Introduction
Leptomeningeal metastasis (LM) occurs when cancer
cells spread to the meninges, the layers of tissue that cover the
brain and spinal cord. Metastases spread to the meninges through
the blood or carried by the cerebrospinal fluid (CSF) that flows
through the meninges (1). The
incidence rate of LM is ∼5% worldwide, with a poor prognosis. The
median survival of patients with LM is ∼3 months (2,3) and
the current treatment methods include localized radiation therapy,
intrathecal chemotherapy or systemic chemotherapy (1). Non-small cell lung carcinoma (NSCLC)
consists of any type of epithelial lung cancer other than small
cell lung carcinoma (SCLC). The present case report describes a
patient with LM from SCLC who responded to gemcitabine plus
oxaliplatin. The procedure followed complied with the ethical
standards of the Changhai Hospital Institutional Review Board (IRB)
and was approved by the hospital committee. Informed written
consent was obtained from the subject.
Case report
A 62-year-old male patient (weight, 65 kg; height,
166 cm) was admitted to Changhai hospital, The Second Military
Medical University (Shanghai, China), due to coughing and chest
pain that had occurred for 5 months. The patient had suffered an
unexplained dry cough since September 2005, accompanied by chest
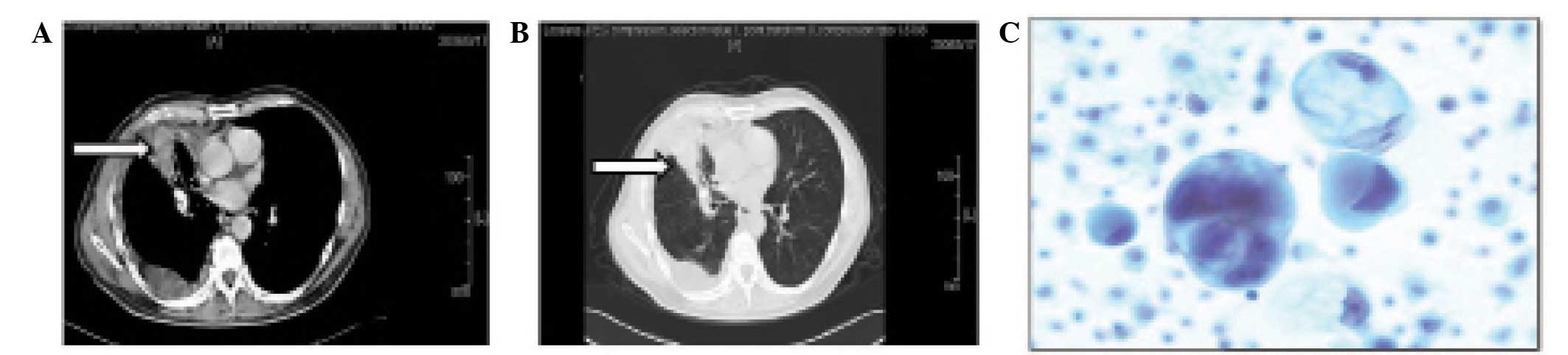
tightness and pain. In March 2006, a chest X-ray showed a shadow in
the right lower lung with a small amount of pleural effusion. The
chest computerized tomography (CT) showed a 2×1.5 cm block shadow
in the right lower lung, a medium dose pleural effusion in the
right chest cavity and certain mediastinal lymph nodes with
calcification (Fig. 1A and B). The
emission CT (ECT) showed numerous bone metastases. On March 27th,
2006 (week 0), a tube was placed in the right chest cavity and
drained 2400 ml of the pleural effusion. The entire pleural
