Introduction
Malignant lymphoma of the mucosa-associated lymphoid
tissue (MALT) was first reported in 1983. The disease commonly
occurs in the stomach and lungs, but rarely in the urinary tract.
As MALT lymphoma is one of the less aggressive lymphomas and tends
to remain localized with slow progression for a long period, it
often produces no subjective symptoms and is incidentally detected
in radiological imaging studies. It is occasionally difficult to
differentiate MALT lymphoma from urothelial carcinoma using imaging
studies when the disease presents with upper urinary obstruction
due to renal pelvic or ureteral involvement. In the present study,
we report a unique case of MALT lymphoma in which the lymphoma
cells appear to diffusely infiltrate the whole upper urinary tract.
Written informed consent was obtained from the patient.
Case report
A 69-year-old male with a history of hypertension
and diabetes mellitus was referred to the National Defense Medical
College hospital, Tokorozawa, Japan as an abdominal computed
tomography (CT) scan had incidentally revealed a left
hydronephrosis and abnormal structure surrounding the left renal
pelvis.
There were no remarkable findings in the physical
examination, while the laboratory tests yielded a white blood cell
count of 5.7×109/l (neutrophilic leukocytes, 54.9%), a
hemoglobin level of 15.3 g/dl, a platelet count of
247×109/l and a serum creatinine level of 0.92 mg/dl.
The patient was free from systemic inflammation; the erythrocyte
sedimentation rate (ESR) was 8 mm in the first hour and the
C-reactive protein level was <0.3 mg/dl. The urinalysis was
normal and the urine cytology indicated no atypical cells.
Enhanced CT and magnetic resonance imaging (MRI)
scans showed a mild left hydronephrosis and a diffuse renal pelvic
wall thickening that was enhanced slightly by contrast media
(Fig. 1A–C). A left retrograde
pyelography revealed a 3-cm long narrowing of the upper ureter and
the surface of the ureteral lumen was smooth (Fig. 1D). Brush cytology of the stenotic
area revealed atypical cells. Although malignant lymphoma was
initially suspected due to the radiological findings,
67gallium scintigraphy showed only weak uptake in the
left renal pelvis and the CT scan showed no lymph node swelling in
the para-aortic area. The serum IL-2 receptor level was slightly
elevated (524 U/ml).
The atypical cells identified by brush cytology, and
the diffuse thickening of the renal pelvic and ureteral wall
detected by imaging studies, led us to suspect invasive urothelial
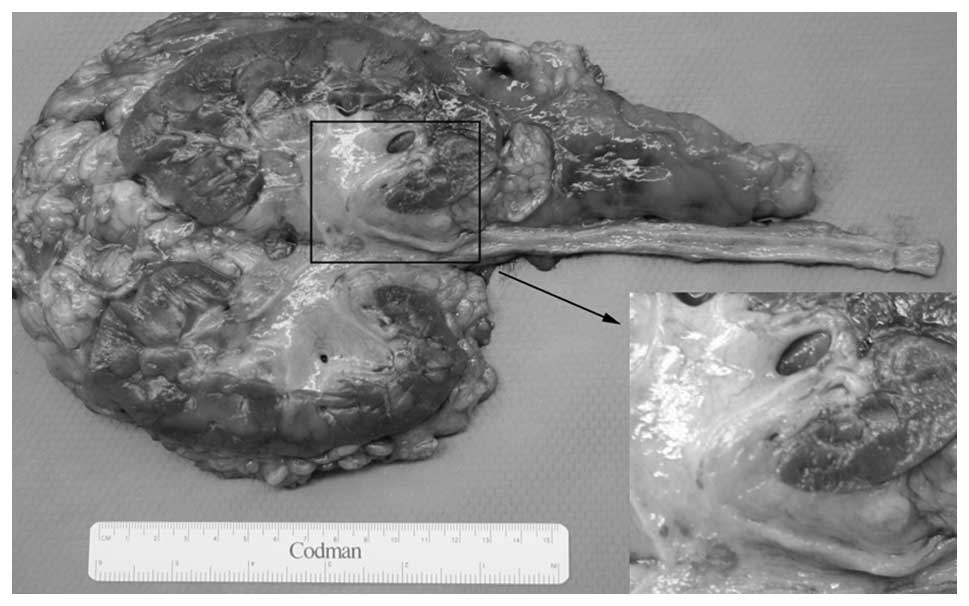
cancer. Therefore, a left nephroureterectomy with bladder-cuff
excision was performed. En bloc excision of the left kidney, ureter
and para-aortic lymph nodes was conducted, as the malignant lesion
was presumed to exist around the renal pelvis and ureter (Fig. 2). Marked adhesion of the left ureter
was observed around the common iliac artery, and abnormal fibrotic
tissue around the ureter was also resected during the
nephroureterectomy.
