Introduction
In the present study, we report a case of tumor
lysis syndrome (TLS) in a patient with gallbladder carcinoma
treated with gemcitabine and cisplatin. TLS occurs most commonly in
highly proliferative hematological malignancies such as acute
lymphoblastic leukemia, acute myeloid leukemia and Burkitt’s
lymphoma (1). It also occurs in
certain solid tumors, notoriously small cell carcinoma, and rarely
in other types of tumor (2).
Although TLS has been reported in hepatocellular carcinoma
(2,3), to the best of our knowledge, this is
the first reported case of TLS associated with gallbladder
carcinoma.
TLS occurs when malignant cells lyse and release
their contents, usually within 12–72 h of cytotoxic therapy
(2,4,5).
Release of intracellular contents leads to hyperuricemia,
hyperphosphatemia, hypocalcemia and hyperkalemia. Laboratory TLS
parameters have been suggested by Cairo and Bishop and include uric
acid ≥8 mg/dl, potassium ≥6 mg/l, phosphorus ≥2.1 mmol/l (children)
or ≥1.45 mmol/l (adults), and calcium ≤1.75 mmol/l, or a 25% change
from baseline in any of these parameters (6). TLS is potentially fatal, possibly
leading to renal failure or fatal arrhythmias (1).
Prevention is considered to be the best management
and consists of aggressive intravenous fluids, allopurinol and
rasburicase prophylaxis in high-risk patients (1). Although urine alkalanization has
previously been used as treatment, it is no longer recommended by
