Introduction
Soft tissue sarcomas (STSs) are a heterogeneous
group of malignant neoplasias of >50 subtypes of mesenchymal
origin. These tumors represent <1% of all types of cancer and
their classification is based on histological morphology of the
tumors (1). STS incidence is low,
annually affecting ∼200,000 individuals worldwide. However, these
neoplasias are aggressive and the treatment, when possible, is
based on traditional chemotherapies often associated with
resistance. STS cells have been identified to originate from
various cell lines, which explains, in part, the variety of
phenotype characteristics observed in this tumor (1–3).
Metastases in STS patients are frequently identified
at diagnosis and consequently, the correct utilization of treament
parameters during disease managment is important (4). Histological grade, size, depth of
tumor and status of surgical resection are currently used as
prognostic factors for STS. Nevertheless, histological grade is
currently the best criterion to determine tumor aggressiveness
(2). At present, various molecules
associated with the biological behavior of these tumors have been
described for STSs and may improve clinical diagnosis (4).
Ki-67 is a well-known protein located in the nucleus
and nucleolus of cells and is associated with proliferation of
somatic cells. Ki-67 is absent in quiescent cells (5). For this reason, human Ki-67 protein is
an efficient immunohistochemical marker for establishing levels of
malignant cell proliferation and is widely used in the diagnosis of
several types of human tumor, including STSs (6). High expression of Ki-67 protein in
STSs, is frequently associated with poor prognosis (7), including the occurrence of distant
metastases (8).
Cluster of differentiation 100 (CD100) protein is an
additional immunohistochemical marker of various types of tumor.
CD100, also known as Semaphorin 4D (Sema4D), is a homodimeric
glycoprotein markedly expressed in lymphoid tissue, skeletal muscle
and at lower levels in the human brain (9). CD100 has been identified in two forms,
membrane-anchored and soluble. Membrane and soluble forms function
as a receptor with high-affinity to Plexin B1 or a ligand to the
low affinity receptor, CD72, respectively (10,11).
Semaphorins were primarily classified as axon guidance molecules
(12–14). However, this family is also involved
in angiogenesis, organogenesis, apoptosis and neoplasia (15–18),
as well as in human immune responses (19) where CD100 functions as a ligand or
receptor to modulate the activities of B and T lymphocytes. In
addition, CD100 interaction with Plexin B1 induces migration and
tubulogenesis of endothelial cells (20). CD100 is involved in a molecular
pathway with Plexin B1 and Met to promote invasive growth of
malignant epithelial cells (21).
Ch’ng et al(22) previously
reported a correlation between CD100 and poor prognosis in STSs.
Accordingly, CD100 is involved in various mechanisms of tumor
progression, including angiogenesis, invasive growth and regulation
of tumor-associated macrophages (23).
The aim of the present study was to evaluate Ki-67
and CD100 expression in STS patient samples from Barretos Cancer
Hospital (Barretos, Brazil) to determine whether, in the current
population sample, reproducible results of the markers as effective
prognostic factors in STSs are obtained. Results demonstrate that
CD100 is an indicator of poor prognosis in STSs, consistent with
the results of Ch’ng et al(22). Furthermore, Ki-67 expression in
these tumors was identified as an effective prognostic tool capable
of predicting local recurrence. To the best of our knowledge the
current study is the first description of the use of Ki-67 as an
indicator of local recurrence in STSs.
Materials and methods
Patients
Sixty-five patients with STSs were treated at the
Department of Orthopaedic Oncology of Barretos Cancer Hospital
(Barretos, Brazil) between 2000 and 2009. Of these patients, 42
(64.6%) were male and 23 (35.4%) were female. Patients were
predominantly Caucasian (43, 66.2%) and 38 (58.5%) were from São
Paulo. Among the patients, 36 cases (55.4%) came to the Hospital
following previous treatment and 35 cases (53.8%) arrived with
advanced disease (M1). Of the individuals who arrived with M1, the
lung was the most frequent site of distant metastasis, representing
31 cases (88.6%). The average lag time was 15 months (SD=19.7).
Only one tumor was classified as benign neoplasia. The tumors were
located in the lower and upper limbs at a frequency of 44 (67.7%)
and 21 (32.3%) patients, respectively.
Tumors were classified as low grade, histological
grades I and II (41.5%); and high grade, histological grade III
(58.5%). Chemotherapy was performed in 32 patients (49.2%) and
radiotherapy in 33 patients (50.8%). Resection was the most common
surgery and was performed in 44 patients (68.8%), followed by
amputation in 20 patients (31.3%). One patient did not undergo a
surgical proceedure. During the follow-up, 28 patients died (43.1%)
and 32 relapsed (49.2%). Of all recurrences, 24 (75.0%) had local
recurrence. Mean patients follow-up of was 45 months.
Histological samples
Paraffin blocks of tumor samples were obtained from
65 patients diagnosed with STS from the Department of Pathology and
treated by Orthopaedic Oncology (Barretos Cancer Hospital). Areas
free of tumor involvement were used as control samples. The
confirmation of the quality and the pathological diagnosis of all
samples was performed by a pathologist. Following selection of
cases, socio-demographic and clinical data were collected from
patient medical records to characterize the samples. The
distribution of the histological classification of tumors was
performed according to the World Health Organization (1) and is depicted in Table I.
 | Table IDistribution of histological
classification. |
Table I
Distribution of histological
classification.
