Introduction
Prostatic small cell neuroendocrine carcinoma
(PSCNC) is an extremely rare type of prostate cancer that accounts
for 0.5–2% of prostatic primary tumors (1,2). In
almost all cases, the tumor is detected at an advanced stage since
prostate-specific antigen (PSA) is unreliable for detecting PSCNC.
The present case was detected during androgen-ablation therapy, at
which point the patient exhibited local symptoms of ischuria and
gross hematuria, as well as a slightly increased PSA value. The
usual treatment for PSCNC is systemic chemotherapy, with or without
radiotherapy, involving a similar regimen to that used for
pulmonary small cell carcinoma (PSCC). In the present case,
following the androgen-ablation therapy, only a locally advanced
tumor and right obturator lymph node metastasis remained;
therefore, it was possible to perform external-beam radiotherapy
(EBRT) and intra-arterial chemotherapy. This treatment was
effective against the local tumor and reduced the lower urinary
tract symptoms, such as gross hematuria and ischuria. The
above-mentioned combination therapy maintained the patient’s
quality of life for a relatively long period and contributed to
extending the patient’s survival. Accordingly, this therapy should
be recommended as a treatment option for cases of locally advanced
PSCNC involving lower urinary obstruction.
This study was approved by the Ethics Committee of
Kurume University (Kurume, Fukuoka, Japan). Written informed
consent was obtained from the patient’s family.
Case report
A 75-year-old male Japanese patient was admitted to
hospital with a high PSA value (95 ng/ml) and right leg edema.
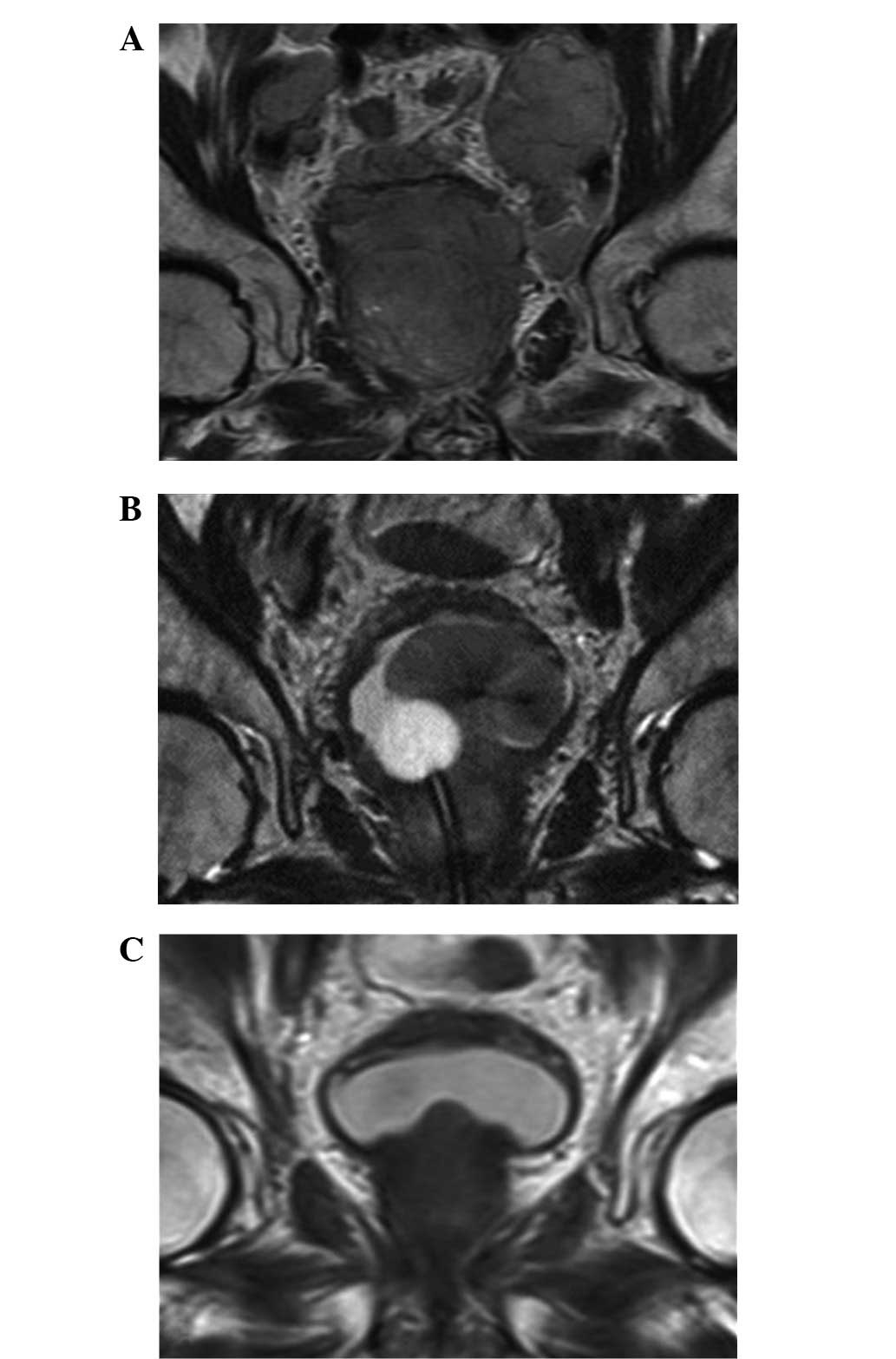
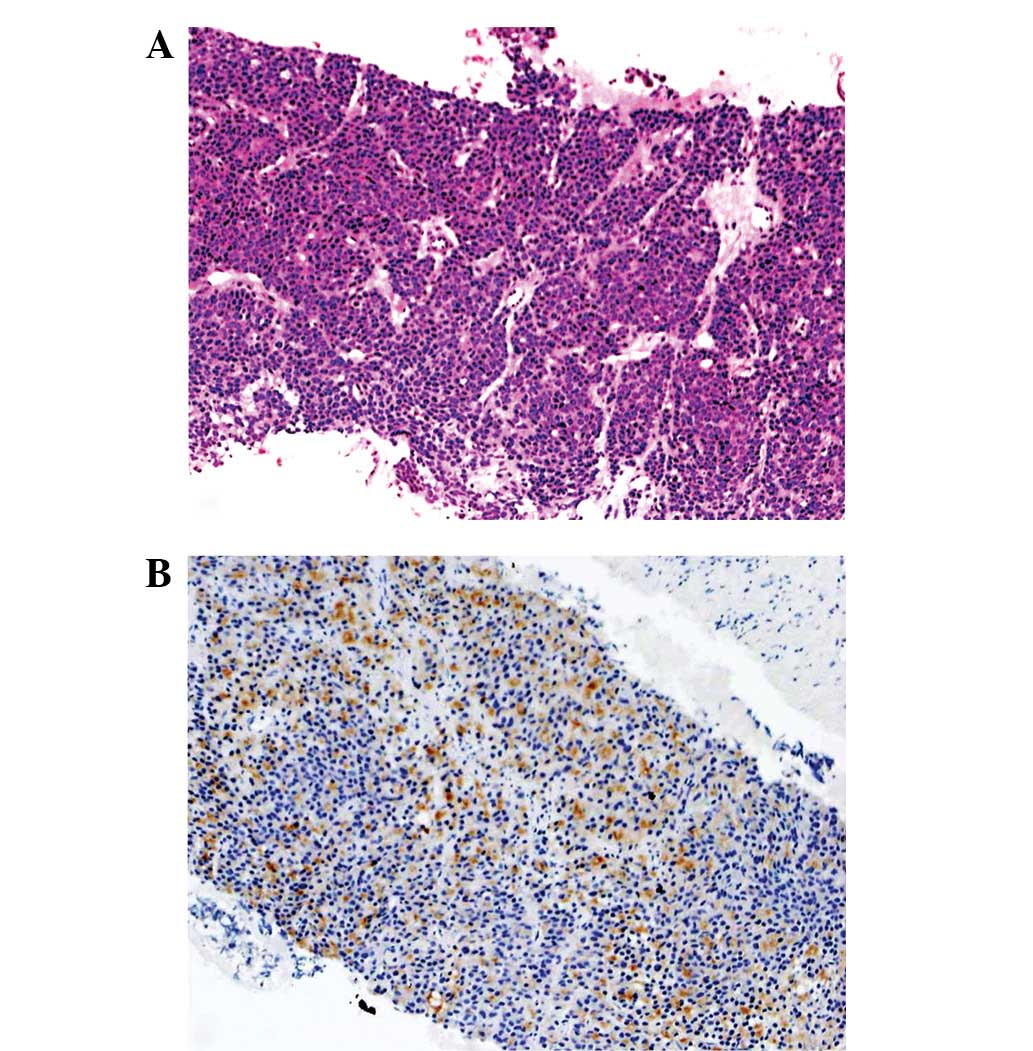
Abdominal ultrasonography, transrectal ultra-sonography, computed
tomography (CT), magnetic resonance imaging (MRI; Fig. 1A) and transrectal biopsy (Fig. 2A) were performed. The patient was
diagnosed with prostate cancer (poorly differentiated
adenocarcinoma, Gleason score: 5+5=10, T4N1M1a stage D2) and
received androgen-ablation therapy involving goserelin acetate
(10.8 mg/3 months) and bicalutamide (80 mg/day) in October 2005.