some groups as a viable treatment option (1). Instead, prevention treatment using
these agents is now recommended.
It has been suggested that the incidence of TLS in
solid tumors is low (5), but it may
be underestimated. A literature review found 45 reported cases,
with a mortality rate of approximately 1 in 3 (2). In the present study, we demonstrate
that even in the case of certain solid tumors, attention should be
given to the possibility of a patient developing TLS.
The case report was approved by the Institutional
Review Board at the University of Missouri.
Case report
A 50-year-old male presented with abdominal pain.
Laboratory tests showed mild leukocytosis (11,500/mcl) and anemia
(11.7 g/dl). The patient had an elevated alkaline phosphotase of
152 U/l with otherwise normal liver function.
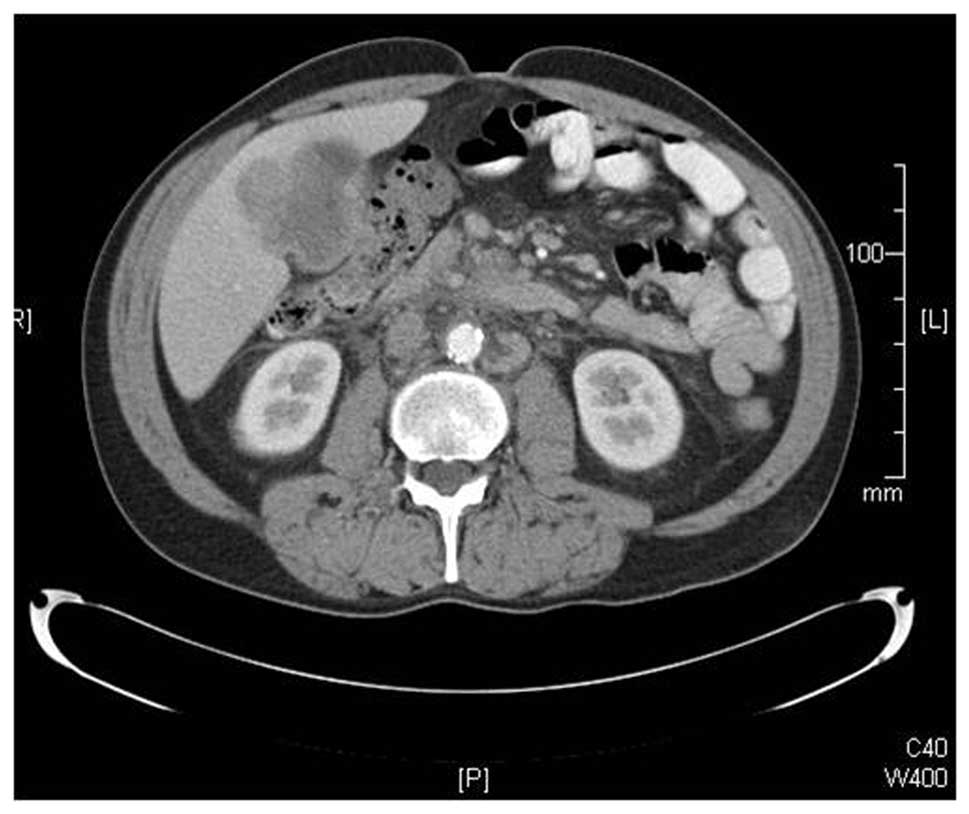
A computed tomography scan of the abdomen (Fig. 1) revealed a heterogeneous mass of
the gallbladder fossa measuring 5×5×6 cm. There was also
lymphadenopathy of periportal, pericaval, periaortic and mesenteric
lymph nodes.
The gallbladder tumor was resected, but a curative
resection was impossible due to massive lymphadenopathy of aortic,
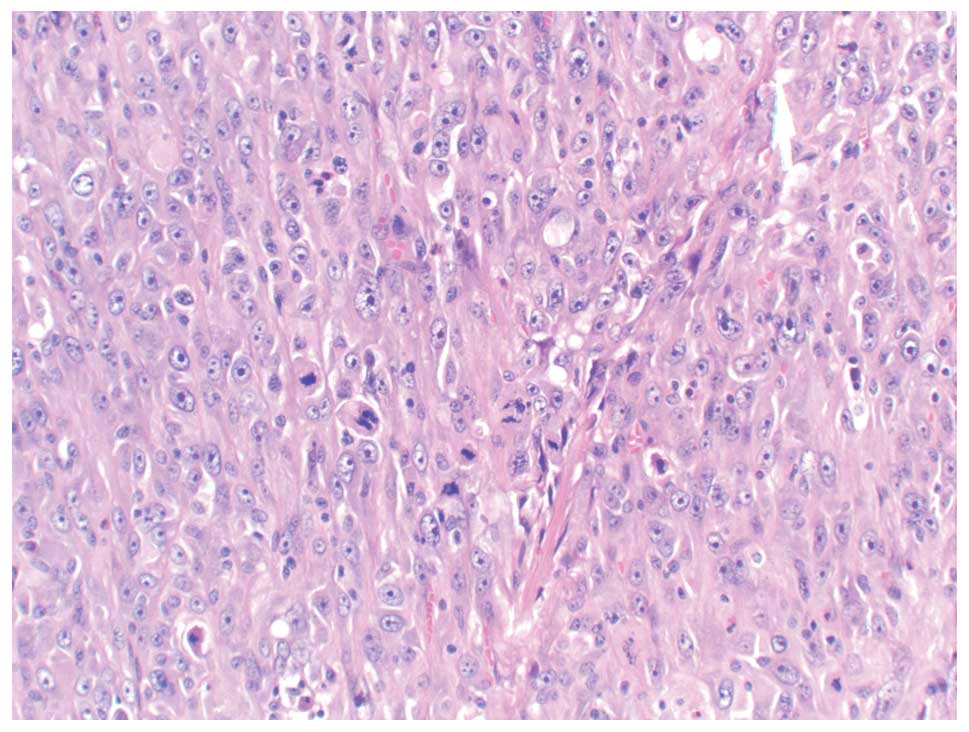
vena cava, and celiac areas. Final pathology revealed a 7-cm poorly
differentiated adenocarcinoma with sarcomatoid features (Fig. 2). The tumor was found to have areas
of brisk atypical mitoses. Lymph nodes showed metastatic
adenocarcinoma.