| Histological
classification | n | % |
|---|
| Pleomorphic
sarcoma | 14 | 21.54 |
| Leiomyosarcoma | 13 | 20.00 |
| Myxoid
liposarcoma | 12 | 18.46 |
| Myxofibrosarcoma | 3 | 4.62 |
| Sarcoma
fibromyxoid | 3 | 4.62 |
| No specified origin
sarcoma | 3 | 4.62 |
| Fibrosarcoma | 2 | 3.08 |
| Fibrosarcoma
sclerosing | 2 | 3.08 |
| Synovial sarcoma | 2 | 3.08 |
| Synovial sarcoma
monophasic | 2 | 3.08 |
| Fibromatosis | 1 | 1.54 |
|
Hemangioperycitoma | 1 | 1.54 |
| Round cell
liposarcoma | 1 | 1.54 |
| Dediferentiated
liposarcoma | 1 | 1.54 |
| Pleomorphic
liposarcoma | 1 | 1.54 |
| Pleomorphic
rhabdomyosarcoma | 1 | 1.54 |
| Clear cell
sarcoma | 1 | 1.54 |
| Biphasic synovial
sarcoma | 1 | 1.54 |
| Metastatic synovial
sarcoma | 1 | 1.54 |
Immunohistochemistry
Following deparaffinization and rehydration of
samples, antigen retrieval was performed using citrate buffer (10
mM, pH 6.0) for 30 min in a Pascal pressurized heating chamber
(Dako, Carpinteria, CA, USA). Following cooling, the tissue samples
were blocked in endogenous peroxidases (3% hydrogen peroxide in
methanol). Subsequently, the material was incubated with normal
horse serum or serum-free protein (Dako) for 1 h to block
non-specific protein. Primary antibodies against the protein Ki-67
(Dako) and CD100 (Abcam, Cambridge, MA, USA) were applied to the
samples according to the manufacturer’s instructions, using the
following dilutions: Ki-67 (1:100) and CD100 (1:100), with
overnight incubation at 4°C. Following this, peroxidase-conjugated
secondary antibody (Abcam) or the amplifier polymer ADVANCE HRP
detection system (Dako) were applied to the samples according to
the manufacturer’s instructions. Antibody binding was visualized
using chromogen diaminobenzidine (Sigma-Aldrich, St. Louis, MO,
USA) and counter-stained with hematoxylin. Positive controls for
each primary antibody were used according to the manufacturer’s
instructions.
Evaluation of CD100 and Ki-67
CD100 was evaluated on a scale from negative, +, ++,
+++ and the stained surface area was calculated (stained surface
area varied between 20 and 100%). For Ki-67, only nuclear reaction
was considered positive. Positive immunostaning was graded as
follows: negative (0); faintly positive, between 1 and 10 (+);
sporadic, >10 and 50 (++); and diffuse, >50 cells (+++) were
positive. In statistical calculations, positive reactions of the
markers were considered as positive or negative.
Images of histological sections were captured using
the Eclipse 50i microscope coupled to a Sight DS-FI1 digital video
camera (both from Nikon, Tokyo, Japan) and analyzed using the
Image-Pro Express (v6.0; Media Cybernetics, Rockville, MD,
USA).
Statistical analysis
Variables considered in this study for statistical
analysis were: ethnicity, gender, histological grade, survival at 3
and 5 years and expression of CD100 and Ki-67. To characterize the
study sample, data were summarized in terms of mean, standard
deviation, median, minimum and maximum, when the variables were
quantitative; and frequency and percentage for qualitative
variables. Global, disease-free and local or locoregional
disease-free survival were compared with the events, death from any
cause, local recurrence and local and/or regional recurrence,
respectively. Initially, the survival rates were estimated using a
nonparametric Kaplan-Meier estimator. The log-rank test was used to
verify the difference between survival curves for various strata of
the same variable. Following this, we used the Cox’s multiple
regression model to determine the effect of combinations of
variables. Data were correlated and analyzed with SPSS software
(for Windows, v19.0). P<0.05 was considered to indicate a
statistically significant difference.
Ethics
The present study was submitted to the Ethics
Committee in Research (Barretos Cancer Hospital; no. 331/2010).
Informed consent was not required as the study was a retrospective
cohort.
Results
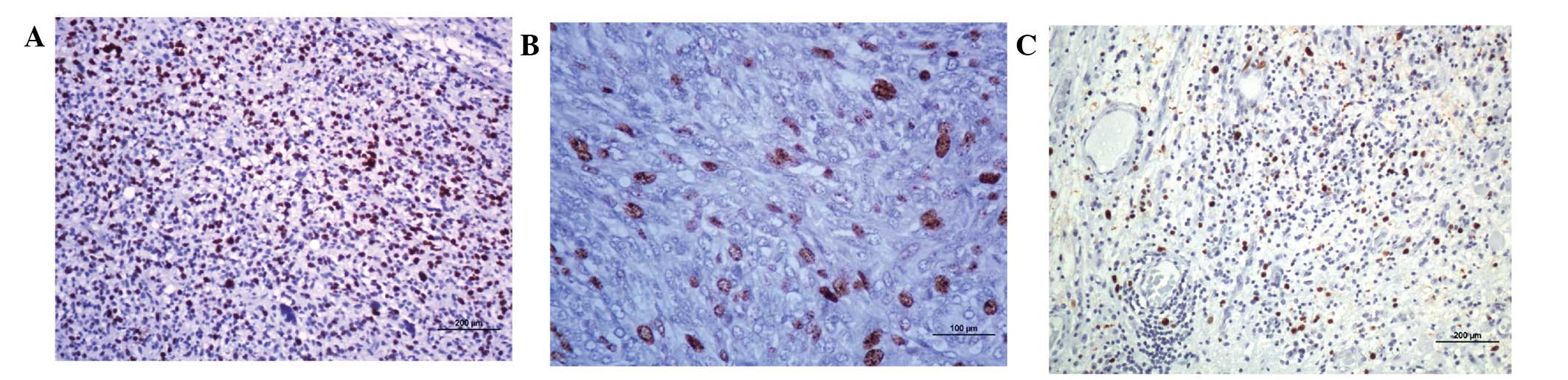
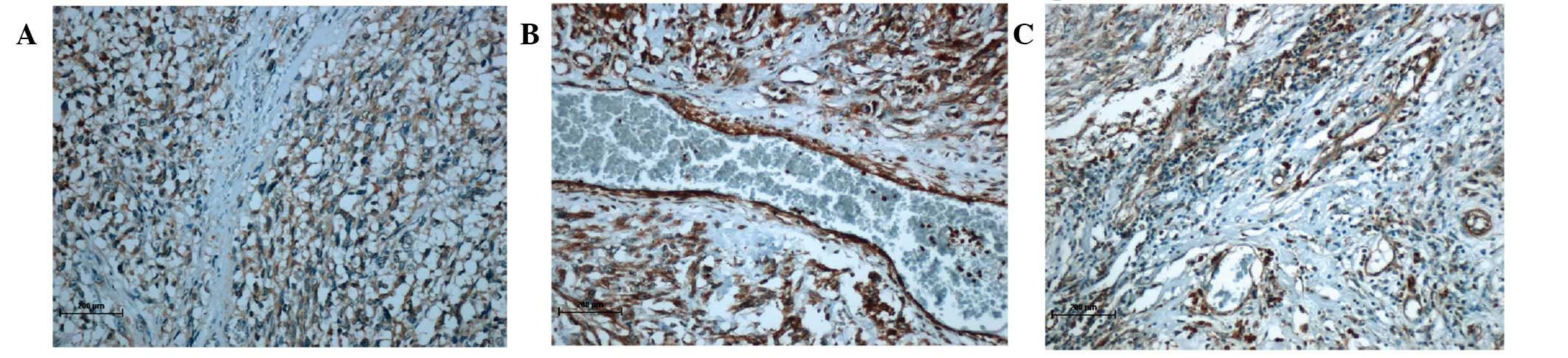
Expression of Ki-67 and CD100 markers in
STS
Labeling of Ki-67 was negative in ∼40% of tumor
samples. Marker expression was considered low, moderate and severe
in 27.7, 18.5 and 13.8% of patient samples, respectively (Table II, Fig.