Subsequently, the patient’s PSA value fell, reaching 0.032 ng/ml in
February 2007. However, the patient gradually became aware of
dysuria and gross hematuria and his PSA value gradually began to
rise again. Eventually, the patient developed ischuria so a
urethral catheter was inserted to relieve the lower urinary
obstruction in September 2007. In October 2007, MRI (Fig. 1B) detected a large tumor extending
from the prostate to the bladder and the patient’s PSA value was
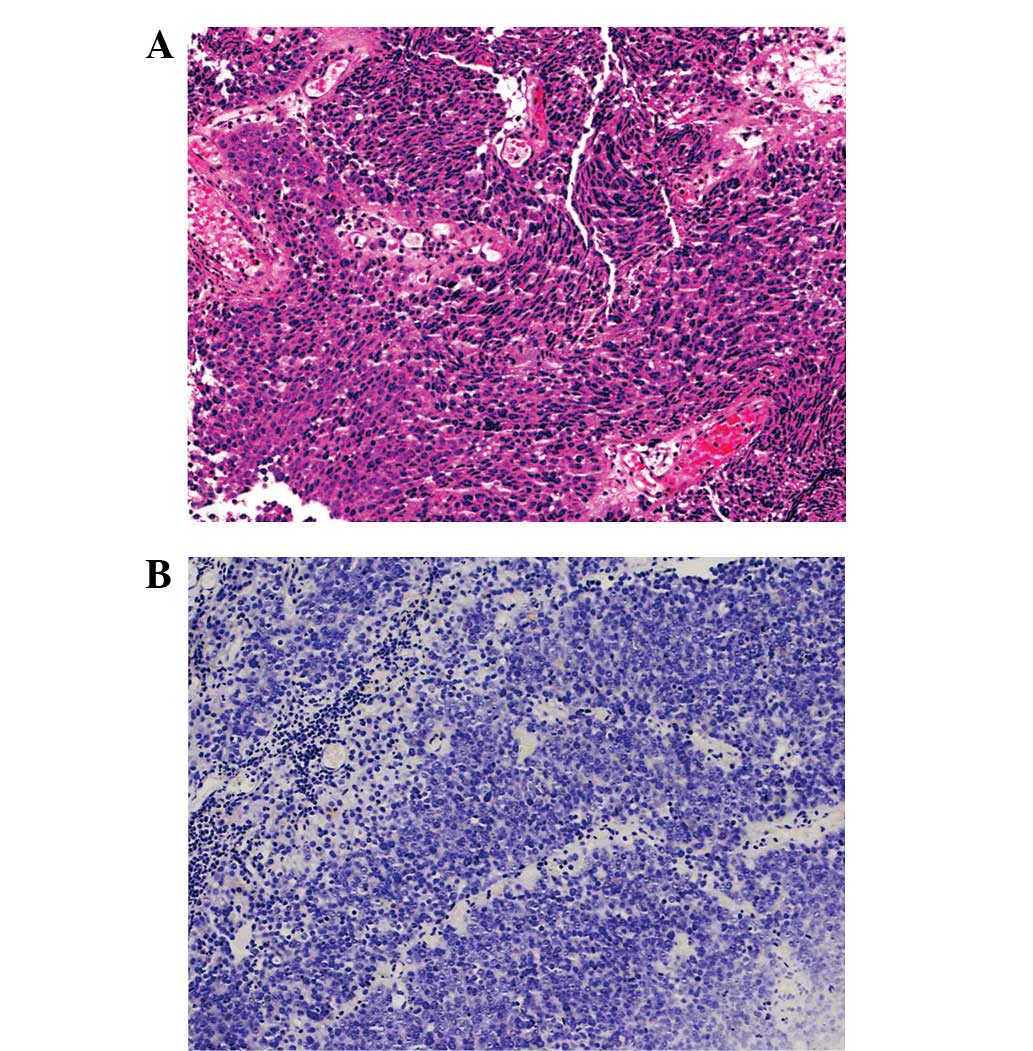
0.151 ng/ml at that time. A transurethral biopsy was performed
(Fig. 3A) and the patient was
diagnosed with PSCNC that occurred following the androgen-ablation
therapy. An immunohistochemical examination of the biopsy tissue
revealed that the tumor cells were negative for PSA (Fig. 3B), neuron-specific enolase (NSE),
chromogranin A and CD56, but positive for synaptophysin.
