Introduction
Splenic tumors are relatively rare and difficult to
diagnose prior to surgery. Splenic neoplasms include hemangioma,
lymphangioma, hamartoma, hemangiosarcoma, malignant lymphoma and
metastatic carcinoma. Inflammatory pseudotumors of the spleen
(IPTSs) are extremely rare and frequently misdiagnosed as malignant
or as other tumors prior to surgery (1,2). IPTSs
are benign entities of unknown etiology and pathogenesis that have
been described in only a few cases in the literature (3). The present study reports a new case
and reviews the clinicopathological features, diagnosis, treatment
and prognosis of the previously reported cases of IPTS. Informed
consent was obtained from the patient’s family.
Case report
A 72-year-old male was admitted to the Department of
General Surgery at the Second Affiliated Hospital of Dalian Medical
University (Dailan, China) due to a tumor of the spleen that had
been identified incidentally 1 year previously and which had grown
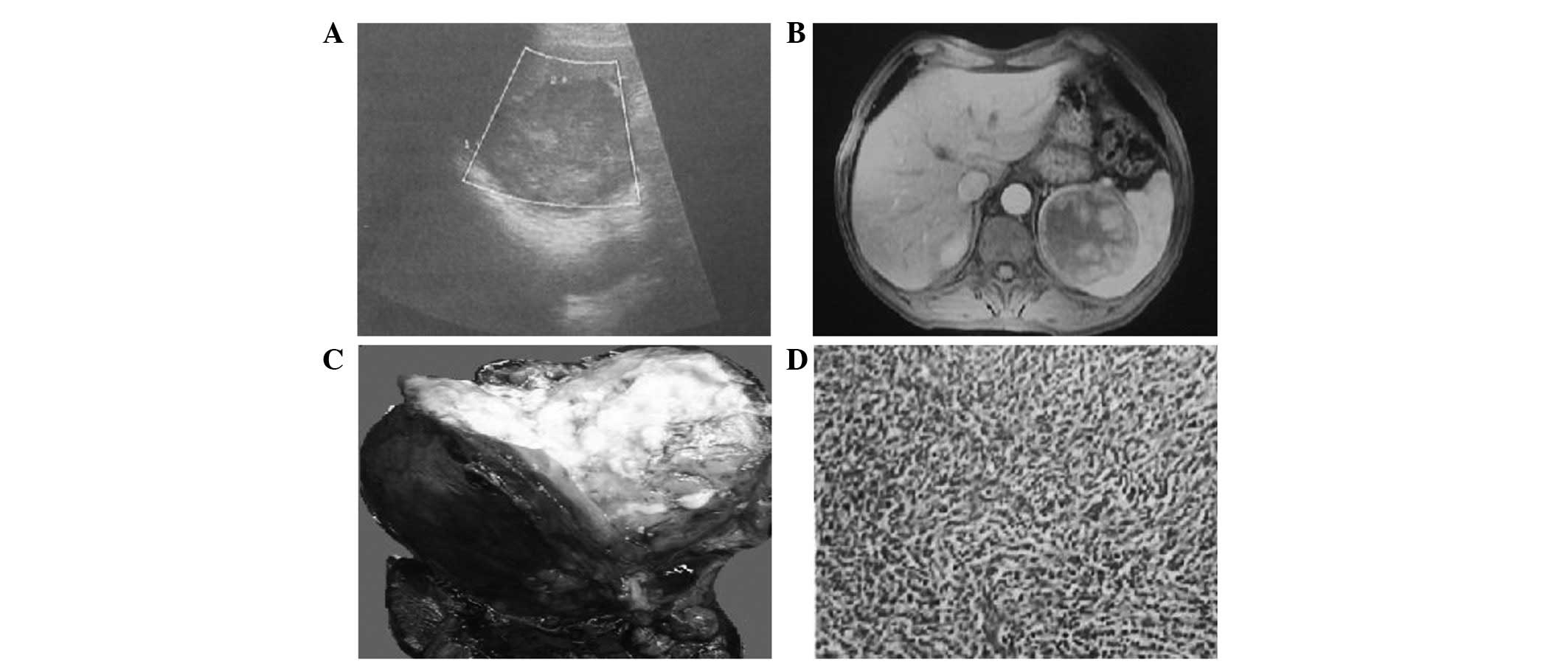
in diameter over a 15-day period prior to the admittance. The
splenic mass was detected in a routine ultrasound scan 1 year prior
to admittance. At the time of identification, the diameter was 5.5
cm (Fig. 1A), while at the time of
admittance, 1 year later, the diameter was 7.7 cm. The patient
remained asymptomatic. A physical examination revealed that the
patient had no fever, or abdominal pain and distension. The
patient’s abdomen was flat, with no tenderness. The biochemical and
hematological investigations were all within the normal ranges.
Magnetic resonance imaging (MRI; Fig.