effusion was drained after 3 days and consisted of ∼3,020 ml in
total. Adenocarcinoma cells were identified in smears of the
pleural effusion (Fig. 1C) and the
diagnosis from a Board Certified Pathologist was determined as that
of a right lower lung adenocarcinoma (T4N2M1, stage IV). Following
admission, the patient began to develop a severe headache with
nausea and vomiting but without cranial and spinal nerve
dysfunction, or signs of leptomeningeal irritation, such as
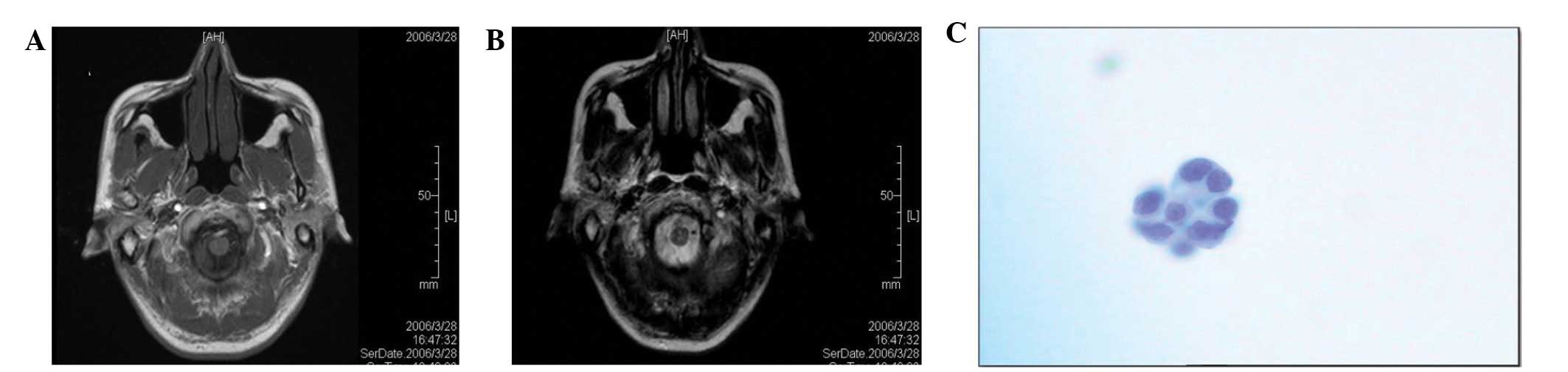
Brudzinski’s or Kernig’s sign. There were no abnormal signs in the
head magnetic resonance (MR; Fig. 2A
and B) or gastroscopy images. In the first week, a lumbar
puncture was performed and the pressure of the CSF was 18 cm
H2O. The result of the test was colorless, positive for
protein, had a total cell number of 10×106/l and
contained cancer cells (Fig. 2C)
(4). Chemotherapy was started with
1.8 g/day gemcitabine (from days 1–8) and 200 mg oxaliplatin (on
day 1 only). The headache symptoms were notably eased after the
first week and disappeared completely in the second week. The
symptoms of coughing and chest pain were also alleviated.
Chemotherapy was administered again in weeks 4 (cycle 2), 7 (cycle
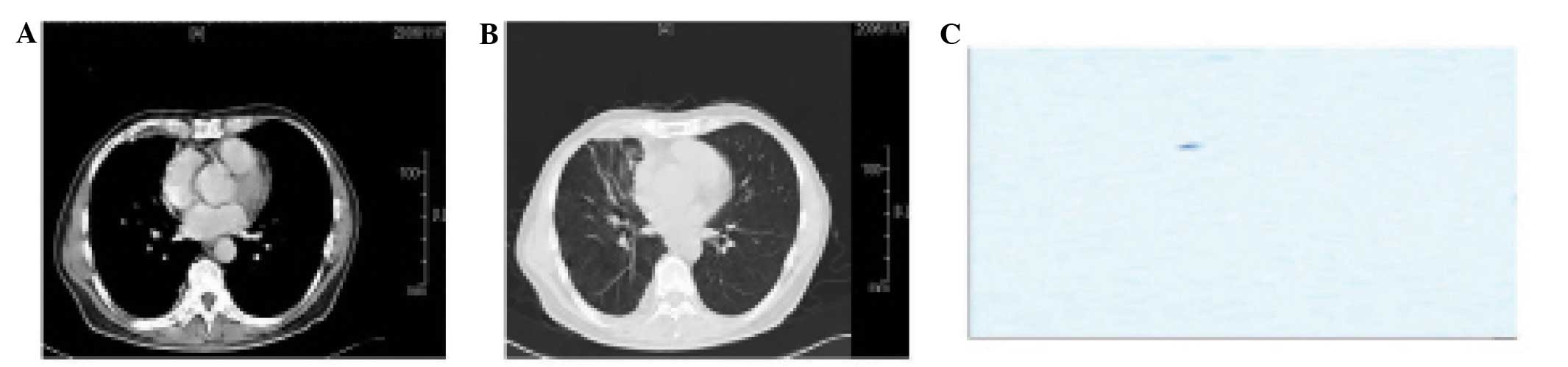
3) and 9 (cycle 4). In week 12, the pressure of the CSF was 12 cm
H2O. The CSF analysis was colorless, positive for
protein, had a total cell number of 0/l and contained no cancer
cells (Fig. 3C). The CT showed that
the shadow in the right lower lung was 0.5×0.5 cm and that the
pleura of the right chest was thickened (Fig. 3A and B). Another 4 cycles of
chemotherapy were administered. The patient was monitored by
monthly visits until January 30th, 2007 (week 44). During this time
the patient was stable. On April 29th, 2007 (week 57), the primary
tumor in the lung was observed to have progressed and 250 mg
gefitinib a day was administered.