1). Patient samples (∼18.5%) were negative for CD100, 24.6% had
moderate and weak expression (each group) and 32.3% of the samples
were identified to exhibit marked expression of the molecule
(Table II, Fig. 2).
| Table IIDistribuition of Ki-67 and CD100
expression. |
Table II
Distribuition of Ki-67 and CD100
expression.
| Variable | n | % |
|---|
| Ki-67 | | |
| Negative | 26 | 40.0 |
| + | 18 | 27.7 |
| ++ | 12 | 18.5 |
| +++ | 9 | 13.8 |
| CD100 | | |
| Negative | 12 | 18.5 |
| + | 16 | 24.6 |
| ++ | 16 | 24.6 |
| +++ | 21 | 32.3 |
| CD100 + Ki-67 | | |
| Negative/+ | 18 | 27.7 |
| ++/+++ | 47 | 72.3 |
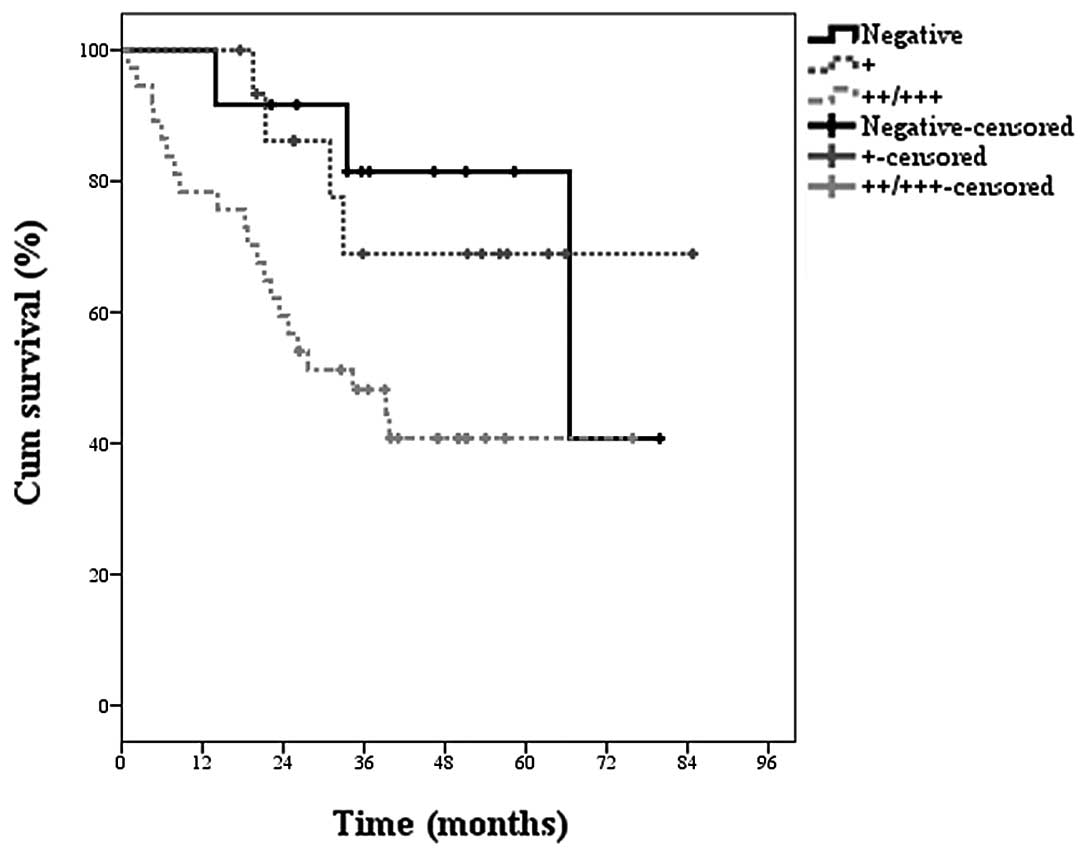
Univariate and multivariate analysis for
prognostic factors in STS
The histological grade of tumors was statistically
significant (P= 0.001) for the risk of death (global survival) in
patients. Similarly, our results demonstrated a statistically
significant correlation (P=0.037; Table
III) between the increased expression of CD100 and decreased
survival (Fig. 3). By contrast, the
analysis of Ki-67 expression in tissues was not statistically
significant when considering the overall disease-free survival.
When evaluating additional variables, including chemotherapy,
radiotherapy, surgery type, gender, ethnicity and previous
treatment, any statistical significance was identified by an
increase in overall survival.
| Table IIIEstimation of global survival by
Kaplan-Meier considering clinical variables/demographics. |
Table III
Estimation of global survival by
Kaplan-Meier considering clinical variables/demographics.
