negative for EBER
(Fig. 2). The study was approved by
the ethics committee of Sichuan Provincial People’s Hospital,
Chengdu, China, and written consent was obtained from the patient’s
family
Treatment and clinical course
The patient received 2 cycles of chemotherapy as
follows: lipid body paclitaxel was administered at a dose of 210 mg
on day 1; nedaplatin was administered at a dose of 50 mg on day 1,
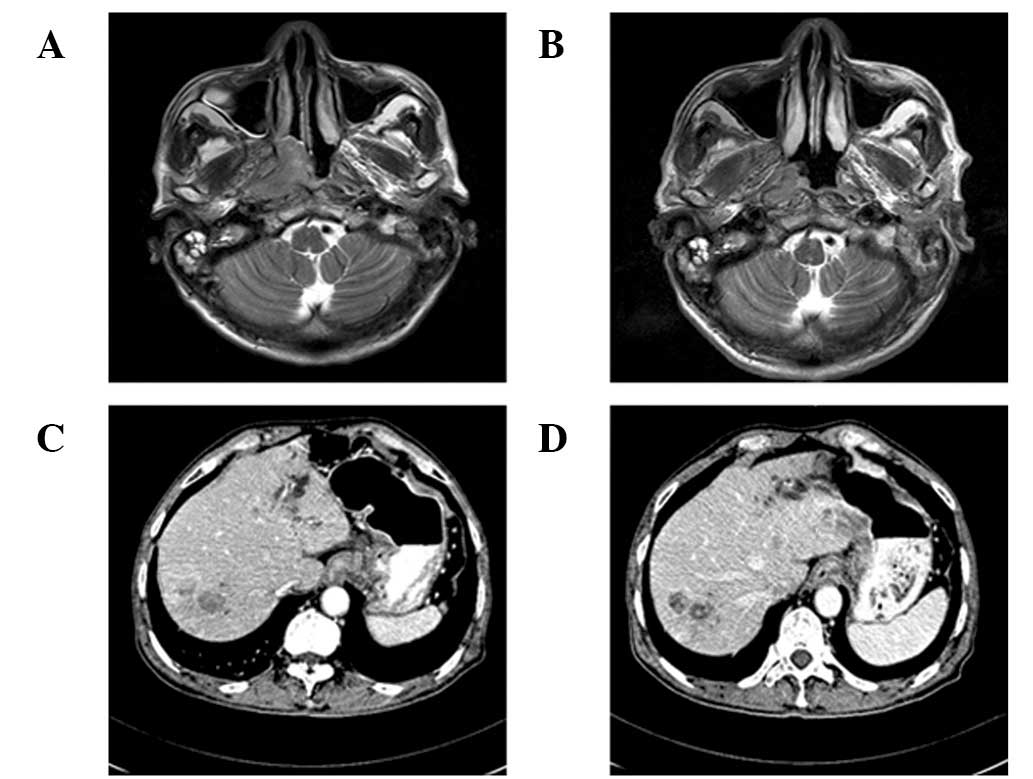
2 and 3. Courses were repeated every 21 days. MRI and CT scans were
repeated to evaluate the effects of chemotherapy. MRI demonstrated
that the nasopharyngeal tumor had shrunk and CT revealed that the
nodules of liver and tumor of cardia remained stable (Fig. 3). Following two cycles of
chemotherapy, rashes were identified on the back of the neck of the
patient. Rashes gradually diffused to the hands and face and formed
erythema with dander (Fig. 4).
Specific anti-allergy drugs were administered to the patient but
had limited effect on the erythema. During the third cycle of
chemotherapy, proximal limb muscle strength of the patient
decreased without pain and presented as difficulty in climbing
steps, rising from a chair, lifting objects and combing hair. This
observation was also accompanied by dysphasia. Serum creatine
kinase levels were analyzed and detected at 214 U/l (normal value,
26–174 U/l). A previous study by Bohan and Peter (1) reported suspected dermatomyositis,
however, muscle biopsy was refused by the patient and result of
electromyography test was normal. The present patient received
intravenous infusion of methylprednisolone 40 mg/day but limited
alleviation of symptoms was observed. The characteristic symptoms
of dermatomyositis advanced and the patient deteriorated rapidly
and succumbed to nutritional deterioration on May 6, 2012.
Discussion
Multiple primary cancers are relatively uncommon. In
a Japanese large-scale survey, approximately 4.2% of patients were
diagnosed with synchronous multiple primary cancers upon initial
admission to the hospital (2).
Analysis of the etiology of multiple primary cancers is important
for understanding a number of factors, including genetic
susceptibility and common exposure status (exposure to an agent
carcinogenic to both sites) and may prove valuable in tumor
prevention and treatment. Patients with Li-Fraumeni syndrome (a
dominantly inherited disorder) or a history of cigarette and
alcohol consumption are associated with a high risk of developing
multiple primary cancers (3,4). EBV
is a member of the herpes virus family. Currently, three EBV
nuclear antigens are associated with cancer development, EBNA-1 and
-3C and LMP-1. These antigens promote genomic instability, increase
the rate of somatic hypermutations and obstruct apoptotic pathways.