The patient was diagnosed with a stage IV poorly
differentiated adenocarcinoma of the gallbladder, AJCC stage IVB
(T3 N2 MX0). The recommendation was a chemotherapy regimen of
gemcitabine and cisplatin. Chemotherapy did not commence
immediately due to poor performance status.
Approximately 2 weeks after this visit, the patient
presented with shortness of breath and an inability to eat or
drink. Laboratory test results on that day included a white blood
cell count of 19,900/mcl, laboratory evidence of dehydration, total
bilirubin of 3.4 mg/dl, alkaline phosphatase of 1652 U/l, AST 109
U/l, and ALT 40 U/l, a picture consistent with cholestasis. Due to
tense ascites, paracentesis was performed. However, the patient
also had elevated cardiac enzymes with possible ST elevations and Q
waves. A cardiac catheterization showed single-vessel coronary
artery disease, and medical therapy was recommended.
When his cardiac status had stabilized, a lengthy
discussion was held with the patient. The decision was made to
proceed with chemotherapy. The patient was administered one dose
each of gemicitabine and cisplatin. On the second day after
chemotherapy, the patient was dyspneic with air hunger. Urine
output decreased to 300 ml over 24 h, even with high doses of IV
lasix.
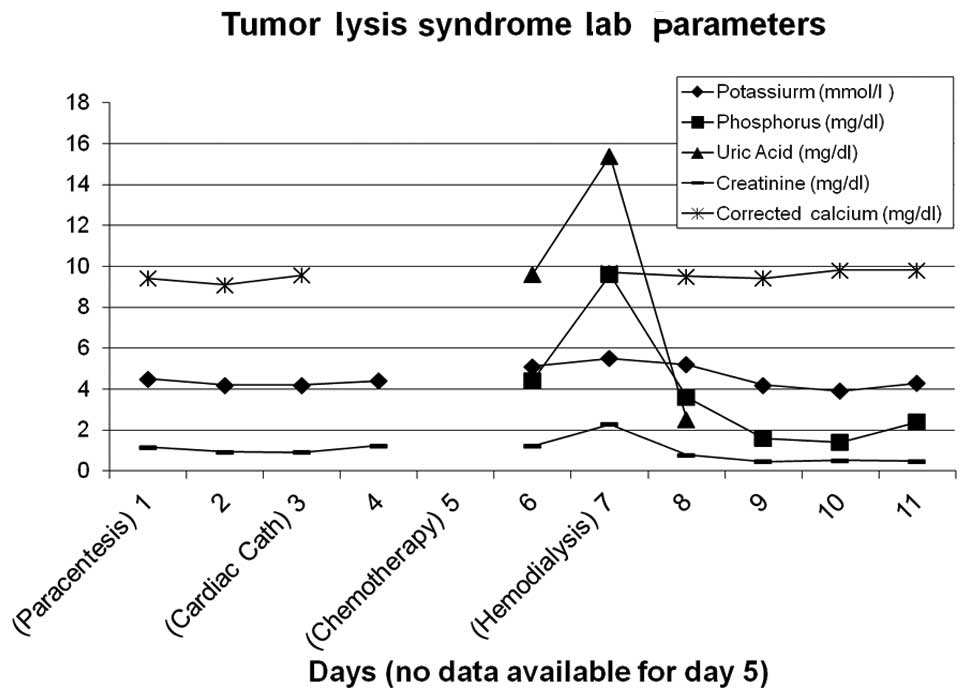
A diagnosis of tumor lysis syndrome was evident
(Fig. 3). Laboratory results showed
hyperkalemia (6.0 mmol/l), hyperphosphatemia (9.6 mg/dl), elevated
uric acid (15.4 mg/dl) and evidence of acute renal failure with a
creatinine of 2.69 mg/dl (previously normal). Corrected calcium was
normal at 9.7 mg/dl, although ionized calcium was slightly reduced
to a low of 1.06 mmol/l. The patient was treated with dialysis. His
calcium-phosphorus product was 93 on the first day of dialysis,
likely contributing to acute renal failure via nephrocalcinosis.