| | | Survival
probability (%)
| |
|---|
| Variables | Cases (n) | Mortalities
(n) | 1 year | 3 years | 5 years | P-value |
|---|
| Chemotherapy | | | | | | |
| No | 33 | 13 | 90.9 | 64.5 | 59.6 | 0.436 |
| Yes | 32 | 15 | 84.4 | 49.2 | 49.2 | |
| Radiotherapy | | | | | | |
| No | 32 | 13 | 84.4 | 54.7 | 54.7 | 0.861 |
| Yes | 33 | 15 | 90.9 | 62.6 | 54.8 | |
| Type of
surgery | | | | | | |
| Amputation | 20 | 9 | 75.0 | 52.5 | 52.5 | 0.381 |
| Resection | 44 | 19 | 93.2 | 62.6 | 56.7 | |
| Histological
grade | | | | | | |
| I/II | 27 | 7 | 100 | 84.1 | 74.2 | 0.001 |
| III | 38 | 21 | 78.9 | 40.8 | 40.8 | |
| Gender | | | | | | |
| Female | 23 | 8 | 91.3 | 67.3 | 67.3 | 0.223 |
| Male | 42 | 20 | 85.7 | 54.9 | 46.5 | |
| Ethnicity | | | | | | |
| Caucasian | 43 | 17 | 88.4 | 59.7 | 55.9 | 0.559 |
| Other | 22 | 11 | 86.4 | 57.8 | 51.4 | |
| Previous
treatment | | | | | | |
| No | 29 | 15 | 86.2 | 48.9 | 44.0 | 0.177 |
| Yes | 36 | 13 | 88.9 | 67.9 | 63.4 | |
| Ki-67 | | | | | | |
| Negative | 26 | 7 | 92.3 | 75.6 | 68.7 | 0.084 |
| + | 18 | 9 | 77.8 | 54.5 | 48.5 | |
| ++/+++ | 21 | 12 | 90.5 | 41.0 | 41.0 | |
| CD100 | | | | | | |
| Negative | 12 | 3 | 100 | 81.5 | 81.5 | 0.037 |
| + | 16 | 4 | 100 | 68.9 | 68.9 | |
| ++/+++ | 37 | 21 | 78.4 | 48.2 | 40.8 | |
In the assessment of local disease-free survival
(Table IV) there was statistical
significance for histological grade and expression of CD100. Again,
the analysis of expression of Ki-67, was unable to demonstrate the
significance of local disease-free survival. In addition, other
variables, including chemotherapy, radiotherapy, surgery type,
gender, ethnicity and previous treatment do not show statistical
significance.
| Table IVEstimated local disease free survival
by the Kaplan-Meier considering clinical
variables/demographics. |
Table IV
Estimated local disease free survival
by the Kaplan-Meier considering clinical
variables/demographics.
| | | Survival
probability (%)
| |
|---|
| Variables | Cases (n) | Recidives (n) | 1 year | 3 years | 5 years | P-value |
|---|
| Ethnicity | | | | | | |
| Caucasian | 43 | 14 | 80.2 | 65.0 | 65.0 | 0.283 |
| Other | 22 | 10 | 75.8 | 59.7 | - | |
| Gender | | | | | | |
| Female | 23 | 8 | 82.2 | 70.9 | 57.3 | 0.474 |
| Male | 42 | 16 | 76.6 | 58.3 | 58.2 | |
| Histological