1B) and computed tomography (CT) scans of the abdomen were
performed and confirmed the presence of a mass within the spleen
demonstrating diffuse heterogeneous enhancement. The tumor was
suspected to be a splenic lymphoma or another type of malignant
tumor. Consequently, the decision was made to proceed with surgery
and the patient underwent a splenectomy.
On entering the abdominal cavity, the splenic tumor
was visible and occupied the majority of the spleen, therefore, the
patient underwent a splenectomy. The resected spleen weighed 385 g
and the tumor size was 7.8×6.5×5.5 cm. When the spleen was placed
into a pan, it was noted that the tumor was circumscribed, but not
encapsulated, and contained a large amount of tan-white, necrotic
tissue in the center (Fig. 1C).
On histological examination, a large,
irregularly-shaped necrotic focus was observed in the center, with
a marked area of inflammatory infiltration. This was composed of an
admixture of inflammatory cellular elements, predominantly plasma
cells and lymphocytes with hyalinization, fibrosis, lymph follicles
and multinuclear giant cells (Fig.
1D). The final pathological diagnosis was of IPTS.
The patient thus far remains alive and asymptomatic
at 4 months subsequent to surgery.
Discussion
Inflammatory pseudotumors occur in a variety of
organs and locations, including the orbit of the eye, the
respiratory tract, the gastrointestinal tract and the liver.
However, IPTSs are extremely rare lesions that are usually located
incidentally (1,4). The incidence of benign splenic tumors
is 0.007% among all subjects on whom surgeries or autopsies are
performed. Consequently, the incidence of IPTS is much lower than
this (5). To the best of our
knowledge, since Cotelingam and Jaffe (6) first reported 2 cases of IPTS in 1984,
only 114 cases, including the present case, have been reported in
the literature.
Based on these studies, it appears that IPTS usually
affects middle- and advanced-aged adults. Only 4 cases have been
reported in children (7–10). However, there is controversy
(11) over the association between
IPTS and gender. The majority of studies have suggested that women
are more frequently affected (12).
A review of the 114 reported cases of IPTS was performed, which
showed that there were 48 cases that listed the gender of the
patients. Among these cases there were 18 males and 30 females,
with a 5:3 female predominance. The patients ranged in age from 6
to 81 years, with a median age of 47.2 years.
The pathogenesis of IPTS is a topic of debate and
several possible causes have been reported. Bacterial infection,
neoplastic processes, vascular causes and immunological derangement
have all been proposed as factors. Certain cases have been reported
to be Epstein-Barr virus-positive inflammatory pseudotumors.
However, the real pathogenesis remains unknown (1,13–16).
IPTSs often present diagnostic difficulties, since
they lack characteristic clinical manifestations and the symptoms
are extremely diverse. The majority of lesions (n=76, 66.7%) were
detected incidentally during routine physical check-ups or elective
abdominal imaging studies. Among the patients exhibiting symptoms,
upper abdominal pain or discomfort (n=23, 60.5%, 23/38) was the
predominant symptom. Fever and splenomegaly were also present in
certain cases (17).
When a lesion occurs as a primary splenic tumor,
lymphoma is usually clinically suspected (18), as occurred in the present patient.
The laboratory data of a number cases showed no evidence of any
abnormalities. Although imaging examinations have improved
significantly in the past 2 decades, they have been unable to
provide conclusive results. Only pathological and
immunohistochemical studies following splenectomy have enabled any
definitive diagnoses.
Ultrasound, MRI and CT scans are able to provide a
certain amount of evidence for diagnosis. However, these findings
are not specific enough to differentiate this type of lesion from
other neoplasms. Ultrasonography may reveal a partially calcified,
well-defined echogenic mass or hypoechoic discrete lesion,
consistent with the findings in the present case. CT scans usually
show a low-density mass in the non-enhanced and enhanced modes. MRI
may reveal a well-defined mass in a superior manner to a CT scan,
which is reported to be isointense on T1-weighted images, and with
either an increased or decreased signal intensity on T2-weighted
images, with respect to the surrounding normal spleen (1,2,19).
Performing a core biopsy is a useful method for
diagnosing hematological and non-hematological splenic lesions that
may be used to distinguish IPTSs from other lesions in its
differential diagnosis (16,20).
However, a core biopsy is not recommended for splenic masses due to
the uncertainty of detecting the disease, the risk of metastases if
the mass is a malignant neoplasm and the potential hemorrhagic
complications of the procedure. Therefore, a histological
examination of the resected specimens is the gold standard for
diagnosing tumors of the spleen.
The typical macroscopic appearance of an IPTS lesion
is that of a well-circumscribed, non-encapsulated mass with a large
amount of tan-white, necrotic tissue in the center. The cellular
composition of IPTSs may be remarkably heterogeneous. The IPTS mass
may resemble granulation tissue, while normal lymphocytes and
plasma cells are constant features, although variable in mixture
and number. Neutrophilic and eosinophilic leukocytes are also
present in certain cases. This may raise the possiblity of a
lymphoreticular malignancy, thus requiring immunohistological
studies for a definitive diagnosis in certain cases (14).