Discussion
A number of malignancies may cause LM, among which
breast, lung [particularly adenocarcinoma (5)] and urinary tract tumors are the most
common and account for ∼80% (6). An
undifferentiated pathology type and other distant metastases are
independent risk factors for LM (7). The clinical features of LM may include
an intractable headache, nausea, vomiting, dizziness and
alterations in mood and consciousness (8). In cases where the cranial nerve is
attacked, symptoms may include diplopia, impaired vision, facial
numbness, difficulties in swallowing and abnormalities in tasting
and hearing (9). In addition, there
may also be disruption to the cauda equina, pseudomeningitis or no
symptoms at all (10). The most
common symptoms are headaches, mental and behavioral changes (often
first detected by family members) and facets of higher cortical
functions, including impaired comprehension, reading, calculation
and difficulty performing motor function tasks, such as eating or
dressing. Acute or rarer symptoms, including seizures (10–15%) or
intratumoral bleeding (10%), are more common in metastatic
melanomas (11). The gold standard
for the identification of LM is identifying tumor cells of the same
pathological type as the primary focus. The main symptoms of the
patient in the present case were a stubborn headache, nausea and
vomiting. Tumor cells were observed in the CSF sample. Therefore,
the diagnosis of this patient was confirmed.
For patients with LM, few therapeutic options are
available other than palliative measures, which include whole brain
irradiation or intrathecal chemotherapy (12). LM from NSCLC is a difficult disease
to treat and remains a major obstacle in the clinical course of
NSCLC. Although the majority of the clinical chemotherapy drugs are
not able to get through the blood-brain barrier, the present study
observed that systemic anti-cancer drugs prolonged the survival
period and rates of patients with LM from NSCLC. This may be as the
transfer of LM disrupts the blood-brain barrier, which allows the
chemotherapy drugs to penetrate into the brain and function there.
Drugs such as methotrexate, cytarabine and thiotepa are not the
most efficient for NSCLC patients, so they are no longer used for
the treatment of NSCLC with meningeal metastasis. At present,
patients receiving first-time treatment often receive
platinum-based drugs in combination with gemcitabine, paclitaxel,
vinorelbine or other treatments, which have achieved a higher
remission rate (13).
Few cases report that these first-line
chemotherapies have been used for the treatment of NSCLC patients
with LM (14–16). In the present study, the stage IV
NSCLC patient, who received gemcitabine plus oxaliplatin for four
courses, achieved a partial remission and the LM was
controlled.
This study suggests that first-line chemotherapy
using gemcitabine and platinum-containing drugs may be effective
for the treatment of NSCLC patients with LM. In addition, the
epidermal growth factor receptor (EGFR) and tyrosine kinase
inhibitors (TKI), including gefitinib and erlotinib, have been
shown to have greater efficacy in LM (17). These new molecularly targeted drugs
may act as another treatment option. However, further research is
required (18–20).
References
|
1
|
Taillibert S, Laigle-Donadey F,
Chodkiewicz C, Sanson M, Hoang-Xuan K and Delattre JY:
Leptomeningeal metastases from solid malignancy: a review. J
Neurooncol. 75:85–99. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gerrard GE and Franks KN: Overview of the
diagnosis and management of brain, spine, and meningeal metastases.