grade | | | | | | |
| I | 27 | 10 | 85.2 | 70.0 | 65.3 | 0.298 |
| III | 38 | 14 | 73.8 | 56.0 | 46.7 | |
| Type of
surgery | | | | | | |
| Amputation | 20 | 5 | 80.0 | 72.0 | 72.0 | 0.448 |
| Resection | 44 | 19 | 78.3 | 59.9 | 52.9 | |
| Previous
treatment | | | | | | |
| No | 29 | 10 | 77.3 | 62.8 | 55.8 | 0.777 |
| Yes | 36 | 14 | 79.8 | 63.4 | 58.1 | |
| Chemotherapy | | | | | | |
| No | 33 | 11 | 87.2 | 67.1 | 56.3 | 0.363 |
| Yes | 32 | 13 | 69.8 | 58.9 | 58.9 | |
| Radiotherapy | | | | | | |
| No | 32 | 9 | 86.1 | 68.3 | 68.3 | 0.234 |
| Yes | 33 | 15 | 72.0 | 58.3 | 48.6 | |
| Ki-67 | | | | | | |
| Negative | 26 | 8 | 88.5 | 75.5 | 69.2 | 0.016 |
| + | 18 | 4 | 92.9 | 68.6 | 68.6 | |
| ++/+++ | 21 | 12 | 55.1 | 50.1 | - | |
| CD100 | | | | | | |
| Negative | 12 | 4 | 100 | 91.7 | 62.9 | 0.298 |
| + | 16 | 5 | 81.3 | 65.2 | 65.2 | |
| ++/+++ | 37 | 15 | 69.8 | 51.3 | 51.3 | |
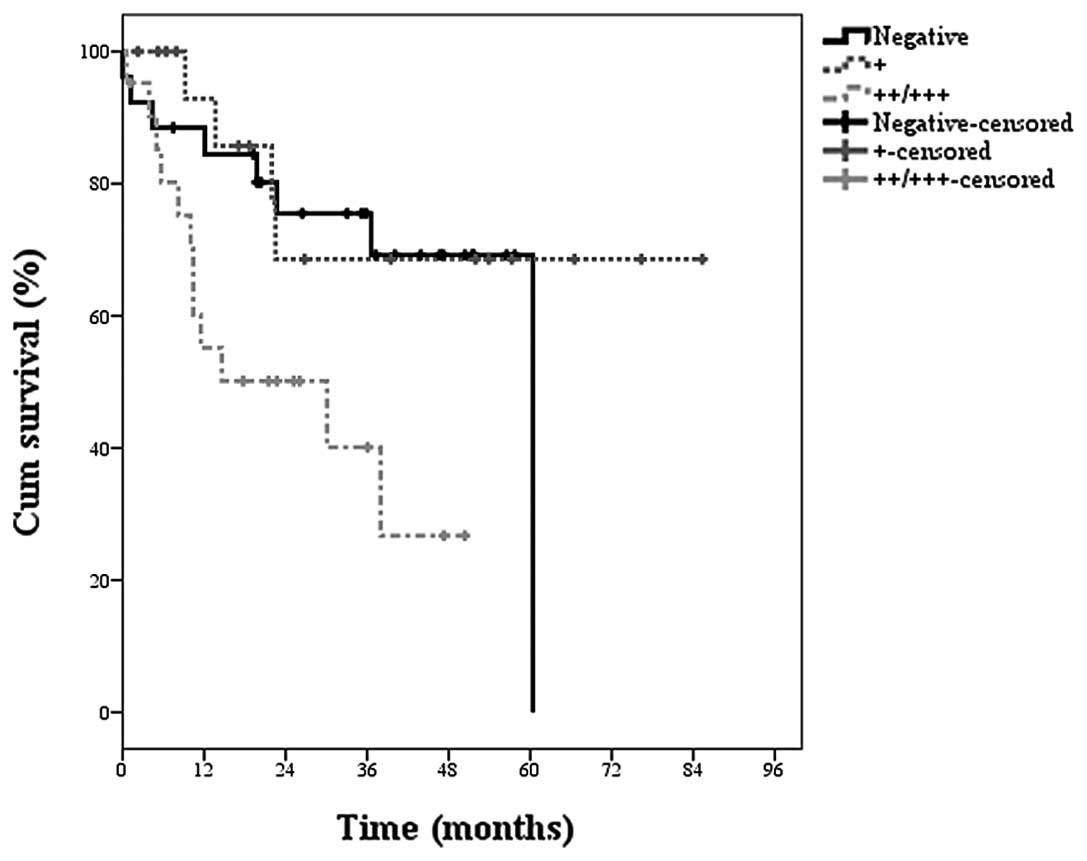
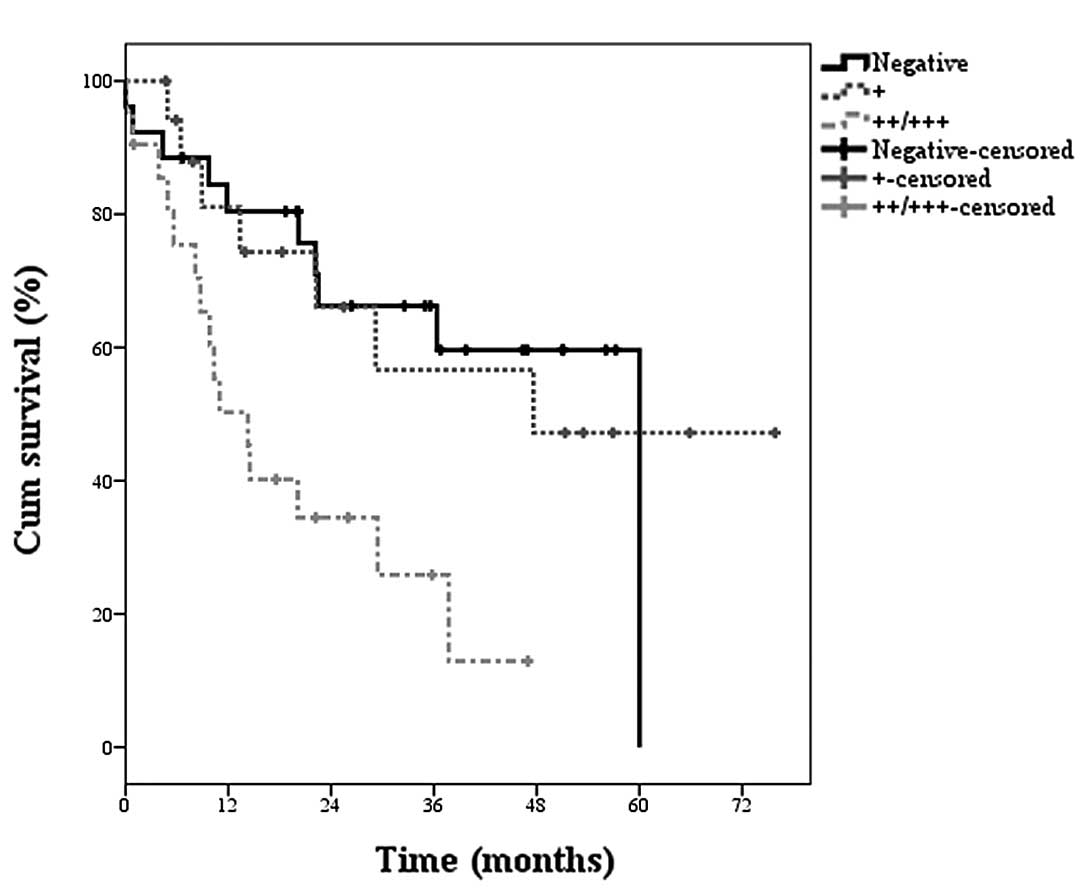
Statistical analysis of local recurrence free
survival (Table V) showed that the
expression of Ki-67 in STS samples correlated significantly with
the incidence of local recurrence in tumors. Fig. 4 presents the estimated nonparametric
survival curve. Conversely, the evaluation of the expression of
CD100 was not able to demonstrate significant for the event of
local recurrence. Similarly, there was no significance to the event
of local recurrence for the variables: chemotherapy, radiotherapy,
surgery type, gender, ethnicity and pretreatment. In addition, the
locoregional recurrence-free survival (Table V), the expression of Ki-67 was again
significant for the incidence of local recurrence and/or regional
STS and estimation of the survival curve is shown in Fig. 5. Similarly, the evaluation of the
expression of CD100 was not able to show significance for the event
of recurrence. The other variables (chemotherapy, radiotherapy,
surgery type, gender, ethnicity and previous treatment), were not
able to predict the event of local recurrence and/or regional level
in patients.
| Table VEstimation of locoregional disease
free survival by Kaplan-Meier considering clinical
variables/demographics. |
Table V
Estimation of locoregional disease
free survival by Kaplan-Meier considering clinical
variables/demographics.