Subsequently, an additional immunohistochemical examination of the
transrectal biopsy tissue was performed, which identified carcinoma
cells showing the same results as the transurethral biopsy tissue
cells with the exception of PSA, which revealed the intermingling
of PSA positive and negative cells (Fig. 2B). The immuno histochemical findings
are presented in Table I.
Chest-to-pelvis CT scanning detected a large prostatic tumor and a
right obturator lymph node (LN) swelling of 2.5 cm, while bone
scintigraphy did not detect any abnormal lesions. Consequently, the
patient was diagnosed with prostate cancer and the local occurrence
of PSCNC during androgen-ablation therapy for advanced mixed-type
PSCNC.
 | Table IDetails of immunohistochemical
findings. |
Table I
Details of immunohistochemical
findings.
| Markers | Before
androgen-ablation | Subsequent to
androgen-ablation |
|---|
| PSA | +/− | − |
| CgA | − | − |
| NSE | − | − |
| Syn | + | + |
| CD56 | − | − |
The decision was made to administer EBRT and an
intra-arterial infusion of cisplatin (CDDP; 20 mg/m2;
Days 1–5) and ifosfamide (IFM; 1.2 mg/m2; Days 1–3) as
treatments for the local tumor and ischuria (regimen cycle, 21
days). An indwelling catheter was placed in the bilateral internal
iliac artery and a pump was placed in a subcutaneous pocket in
November 2007. At that time, the patient’s serum PSA level was
0.144 ng/ml.
From December 2007, the patient received 3 courses
of intra-arterial chemotherapy and also underwent EBRT of the whole
pelvic cavity and the local tumor with the swollen lymph node at a
total dose of 67 Gy. In the present case, no serious side-effects
that posed a risk to the continuation of the intra-arterial
infusion chemotherapy were observed. The tumor volume was reduced
in MRI (Fig. 1C) and therefore, the
urethral catheter was removed in April 2008 and the patient had no
urinary symptoms. The patient’s PSA value had decreased to 0.015
ng/ml by June 2008.
However, the patient’s PSA value gradually increased
and bone and LN metastasis occurred, although radiographically, the
volume of the local mass remained stable. The patient succumbed in
August 2011 at 70 months after the start of the androgen-ablation
therapy. At the time of the patient’s mortality, he had not
required a urethral catheter for 40 months, although he lost
uresiesthesia due to the wide-ranging spinal bone metastasis and
developed incontinence. No autopsy was performed since we were
unable to obtain the approval of the patient’s family.
Discussion
Extra-pulmonary small cell carcinoma (EPSCC)
accounts for ∼0.1% of all cancers (3) and only 2.5–5% of small cell carcinomas
occur outside of the lungs (4,5). De
novo prostate cancer involving small cell carcinoma is
extremely rare in patients that are diagnosed by biopsy, with an
incidence of 0.5–2% (1,2). However, in a report examining auto
psied prostatic cancer cases, small cell carcinoma showed an
incidence of 10–20% (6). In
addition, Haider et al(3)
reported that the prostate and neck of the uterus were the two most
common organs from which EPSCC originates and that the two most
commonly affected sites were the gastrointestinal tract and the
genitourinary tract. From a review of the literature, there appear
to be three patterns of PSCNC; 35.4% of cases exhibited pure small
cell neuroendocrine (NE) carcinoma, 17.7% of cases involved mixed
adenocarcinoma and 46.9% of cases demonstrated recurrence involving
small cell NE carcinoma that had differentiated from conventional
adenocarcinoma during androgen-ablation therapy (7,8). Thus,
we named these types pure-type PSCNC, mixed-type PSCNC and
differentiated-type PSCNC, respectively.
The prognosis of PSCNC is extremely poor (9). With regard to the prognosis of primary
PSCNC, Deorah et al(10)
reported that the median survival periods for patients with the
local/regional disease (a primary tumor and regional lymph node
metastasis only) and metastatic disease were 15 and 7 months,
respectively, and the 12, 24, 36, 48 and 60-month survival rates
were 47.9, 27.5, 19, 17 and 14.3%, respectively. Furthermore, mixed
adenocarcinoma-type patients live 3–5 months longer than patients
with pure small cell carcinoma (7,8).