Histological examination showed an intense lymphoid
infiltrate consisting of mainly B cells. There were areas in which
plasma cells and small centrocyte-like lymphocytes formed distinct
lymphoid follicles, therefore, extranodal marginal zone B cell
MALT-type lymphoma, follicular lymphoma or mantle cell lymphoma
were suspected (Fig. 3). The
immunohistochemical analysis demonstrated that the lesion was
positive for CD20 and CD79a and negative for CD5 and cyclin D1.
These observations led to the diagnosis of MALT lymphoma. Lymphoma
cells occupying the submucosa of the renal pelvis and upper ureter
spread into the surrounding area and extended to the level of the
distal ureter, where the abnormal tissue was macroscopically
unremarkable. Furthermore, lymphoma cells were identified at the
distal edge of the excised ureter. As a focal infiltration of
lymphocytes and plasma cells was observed in the specimen obtained
from around the common iliac artery, the presence of residual MALT
lymphoma in situ was inferred. The patient was referred to
the department of hematology, where he underwent eight courses of
rituximab. Since the surgery, the patient has survived for 78
months without a relapse of lymphoma.
Discussion
MALT lymphoma, first described by Isaacson et
al in 1983 (1), accounts for 8%
of all malignant lymphomas. The disease may occur in various sites,
most commonly in the gastrointestinal tract, lungs, salivary
glands, orbits, skin and thyroid, but the urinary tract is rarely
involved. Low-grade MALT lymphomas often have an indolent clinical
course, and the onset of MALT is usually preceded by an
inflammatory process. For example, Helicobacter pylori
gastritis typically precedes MALT lymphoma of the stomach, lymphoid
interstitial pneumonia may precede MALT lymphoma of the lungs,
Sjögren syndrome may precede MALT lymphoma of the salivary glands
and Hashimoto’s thyroiditis may precede MALT lymphoma of the
thyroid. The pathogenesis of MALT lymphoma in the present case is
unknown as the patient had no history of urinary tract inflammation
and no inflammatory cells in the urine.
To the best of our knowledge, only seven cases of
MALT lymphoma affecting the upper urinary tract have been reported
previously. Table I summarizes the
clinicopathological findings of these cases and those of the
present case (2–7). MALT lymphoma of the upper urinary
tract is dominant in males (87.5%). The patient age ranged from 30
to 83 years (median, 65 years). Only three patients complained of
back or abdominal pain, and the remaining five patients were
asymptomatic. Two patients also had cancerous tissue in either the
orbits or the salivary and prostate glands. Two of these eight were
diagnosed by needle biopsy, and in the case of the remaining six
patients, the diagnosis was made after nephrectomy or
nephroureterectomy. No cancer-related mortality was reported in
these cases, suggesting that patients with MALT lymphoma of the
upper urinary tract have a favorable prognosis.
 | Table ISummary of MALT lymphoma affecting the
upper urinary tract. |
Table I
Summary of MALT lymphoma affecting the
upper urinary tract.
| Case | Site | Age (years) | Gender | Chief complaint | Other sites | Radiological
feature | Other illness | Means of
diagnosis | Additional
treatment | Outcome | Ref. |
|---|
| 1 | Bil. renal
pelvis | 68 | M | None | Salivary and
prostate | Mass | Excision of
submandibular glands | Biopsy | None | 13 months, alive | 2 |
| 2 | Rt renal pelvis and
parenchyma | 50 | M | None | | Mass | H.P. gastritis and
HT | Nx | Eradication of
H.P | Alive | 3 |
| 3 | Rt renal pelvis and
parenchyma | 30 | M | Rt. abd. pain and
frequency | | Mass | Nephrotic
syndrome | Nx | None | 28 months, alive | 4 |
| 4 | Lt renal pelvis | 83 | F | Back pain | | Thickening | None | Biopsy | Chemotherapy | 8 months, alive | 5 |
| 5 | Rt renal pelvis | 72 | M | Abd. pain and
fever | Bil. orbit | Mass | Colon AC | Nx | None | Died of pulmonary
embolism | 5 |
| 6 | Rt renal pelvis | 77 | M | None | | Thickening | Gastric AC | Nux | None | 10 months, alive | 6 |
| 7 | Rt upper ureter | 72 | M | None | | Thickening | DM | Nux | None | 9 months, alive | 7 |
| 8 | Lt renal pelvis and
upper ureter | 69 | M | None | | Thickening | HT and DM | Nux | Chemotherapy | 78 months, alive | Present case |
Lymphomatous involvement of the ureter was first
reported by Stow in 1909 (8).