| | | Survival
probability (%)
| |
|---|
| Variables | Cases (n) | Recidives (n) | 1 year | 3 years | 5 years | P-value |
|---|
| Chemotherapy | | | | | | |
| No | 33 | 16 | 77.3 | 52.6 | 33.1 | 0.661 |
| Yes | 32 | 16 | 64.3 | 49.6 | 00.0 | |
| Radiotherapy | | | | | | |
| No | 32 | 14 | 78.7 | 51.5 | 20.6 | 0.553 |
| Yes | 33 | 18 | 63.6 | 49.5 | 40.5 | |
| Type of
surgery | | | | | | |
| Amputation | 20 | 7 | 74.7 | 56.9 | 56.9 | 0.541 |
| Resection | 44 | 25 | 69.2 | 48.8 | 18.8 | |
| Histological
grade | | | | | | |
| I/II | 27 | 15 | 74.1 | 54.5 | 21.2 | 0.649 |
| III | 38 | 17 | 68.9 | 48.3 | 40.3 | |
| Gender | | | | | | |
| Female | 23 | 12 | 73.2 | 53.0 | 40.3 | 0.817 |
| Male | 42 | 20 | 69.5 | 49.7 | 00.00 | |
| Ethnicity | | | | | | |
| Caucasian | 43 | 21 | 73.1 | 49.3 | 28.8 | 0.769 |
| Other | 22 | 11 | 66.0 | 54.2 | - | |
| Previous
treatment | | | | | | |
| No | 29 | 11 | 77.3 | 57.8 | 50.6 | 0.142 |
| Yes | 36 | 21 | 65.7 | 46.0 | 0.00 | |
| Ki-67 | | | | | | |
| Negative | 26 | 10 | 84.4 | 66.2 | 0.00 | 0.006 |
| + | 18 | 7 | 81.1 | 56.6 | 47.2 | |
| ++/+++ | 21 | 15 | 50.3 | 25.9 | 12.9 | |
| CD100 | | | | | | |
| Negative | 12 | 5 | 91.7 | 81.5 | 0.00 | 0.101 |
| + | 16 | 7 | 81.3 | 59.1 | 49.2 | |
| ++/+++ | 37 | 20 | 55.3 | 35.8 | 35.8 | |
In order to understand the behavior set of variables
was used Cox’s multiple regression model. In addition to the
markers that were statistically significant considering the
log-rank test were also adjusted variables: histological grade,
chemotherapy, radiotherapy and pretreatment. The results of
adjusting the Cox model are presented in Tables VI, VII and VIII for global survival, local
disease-free survival and locoregional disease free survival,
respectively. For global survival, only histological grade and
CD100 were statistically significant (Table VI). Patients with histological grade
I/II has 0.16 risk of death as compared to patients with
histological grade III, characterizing histological grades I/II as
a protective factor. In evaluating the expression of CD100,
patients with low expression (+), have 0.19 risk of death as
compared to patients with higher expression (++/+++). Accordingly,
low expression of CD100 (+), is a protective factor when compared
with increased expression, represented here as patients with two or
three crosses (++/+++).
| Table VIEstimate of relative risk by Cox
multiple model for times of global survival. |
Table VI
Estimate of relative risk by Cox
multiple model for times of global survival.
| | | | 95% CI
| |
|---|
| Variables | Cases (n) | Mortalities
(n) | Relative risk | Lower | Upper | P-value |
|---|
| Histological
grade | | | | | | |
| I/II | 27 | 15 | 0.161 | 0.059 | 0.440 | <0.001 |
| III | 38 | 17 | - | - | - | - |
| Chemotherapy | | | | | | |
| No | 33 | 13 | 0.552 | 0.241 | 1.260 | 0.158 |
| Yes | 32 | 15 | - | - | - | - |
| Radiotherapy | | | | | | |
| No | 32 | 9 | 1.132 | 0.513 | 2.500 | 0.759 |
| Yes | 33 | 15 | - | - | - | - |
| Previous
treatment | | | | | | |
| No | 29 | 15 | 2.476 | 2.476 | 1.096 | 5.593 |
| Yes | 36 | 13 | - | - | - | - |
| CD100 | | | | | | |
| Negative | 12 | 5 | 0.378 | 0.112 | 1.284 | 0.119 |
| + | 16 | 7 | 0.192 | 0.063 | 0.586 | 0.004 |
| ++/+++ | 37 | 20 | - | - | - | - |
| Table VIIEstimate of relative risk by Cox
multiple model for times of local disease-free survival. |
Table VII
Estimate of relative risk by Cox
multiple model for times of local disease-free survival.
| | | | 95% CI
| |
|---|
| Variables | Cases (n) | Recidives (n) | Relative risk | Lower | Upper | P-value |
|---|
| Histological
grade | | | | | | |
| I/II | 27 | 10 | 0.905 | 0.367 | 2.229 | 0.828 |
| III | 38 | 14 | - | - | - | - |
| Chemotherapy | | | | | | |
| No | 33 | 11 | 0.780 | 0.328 | 1.857 | 0.575 |
| Yes | 32 | 13 | - | - | - | - |
| Radiotherapy | | | | | | |
| No | 32 | 9 | 0.581 | 0.247 | 1.365 | 0.213 |
| Yes | 33 | 15 | - | - | - | - |
| Previous
treatment | | | | | | |
| No | 29 | 10 | 1.029 | 0.439 | 2.410 | 0.947 |
| Yes | 36 | 14 | - | - | - | - |
| Ki-67 | | | | | | |
| Negative | 26 | 8 | 0.338 | 0.127 | 0.903 | 0.030 |
| + | 18 | 4 | 0.271 | 0.078 | 0.942 | 0.040 |
| ++/+++ | 21 | 12 | - | - | - | - |
| Table VIIIEstimate of relative risk by Cox
multiple model for times of locoregional disease-free survival. |
Table VIII
Estimate of relative risk by Cox
multiple model for times of locoregional disease-free survival.
| | | | 95% CI
| |
|---|
| Variables | Cases (n) | Recidives (n) | Relative risk | Lower | Upper | P-value |
|---|
| Histological
grade | | | | | | |
| I/II | 27 | 15 | 1.105 | 0.527 | 2.316 | 0.230 |
| III | 38 | 17 | - | - | - | - |
| Chemotherapy | | | | | | |
| No | 33 | 16 | 0.814 | 0.383 | 1.731 | 0.593 |
| Yes | 32 | 16 | - | - | - | - |
| Radiotherapy | | | | | | |
| No | 32 | 14 | 0.689 | 0.337 | 1.411 | 0.309 |
| Yes | 33 | 18 | - | - | - | - |
| Previous
treatment | | | | | | |
| No | 29 | 11 | 0.630 | 0.296 | 1.340 | 0.230 |
| Yes | 36 | 21 | - | - | - | - |
| Ki-67 | | | | | | |
| Negative | 26 | 10 | 0.279 | 0.115 | 0.679 | 0.005 |
| + | 18 | 7 | 0.365 | 0.140 | 0.951 | 0.039 |
| ++/+++ | 21 | 15 | - | - | - | - |
The negative expression for this marker was not
significant at 0.05 and we hypothesize that this had occurred due
to the low number of events associated with this result.