Several reports have examined the predictors of a
poor prognosis in mixed-type PSCNC. It was reported that the
presence of the mixed-type adenocarcinoma was predictive of the
degree of metastatic disease and a total lack of hormone
responsiveness (11). Deorah et
al(10) reported that
concomitant well-to-moderately differentiated adeno carcinomas were
associated with an improved prognosis in small cell carcinoma of
the prostate.
With regard to the histological findings of PSCNC,
it is important to note that PSCNC cells exhibit a similar
morphology to PSCC and Gleason pattern 5b prostate adenocarcinoma
cells. Consequently, small cell NE carcinoma is often mistaken for
Gleason pattern 5b adenocarcinoma, as occurred in the present case
(12).
Immunohistochemical staining is often used to detect
PSA, NSE, ProGRP, synaptophysin and chromogranin A in PSCNC,
although other markers have also been reported to be effective. Yao
et al(12) reported that
PSCNC exhibits a positive PSA percentage of 17% and suggested that
PSA, thyroid transcription factor-1 (TTF-1) and CD56 were useful
for distinguishing PSCNC from Gleason pattern 5b adenocarcinoma.
The authors also reported that numerous PSCNC cells were positive
for bombesin/GRP, c-kit, bcl-2 and EGFR. The majority (80%) of
small cell carcinoma cells were positive for at least one
neuroendocrine marker. However, negative immunostaining for these
markers does not exclude small cell carcinoma.
The most curative treatment for PSCNC is radical
prosta tectomy, although it is only indicated for early stage and
limited tumors (1). However, PSCNC
is an extemely aggressive disease and the majority of cases exhibit
metastatic lesions and a large mass at diagnosis. Thus, there is no
established treatment for PSCNC. With regard to the treatment for
PSCC, the most effective method for limited PSCC is
chemoradiotherapy using systemic chemotherapy involving CDDP and
etoposide in combination with EBRT involving a total dose of 45 Gy
and the most effective method for extensive-stage PSCC is four to
six cycles of systemic chemotherapy of CDDP and etoposide
(non-Asian patients) or CDDP and irinotecan (Asian patients).
Moreover, additional thorax radiotherapy has improved the prognosis
of advanced PSCC in which extensive-stage non-thorax cases achieved
CR and those with intra-thorax disease achieved PR following three
courses with the systemic chemotherapy of CDDP and etoposide
(13). Accordingly, in the majority
of cases, advanced PSCNC is treated with systemic chemotherapy
involving the CDDP/etoposide regimen with or without EBRT as well
as PSCC. In the present case, intra-arterial chemotherapy was
selected in order to increase the efficacy of the treatment against
the local lesion and reduce the frequency/grade of the side-effects
(14). The CDDP/IFM regimen was
selected and considered to be an appropriate choice as it was an
effective carcinostatic and was the most suitable treatment option
of those that were available for prostate cancer under the Japanese
national healthcare insurance scheme at the time of the patient’s
treatment (14). With regard to
prophylactic cranial irradiation (PCI), EPSCC is not usually
indicated for PCI since the frequency of brain metastasis in EPSCC
is lower than that in PSCC (15). A
small number of reports have revealed that PSCNC is not suitable
for routine PCI (16), although
another report observed that the incidence of brain metastasis from
PSCNC was ∼10% (11). Vashchenko
and Abrahamsson (17) reported
several new useful treatment agents for NE differentiation in
prostate cancer, including somatostatin analogs, serotonin
antagonists, bombesin antagonists and inflammatory cytokines, such
as interleukin-6. These new agents are expected to prolong the
survival of PSCNC patients. The relaxin (RLN) receptor RXFP1 is
also a potential target for PSCNC treatments. Feng et
al(18) reported that the
suppression of RLN/RXFP1 produced a significant reduction in tumor
volume, which was associated with decreased cell proliferation and
increased apoptosis in PC3 prostate cancer cell lines (the group to
which small cell NE carcinoma belongs).