Ureteral obstruction is rarely observed at the initial presentation
of malignant lymphoma, and its overall frequency in malignant
lymphoma cases varies from 0.86–8.8% (9–10).
Although the majority of patients with lymphomatous involvement of
the ureter have extrinsic ureteral compression due to enlarged
lymphoma-bearing lymph nodes, upper urinary obstruction due to an
apparent intrinsic renal pelvic or ureteral involvement without
extrinsic nodal enlargement has rarely been reported. Additionally,
diffuse invasion of lymphoma cells into the whole ureter was also
rarely observed. In the reported cases listed in Table I, we identified four cases (50%)
with similar features of wall thickening; each of these cases
presented with a thick urinary tract. Diffuse thickening of the
pyeloureteral wall may therefore be a representative feature of
MALT lymphoma involving the upper urinary tract.
The overall prognosis for MALT lymphoma patients
appears to be good, as MALT lymphoma presents as an indolent and
localized disease and remains confined to the site of origin for a
prolonged period following diagnosis (11). However, transformation to high-grade
lymphoma in the late course of the disease was reported to occur in
8% of MALT lymphoma patients (12).
The disease may be treated with surgery or radiotherapy if it is
localized, but may require treatment by chemotherapy, with or
without irradiation, in cases where it presents with dissemination
or high-grade transformation. In the present case, the observation
of diffuse lymphomatous extension into not only the renal pelvis
but also the whole ureter, and the possibility of residual lymphoma
cells around the ureter, led us to administer rituximab following
surgery.
References
|
1
|
Isaacson P, Wright DH and Jones DB:
Malignant lymphoma of true histiocytic (monocyte/macrophage)
origin. Cancer. 51:80–91. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Araki K, Kubota Y, Iijima Y, et al:
Indolent behaviour of low-grade B-cell lymphoma of
mucosa-associated lymphoid tissue involved in salivary glands,
renal sinus and prostate. Scand J Urol Nephrol. 32:234–236. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Colović M, Hadzi-Djokić J, Cemerikić V, et
al: Primary MALT lymphoma of the kidney. Hematol Cell Ther.
41:229–232. 1999.PubMed/NCBI
|
|
4
|
Kato Y, Hasegawa M, Numasato S, Monma N
and Fujioka T: Primary mucosa-associated lymphoid tissue-type
lymphoma arising in the kidney. Int J Urol. 15:90–92. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Qiu L, Unger PD, Dillon RW and Strauchen
JA: Low-grade mucosa-associated lymphoid tissue lymphoma involving
the kidney: report of 3 cases and review of the literature. Arch
Pathol Lab Med. 130:86–89. 2006.PubMed/NCBI
|
|
6
|
Mita K, Ohnishi Y, Edahiro T, et al:
Primary mucosa-associated lymphoid tissue lymphoma in the renal
pelvis. Urol Int. 69:241–243. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hara M, Satake M, Ogino H, et al: Primary
ureteral mucosa-associated lymphoid tissue (MALT) lymphoma -
pathological and radiological findings. Radiat Med. 20:41–44.
2002.PubMed/NCBI
|
|
8
|
Stow B: Fibrolymphosarcomata of both
ureters metastatic to a primary lymphosarcomata of the anterior
mediastinum of thymus origin. Ann Surg. 50:901–906. 1909.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rosenberg SA, Diamond HD, Jaslowitz B and
Craver LF: Lymphosarcoma: a review of 1269 cases. Medicine
(Baltimore). 40:31–84. 1961. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Abeloff MD and Lenhard RE Jr: Clinical
management of ureteral obstruction secondary to malignant lymphoma.
Johns Hopkins Med J. 134:34–42. 1974.PubMed/NCBI
|
|
11
|
Montalbán C, Castrillo JM, Abraira V, et
al: Gastric B-cell mucosa-associated lymphoid tissue (MALT)
lymphoma. Clinicopathological study and evaluation of the
prognostic factors in 143 patients. Ann Oncol. 6:355–362.
1995.PubMed/NCBI
|
|
12
|
Thieblemont C, Berger F, Dumontet C, et
al: Mucosa-associated lymphoid tissue lymphoma is a disseminated
disease in one third of 158 patients analyzed. Blood. 95:802–806.
2000.PubMed/NCBI
|