In the analysis of local disease-free survival and
locoregional disease-free survival, only Ki-67 was a significant
marker (Tables VII and VIII, respectively). In both cases,
negative or low (+) Ki-67 expression is characterized as a
protective factor compared with increased expression (++ or +++).
For local disease-free survival, patients with negative Ki-67
expression have 0.28 times the chance of local recurrence, compared
with higher expression of the molecule (++ or +++). Also, for the
expression of low Ki-67 (+) the chance of local recurrence is 0.36.
For locoregional disease-free survival, patients with negative
Ki-67 expression have a 0.28 chance of local and/or regional
recurrence as compared to those who present a higher expression of
the marker (++ or +++). Low expression of the molecule (+) has a
relative risk of 0.365 for locoregional recurrence.
Discussion
A number of previous studies have aimed to establish
more effective prognostic criteria for STSs using parameters
associated with location and/or tumor size, histological grade or
the expression of biomarkers in clinical samples (2,4). As a
prognostic factor, histological grade is currently considered to be
the most reliable marker for STSs (2). In the present study, histological
grade showed a statistically significant (P=0.001) value for the
risk of death (global disease-free survival) in patients.
Histological grade is commonly analyzed to predict disease
progression in STSs, was confirmed as a suitable marker for local
and global survival analysis.
Previous studies have analyzed CD100 and Ki-67
levels in STSs. However, in the present study expression of CD100
and Ki-67 proteins in STSs was analyzed by immunohistochemistry in
a patient population to establish their suitability as potential
clinical prognostic markers. Expression of CD100 was identified to
be significantly different in patients with high and decreased
rates of survival (P=0.037). Ki-67 was not revealed to correlate
with overall disease-free survival. This particular scenario was
repeated when we evaluate the local disease-free survival that
indicated significant value of histological grade and expression of
CD100 for worse prognosis. Again, Ki-67 expression was not
associated with local disease-free survival.
As discussed, CD100 is associated with a number of
tumorigenic processes, including regulation of immune cells and
angiogenesis (23). Recently, Kato
et al(24) demonstrated that
lymphocytes infiltrating pancreatic ductal adenocarcinoma
overexpress Sema4D and its receptor Plexin B1. Levels of these
molecules correlate with clinical factors, including poor prognosis
and metastasis. In addition, Plexin B1 expression was identified to
correlate with poor prognosis in ER-positive breast cancer
(25). The potential of CD100 as a
biomarker in STSs was confirmed in the current study (22). CD100 expression was identified to
significantly correlate with global and local survival free of
disease in patients, consistent with Ch’ng et al(22). Therefore, we conclude that CD100
expression levels are suitable for evaluation of tumors from STS
patients to determine prognosis.
CD100 expression levels were not identified to
predict local relapse-free survival in patients. Only Ki-67 was
identified as a biomarker for prediction of disease recurrence in
patients, whereby local and locoregional recurrence-free survival
was revealed to correlate with Ki-67 expression in tissues. Ki-67
is expressed throughout the majority of the cell cycle and is
considered to be an excellent marker of cell division (5,26).
However, Ki-67 was not demonstrated to predict disease-free
survival in global or local tumors. Several studies have reported
Ki-67 as a prognostic factor in various tumor types (6). A number of previous studies have
reported Ki-67 to be a poor prognostic factor (27,28).
However, more recently the protein was identified as a marker of
specific STS subtypes suitable for adjuvant therapy (29) as well as a predictive marker of
distant tumor metastases (7,30). To
date, a large casuistic study has not demonstrated the correlation
of this cell proliferation marker with local recurrence in STSs.
Only a single study with a limited number of cases of uterine
sarcoma (gynecological sarcomas are not included in the current
study), has identified a correlation between local recurrence and
Ki-67 expression (31).
The present study demonstrates that Ki-67 is a
prognostic marker of local recurrence and/or locoregional relapse
in STSs and may prove a suitable tool for the clinical management
of disease progression. In addition, results demonstrate that CD100
expression is an indicator of poor prognosis of STSs. The use of
these markers in routine clinical pathology may be useful as an
important prognostic criterion of disease progression.
References
|
1
|
Fletcher CDM, Sundaram M, Rydholm A,
Coindre JM and Singer S: Soft tissue tumours: Epidemiology,
clinical features, histopathological typing and grading. World
Health Organization, International Agency for Research on Cancer.
Pathology and Genetics of Tumours of Soft Tissue and Bone. Fletcher
CDM, Unni KK and Mertens F: IARC Press; Lyon: pp. 12–18. 2002
|
|
2
|
Jones NB, Iwenofu H, Scharschmidt T and
Kraybill W: Prognostic factors and staging for soft tissue
sarcomas: an update. Surg Oncol Clin N Am. 21:187–200. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Taylor BS, Barretina J, Maki RG, Antonescu
CR, Singer S and Ladanyi M: Advances in sarcoma genomics and new
therapeutic targets. Nat Rev Cancer. 11:541–557. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ottaiano A, De Chiara A, Fazioli F,
Talamanca AA, Mori S, Botti G, Milano A and Apice G: Biological
prognostic factors in adult soft tissue sarcomas. Anticancer Res.
25:4519–4526. 2005.PubMed/NCBI
|
|
5
|
Endl E and Gerdes J: The Ki-67 protein:
fascinating forms and an unknown function. Exp Cell Res.
257:231–237. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Brown DC and Gatter KC: Ki67 protein: the
immaculate deception? Histopathology. 40:2–11. 2002. View Article : Google Scholar
|
|
7
|
Hoos A, Stojadinovic A, Mastorides S,
Urist MJ, Polsky D, Di Como CJ, Brennan MF and Cordon-Cardo C: High
Ki-67 proliferative index predicts disease specific survival in
patients with high-risk soft tissue sarcomas. Cancer. 92:869–874.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Heslin MJ, Cordon-Cardo C, Lewis JJ,
Woodruff JM and Brennan MF: Ki-67 detected by MIB-1 predicts
distant metastasis and tumor mortality in primary, high grade
extremity soft tissue sarcoma. Cancer. 83:490–497. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hall KT, Boumsell L, Schultze JL,
Boussiotis VA, Dorfman DM, Cardoso AA, Bensussan A, Nadler LM and
Freeman GJ: Human CD100, a novel leukocyte semaphorin that promotes
B-cell aggregation and differentiation. Proc Natl Acad Sci USA.