PSCNC is sensitive to chemoradiotherapy, which is
able to achieve local control and prolong survival, similar to its
effects in PSCC. This suggests that combined therapy involving
androgen-ablation therapy and chemoradiotherapy is beneficial for
advanced mixed-type PSCNC. In addition, we suggest that the
prognostic factors for advanced mixed-type PSCNC are as follows:
the sensitivity of the conventional adenocarcinoma to
androgen-ablation therapy, degree of metastasis (the number of
metastatic organs and the size of any masses) and extent of the
small cell NE carcinoma component.
References
|
1
|
Palmgren JS, Karavadia SS and Wakefield
MR: Unusual and underappreciated: small cell carcinoma of the
prostate. Semin Oncol. 34:22–29. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yao JL, Huang J and di Sant’Agnese PA:
Small cell carcinoma of the prostate. Diagn Histopathol.
14:117–121. 2008. View Article : Google Scholar
|
|
3
|
Haider K, Shahid RK, Finch D, et al: Extra
pulmonary small cell carcinoma: a Canadian province’s experience.
Cancer. 107:2262–2269. 2006.
|
|
4
|
Levenson RM Jr, Ihde DC, Matthews MJ,
Cohen MH, Gazdar AF, Bunn PA Jr and Minna JD: Small cell carcinoma
presenting as an extrapulmonary neoplasm: sites of origin and
response to chemotherapy. J Natl Cancer Inst. 67:607–612.
1981.PubMed/NCBI
|
|
5
|
Remic SC and Ruckdeschel JC:
Extrapulmonary and pulmonary small-cell carcinoma: tumor biology,
therapy, and outcome. Med Pediatr Oncol. 20:89–99. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tanaka M, Suzuki Y, Takaoka K, Suzuki N,
Murakami S, Matsuzaki O and Shimazaki J: Progression of prostate
cancer to neuroendocrine cell tumor. Int J Urol. 8:431–436. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Oesterling JE, Hauzeur CG and Farrow GM:
Small cell anaplastic carcinoma of the prostate: a clinical,
pathological and immunohistological study of 27 patients. J Urol.
147:804–807. 1992.PubMed/NCBI
|
|
8
|
Papandreou CN, Daliani DD, Thall PF, et
al: Result of a phase II study with doxorubicin, etoposide, and
cisplatin in patients with fully characterized small-cell carcinoma
of the prostate. J Clin Oncol. 20:3072–3080. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Di Sant’Agnese PA and Cockett AT: The
prostatic endocrine-paracrine (neuroendocrine) regulatory system
and neuroendocrine differentiation in prostatic carcinoma: a review
and future directions in basic research. J Urol. 152:1927–1931.
1994.
|
|
10
|
Deorah S, Rao MB, Raman R, Gaitonde K and
Donovan JF: Survival of patients with small cell carcinoma of the
prostate during 1973–2003: a population-based study. BJU Int.
109:824–830. 2012.
|
|
11
|
Spiess PE, Pettaway CA, Vakar-Lopez F, et
al: Treatment outcomes of small cell carcinoma of the prostate: a
single-center study. Cancer. 110:1729–1737. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yao JL, Mardeb R and Bourne P: Small cell
carcinoma of the prostate: an immunohistochemical study. Am J Surg
Pathol. 30:705–712. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
van Meerbeeck JP, Fennell DA and De
Ruysscher DK: Small-cell lung cancer. Lancet. 378:1741–1755.
2011.
|
|
14
|
Uemura K, Nishihara K, Hayashi T, Tomiyasu
K and Matsuoka K: Improvement in urinary retention due to recurrent
anastomotic prostate cancer treated with various therapies by
intra-arterial infusion of cisplatin and ifosfamide. J Infect
Chemother. 18:753–755. 2012. View Article : Google Scholar
|
|
15
|
Früh M, Kacsir B, Ess S, Cerny T,
Rodriguez R and Plassnilm L: Extrapulmonary small cell carcinoma:
an indication for prophylactic cranial irradiation? A single center
experience. Strahlenther Onkol. 187:561–567. 2011.PubMed/NCBI
|
|
16
|
Walenkamp AM, Sonke GS and Sleijfer DT:
Clinical and therapeutic aspects of extrapulmonary small cell
carcinoma. Cancer Treat Rev. 35:228–236. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Vashchenko N and Abrahamsson PA:
Neuroendocrine differentiation in prostate cancer: implications for
new treatment modalities. Eur Urol. 47:147–155. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Feng S, Agoulnik IU, Truong A, et al:
Suppression of relaxin receptor RXFP1 decreases prostate cancer
growth and metastasis. Endocr Relat Cancer. 17:1021–1033. 2010.
View Article : Google Scholar : PubMed/NCBI
|