Nasopharyngeal non-keratinizing carcinomas are markedly associated
with EBV. In addition, EBV is correlated with a number of other
types of cancer, including Burkitt’s, Hodgkin’s and non-Hodgkin’s
lymphoma, gastric carcinoma and leiomyosarcomas. A previous study
reported detection of EBV in more than 90% of gastric
lymphoepithelioma-like carcinomas and 5–25% of gastric
adenocarcinomas (5). Following
synchronous nasopharyngeal carcinoma and cardia adenocarcinoma
diagnosis of the present patient, a hypothesis emerged associating
the two tumors with EBV. However, results of EBER detection were
not consistent with this hypothesis. The nasopharyngeal
non-keratinizing carcinoma was identified as EBV-positive, however,
the cardia adenocarcinoma was negative for EBV. Results of the
literature review revealed that EBV-associated multiple primary
cancers (defined as the positive detection of EBV in all primary
cancers) is extremely rare. Wang et al analysed the
correlation between the ratio of second primary tumors with
nasopharyngeal carcinoma and EBV. The group identified that gastric
cancer was the second leading second primary tumor in
nasopharyngeal non-keratinizing carcinoma patients. However, the
results also demonstrated that only 1/11 second primary gastric
cancer specimens were EBV-positive and an increased detection of
EBV was not reported (6). The
majority of adult individuals are infected with EBV (95%), however,
only a small number of these cases develop into malignances. The
distribution of EBV-associated cancers is geography defined.
EBV-related Burkitt’s lymphoma occurs primarily in regions of
equatorial Africa. Nasopharyngeal carcinoma is rare in most parts
of the world, however, it is prevalent in South China, indicative
of additional factors important for the development of specific
types of tumors. Although EBV infection is correlated with a number
of tumor types, it is not currently considered to be sufficient for
the induction of cancer alone, instead it appears to promote the
induction of tumorigenesis by additional oncogenic factors.
DM is an autoimmune disorder characterized by
inflammatory muscular and cutaneous disease. Individuals with DM
have a high risk of developing a malignancy. It is currently
estimated that 8–60% of individuals with DM also have cancer
(7). Malignancies have been
identified prior to, following and in tandem with DM diagnosis and
are most commonly identified one year following diagnosis.
Cross-immune responses against myositis autoantigens or viral
infections, including EBV, are thought to be responsible for the
correlation between malignancy and DM (8,9).
Common malignancies identified in individuals with DM include
adenocarcinoma of the ovary, lung or gastrointestinal tract in
western countries and nasopharyngeal non-keratinizing carcinoma in
South Asia and China. Individuals with these correlations commonly
present with skin lesions and muscle weakness. Patients presenting
with DM and a malignancy are not sensitive to glucocorticoid,
however, the symptoms of DM would be alleviated accompanied by
remission of the tumor after antitumor therapy in the majority of
patients (10). The current patient
exhibited two primary synchronous tumours and did not respond to
chemotherapy or corticosteroids, indicative of a more complex
disorder involving the immune system and poor prognosis.
References
|
1
|
Bohan A and Peter JB: Polymyositis and
dermatomyositis (first of two parts). N Engl J Med. 292:344–347.
1975. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kaneko S and Yamaguchi N: Epidemiological
analysis of site relationships of synchronous and metachronous
multiple primary cancers in the National Cancer Center, Japan,
1962–1996. Jpn J Clin Oncol. 29:96–105. 1999.PubMed/NCBI
|
|
3
|
Hisada M, Garber JE, Fung CY, Fraumeni JF
Jr and Li FP: Multiple primary cancers in families with Li-Fraumeni
syndrome. J Natl Cancer Inst. 90:606–611. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wynder EL, Mushinski MH and Spivak JC:
Tobacco and alcohol consumption in relation to the development of
multiple primary cancers. Cancer. 40:1872–1878. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Young LS and Murray PG: Epstein-Barr virus
and oncogenesis: from latent genes to tumours. Oncogene.
22:5108–5121. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang CC, Chen ML, Hsu KH, et al: Second
malignant tumors in patients with nasopharyngeal carcinoma and
their association with Epstein-Barr virus. Int J Cancer.
87:228–231. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zahr ZA and Baer AN: Malignancy in
myositis. Curr Rheumatol Rep. 13:208–215. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Casciola-Rosen L, Nagaraju K, Plotz P, et
al: Enhanced autoantigen expression in regenerating muscle cells in
idiopathic inflammatory myopathy. J Exp Med. 201:591–601. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chen DY, Chen YM, Lan JL, et al:
Polymyositis/dermatomyositis and nasopharyngeal carcinoma: the
Epstein-Barr virus connection? J Clin Virol. 49:290–295. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pectasides D, Koumpou M, Gaglia A, et al:
Dermatomyositis associated with breast cancer. Anticancer Res.
26:2329–2331. 2006.PubMed/NCBI
|