93:11780–11785. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Goodman CS, Kolodkin AL, Luo Y, Püschel AW
and Raper JA: Unified nomenclature for the semaphorins/collapsins.
Cell. 97:551–552. 1999. View Article : Google Scholar
|
|
11
|
Kumanogoh A, Watanabe C, Lee I, Wang X,
Shi W, Araki H, Hirata H, Iwahori K, Uchida J, Yasui T, Matsumoto
M, Yoshida K, Yakura H, Pan C, Parnes JR and Kikutani H:
Identification of CD72 as a lymphocyte receptor for the class IV
semaphoring CD100: a novel mechanism for regulating B cell
signaling. Immunity. 13:621–631. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tessier-Lavigne M and Goodman SC: The
molecular biology of axon guidance. Science. 274:1123–1133. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Luo Y, Raible D and Raper JA: Collapsin: a
protein in brain that induces the collapse and paralysis of
neuronal growth cones. Cell. 75:217–227. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kolodkin AL, Matthes DJ and Goodman CS:
The semaphorin genes encode a family of transmembrane and secreted
growth cone guidance molecules. Cell. 75:1389–1399. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Behar O, Golden JA, Mashimo H, Schoen FJ
and Fishman MC: Semaphorin III is needed for normal patterning and
growth of nerves, bones and heart. Nature. 383:525–528. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kitsukawa T, Shimono A, Kawakami A, Kondoh
H and Fujisawa H: Overexpression of a membrane protein, neuropilin,
in chimeric mice causes anomalies in the cardiovascular system,
nervous system and limbs. Development. 121:4309–4318. 1995.
|
|
17
|
Roche J, Boldog F, Robinson M, Robinson L,
Varella-Garcia M, Swanton M, Waggoner B, Fishel R, Franklin W,
Gemmill R and Drabkin H: Distinct 3p21.3 deletions in lung cancer
and identification of a new human semaphorin. Oncogene.
12:1289–1297. 1996.PubMed/NCBI
|
|
18
|
Sekido Y, Bader S, Latif F, Chen JY, Duh
FM, Wei MH, et al: Human semaphorins A(V) and IV reside in the
3p21.3 small cell lung cancer deletion region and demonstrate
distinct expression patterns. Proc Natl Acad Sci USA. 93:4120–4125.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mizui M, Kumanogoh A and Kikutani H:
Immune semaphorins: novel features of neural guidance molecules. J
Clin Immunol. 29:1–11. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Conrotto P, Valdembri D, Corso S, Serini
G, Tamagnone L, Comoglio PM, Bussolino F and Giordano S: Sema4D
induces angiogenesis through Met recruitment by Plexin B1. Blood.
105:4321–4329. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Conrotto P, Corso S, Gamberini S, Comoglio
PM and Giordano S: Interplay between scatter factor receptors and B
plexins controls invasive growth. Oncogene. 23:5131–5137. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ch’ng E, Tomita Y, Zhang B, He J, Hoshida
Y, Qiu Y, Morii E, Nakamichi I, Hamada K, Ueda T and Aozasa K:
Prognostic significance of CD100 expression in soft tissue sarcoma.
Cancer. 110:164–172. 2007.PubMed/NCBI
|
|
23
|
Ch’ng ES and Kumanogoh A: Roles of Sema4D
and Plexin-B1 in tumor progression. Mol Cancer.
9:2512010.PubMed/NCBI
|
|
24
|
Kato S, Kubota K, Shimamura T, Shinohara
Y, Kobayashi N, Watanabe S, Yoneda M, Inamori M, Nakamura F,
Ishiguro H, Nakaigawa N, Nagashima Y, Taguri M, Kubota Y, Goshima
Y, Morita S, Endo I, Maeda S, Nakajima A and Nakagama H: Semaphorin
4D, a lymphocyte semaphorin, enhances tumor cell motility through
binding its receptor, plexinB1, in pancreatic cancer. Cancer Sci.
102:2029–2037. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Rody A, Holtrich U, Gaetje R, Gehrmann M,
Engels K, von Minckwitz G, Loibl S, Diallo-Danebrock R, Ruckhäberle
E, Metzler D, Ahr A, Solbach C, Karn T and Kaufmann M: Poor outcome
in estrogen receptor-positive breast cancers predicted by loss of
plexin B1. Clin Cancer Res. 13:1115–1122. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gerdes J: Ki-67 and other proliferation
markers useful for immunohistological diagnostic and prognostic
evaluations in human malignancies. Semin Cancer Biol. 1:199–206.
1990.PubMed/NCBI
|
|
27
|
Choong PF, Akerman M, Willén H, Andersson
C, Gustafson P, Baldetorp B, Fernö M, Alvegård T and Rydholm A:
Prognostic value of Ki-67 expression in 182 soft tissue sarcomas.
Proliferation - a marker of metastasis? APMIS. 102:915–924. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ueda T, Aozasa K, Tsujimoto M, Ohsawa M,
Uchida A, Aoki Y, Ono K and Matsumoto K: Prognostic significance of
Ki-67 reactivity in soft tissue sarcomas. Cancer. 63:1607–1611.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jensen V, Sørensen FB, Bentzen SM,
Ladekarl M, Nielsen OS, Keller J and Jensen OM: Proliferative
activity (MIB-1 index) is an independent prognostic parameter in
patients with high-grade soft tissue sarcomas of subtypes other
than malignant fibrous histiocytomas: a retrospective
immunohistological study including 216 soft tissue sarcomas.
Histopathology. 32:536–546. 1998. View Article : Google Scholar
|
|
30
|
Huutanen RL, Blomqvist CP, Wiklund TA,
Böhling TO, Virolainen MJ, Tukiainen EJ, Tribukait B and Andresson
LC: Comparison of the Ki-67 score and S-phase fraction as
prognostic variables in soft-tissue sarcoma. Br J Cancer.
79:945–951. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Popiolek D, Yee H, Levine P, Vamvakas E
and Demopoulos RI: MIB1 as a possible predictor of recurrence in
low-grade endometrial stromal sarcoma of the uterus. Gynecol Oncol.
90:353–357. 2003. View Article : Google Scholar : PubMed/NCBI
|