J Neurol Neurosurg Psychiatry. 75(Suppl 2): ii37–ii42. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Oechsle K, Lange-Brock V, Kruell A,
Bokemeyer C and de Wit M: Prognostic factors and treatment options
in patients with leptomeningeal metastases of different primary
tumors: a retrospective analysis. J Cancer Res Clin Oncol.
136:1729–1735. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Twijnstra A, Ongerboer de Visser BW and
van Zanten AP: Diagnosis of leptomeningeal metastasis. Clinical
Neurol Neurosurg. 89:79–85. 1987. View Article : Google Scholar
|
|
5
|
Chuang TY, Yu CJ, Shih JY, Yang PC and Kuo
SH: Cytologically proven meningeal carcinomatosis in patients with
lung cancer: clinical observation of 34 cases. J Formos Med Assoc.
107:851–856. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wasserstrom WR, Glass JP and Posner JB:
Diagnosis and treatment of leptomeningeal metastases from solid
tumors: experience with 90 patients. Cancer. 49:759–772. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Strady C, Ricciarelli A, Nasca S,
Liautaud-Roger F and Coninx P: Carcinomatous meningitis and solid
tumours. Oncol Rep. 7:203–207. 2000.PubMed/NCBI
|
|
8
|
Waki F, Ando M, Takashima A, et al:
Prognostic factors and clinical outcomes in patients with
leptomeningeal metastasis from solid tumors. J Neurooncol.
93:205–212. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kesari S and Batchelor TT: Leptomeningeal
metastases. Neurol Clin. 21:25–66. 2003. View Article : Google Scholar
|
|
10
|
Park JH, Kim YJ, Lee JO, et al: Clinical
outcomes of leptomeningeal metastasis in patients with non-small
cell lung cancer in the modern chemotherapy era. Lung Cancer.
76:387–392. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Westphal M, Heese O and de Wit M:
Intracranial metastases: therapeutic options. Ann Oncol. 14(Suppl
3): iii4–iii10. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chamberlain MC: Neoplastic meningitis. J
Clinical Oncol. 23:3605–3613. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ahmed SA, Gogal RM Jr and Walsh JE: A new
rapid and simple non-radioactive assay to monitor and determine the
proliferation of lymphocytes: an alternative to [3H]thymidine
incorporation assay. J Immunol Methods. 170:211–224.
1994.PubMed/NCBI
|
|
14
|
Paydas S, Bicakci K and Yavuz S: Dramatic
response with capecitabine after cranial radiation to the brain
parenchymal and leptomeningeal metastases from lung cancer. Eur J
Intern Med. 20:96–99. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen YM, Chen MC, Tsai CM and Perng RP:
Intrathecal gemcitabine chemotherapy for non-small cell lung cancer
patients with meningeal carcinomatosis - a case report. Lung
Cancer. 40:99–101. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sakai M, Ishikawa S, Ito H, et al:
Carcinomatous meningitis from non-small-cell lung cancer responding
to gefitinib. Int J Clin Oncol. 11:243–245. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sharma SV, Bell DW, Settleman J and Haber
DA: Epidermal growth factor receptor mutations in lung cancer.
Nature Rev Cancer. 7:169–181. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Choong NW, Dietrich S, Seiwert TY, et al:
Gefitinib response of erlotinib-refractory lung cancer involving
meninges - role of EGFR mutation. Nat Clin Pract Oncol. 3:50–57.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jackman DM, Holmes AJ, Lindeman N, et al:
Response and resistance in a non-small-cell lung cancer patient
with an epidermal growth factor receptor mutation and
leptomeningeal metastases treated with high-dose gefitinib. J Clin
Oncol. 24:4517–4520. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Clarke JL, Pao W, Wu N, Miller VA and
Lassman AB: High dose weekly erlotinib achieves therapeutic
concentrations in CSF and is effective in leptomeningeal metastases
from epidermal growth factor receptor mutant lung cancer. J
Neurooncol. 99:283–286. 2010. View Article : Google Scholar
|