His clinical picture was complicated by urosepsis, bilateral deep
vein thrombosis and a possible pulmonary embolism. The patient
succumbed 6 days after beginning chemotherapy to the disease.
Discussion
This is the first reported case of TLS developing in
a patient with gallbladder carcinoma. There are at least two
clinical factors that make this case unique and, in retrospect,
increased the patient’s risk of TLS.
First, the patient had multi-factorial mild acute
renal failure. He had mild contrast-induced nephropathy following
cardiac catheterization, with creatinine increasing from a baseline
of approximately 0.9 to 1.24 mg/dl the day after catheterization.
It was also thought that volume depletion associated with
paracentesis performed two days prior to the cardiac
catheterization contributed to acute renal failure. These factors
may have altered the patient’s renal function just enough to create
a physiological condition favorable to the development of TLS.
Pretreatment renal impairment is a reported risk factor for TLS in
solid tumors, along with increased LDH and hyperuricemia (1,2).
Second, the tumor in this case was described as a
poorly differentiated sarcomatoid type of adenocarcinoma. Brisk
atypical mitoses were noted, indicating a highly proliferative
tumor. This type of solid tumor may increase the risk of TLS
compared to one that is slow-growing (fewer mitoses) and
well-differentiated.
This raises the question of whether TLS prophylaxis
such as allopurinol or rasburicase, urine alkalinization and
intense hydration should be considered in certain types of solid
tumors and/or in clinical situations such as in patients with mild
acute nephropathy. Known risk factors for TLS include highly
proliferative tumors (1,5), treatment-sensitive tumors, heavy tumor
burden, and dehydration and/or renal disease (3). A recent expert TLS panel determined
that the majority of solid tumors are in the low-risk category
(4), but each clinical situation
should be considered separately. TLS risk is particularly affected
by renal function, and patients with low-risk tumors are moved into
an intermediate risk category when renal dysfunction is present
(4). It has been suggested that
improvements in the treatment of some solid tumors, which were
previously considered relatively insensitive to chemotherapy, have
now rendered them more sensitive, thus placing these patients at a
greater risk for TLS. As the mortality rate of patients with TLS in
solid tumors may be higher than in patients with hematological
malignancies (5), this renders
prevention of TLS in certain solid tumors a clinical necessity
(2,3).
References
|
1
|
Coiffier B, Altman A, Pui CH, Younes A and
Cairo MS: Guidelines for the management of pediatric and adult
tumor lysis syndrome: an evidence based review. J Clin Oncol.
26:2767–2778. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Baeksgaard L and Sorensen JB: Acute tumor
lysis syndrome in solid tumors – a case report and review of the
literature. Cancer Chemother Pharmacol. 51:187–192. 2003.
|
|
3
|
Huang WS and Yang CH: Sorafenib induced
tumor lysis syndrome in an advanced hepatocellular carcinoma
patient. World J Gastroenterol. 15:4464–4466. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cairo MS, Coiffier B, Reiter A and Younes
A: Recommendations for the evaluation of risk and prophylaxis of
tumour lysis syndrome (TLS) in adults and children with malignant
diseases: an expert TLS panel consensus. British J Haem.
149:578–586. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mughal TI, Ejaz AA, Foringer JR and
Coiffier B: An integrated clinical approach for the identification,
prevention, and treatment of tumor lysis syndrome. Cancer Treat
Rev. 36:164–176. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cairo MS and Bishop M: Tumour lysis
syndrome: New therapeutic strategies and classification. Br J
Haematol. 127:3–11. 2004. View Article : Google Scholar : PubMed/NCBI
|