When an IPTS is identified, it must first be
differentiated from lymphatic neoplasma, particularly malignant
lymphoma. A diagnosis of malignant lymphoma was initially made in a
number of the IPTS cases reported in the literature, as occurred in
the present case prior to surgery. The differential diagnosis for
IPTS also considers other lesions, including hamartomas,
hemangiomas, hemangioendotheliomas, angiosarcomas, infectious
granulomatous processes and sarcoidosis (4–7,11–15,21,22).
As an IPTS lesion is benign without the risk of
malignant transformation, the question arises whether an
asymptomatic patient with IPTS should undergo a surgical procedure
if the lesion is detected incidentally. At present there is no
sensitive and specific method for diagnosing IPTS without a tissue
sample, and since certain lesions that resemble IPTS are malignant
in nature, we propose that it is prudent to operate even if IPTS is
suspected. If the lesion is not too large, a splenectomy is
unnecessary and partial splenic resection, using laparoscopic or
open surgery, is a relatively suitable surgical approach. Recently,
there have been several studies concerned with the use of
laparoscopic spleen surgery for IPTS (23–25).
According to the previously published cases, the
prognosis of IPTS has generally been considered to be favorable
following splenectomy, although there is minimal data available on
the follow-up of these patients. There have been no reports of
metastatic disease, local invasion or recurrence. However, careful
follow-up is necessary, since certain patients with inflammatory
pseudotumors of the liver have been reported to have succumbed to
the disease (1,26,27).
To conclude, IPTS is an extremely rare condition. To
the best of our knowledge, only 114 cases have been reported in the
literature, including the present case. Establishing a
pre-operative diagnosis of IPTS is often difficult and since
certain lesions that resemble IPTS are malignant in nature, we
suggest that it is prudent to operate even if IPTS is suspected.
Only splenectomy and histopathological study of the specimen enable
a definitive diagnosis and the consequent treatment of this
disease, therefore splenectomy is diagnostic and curative. The
prognosis of IPTS has generally been considered to be favorable
following splenectomy.
References
|
1
|
Yan J, Peng C, Yang W, Wu C, Ding J, Shi T
and Li H: Inflammatory pseudotumour of the spleen: report of 2
cases and literature review. Can J Surg. 51:75–76. 2008.PubMed/NCBI
|
|
2
|
Yano H, Imasato M, Monden T and Okamoto S:
Inflammatory pseudotumor of the spleen: report of two cases.
Surgery. 133:349–350. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Oz Puyan F, Bilgi S, Unlu E, Yalcin O,
Altaner S, Demir M and Cakir B: Inflammatory pseudotumor of the
spleen with EBV positivity: report of a case. Eur J Haematol.
72:285–291. 2004.PubMed/NCBI
|
|
4
|
Oshiro H, Nomura M, Yamanaka S, Watanabe S
and Inayama Y: Splenic inflammatory pseudotumor (inflammatory
myofibroblastic tumor). J Clin Exp Hematop. 47:83–88. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Natsugoe S, Ohwaki T, Tsubouti H, Mitsuda
K, Maenohara S, Takao S, Aikou T, Shimazu H and Hasui K:
Inflammatory pseudotumor of the spleen: report of a case. Surg
Today. 23:246–250. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cotelingam JD and Jaffe ES: Inflammatory
pseudotumor of the spleen. Am J Surg Pathol. 8:375–380. 1984.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yesildag E, Sarimurat N, Ince U, Numan F
and Buyukunal C: Nonsurgical diagnosis and management of an
inflammatory pseudotumor of the spleen in a child. J Clin
Ultrasound. 31:335–338. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sarker A, An C, Davis M, Praprotnik D,
McCarthy LJ and Orazi A: Inflammatory pseudotumor of the spleen in
a 6-year-old child: a clinicopathologic study. Arch Pathol Lab Med.
127:e127–e130. 2003.PubMed/NCBI
|
|
9
|
Aru GM, Abramowsky CR and Ricketts RR:
Inflammatory pseudotumor of the spleen in a young child. Pediatr
Surg Int. 12:299–301. 1997.PubMed/NCBI
|
|
10
|
Yeung E, Hugh TB and Rainer S:
Inflammatory pseudotumour of the spleen. Aust N Z J Surg.
66:492–493. 1996. View Article : Google Scholar
|
|
11
|
Inada T, Yano T, Shima S, Ishikawa Y, Irie
S, Ishida M, Nakamura Y, Ishibashi K and Kageyama H: Inflammatory
pseudotumor of the spleen. Intern Med. 31:941–945. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wiernik PH, Rader M, Becker NH and Morris
SF: Inflammatory pseudotumor of spleen. Cancer. 66:597–600. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Matsubayashi H, Mizoue T, Mizuguchi Y,
Shinohara Y, Magami Y, Horibe T, Seki T, Saito T and Serizawa H: A
case of hemangioma accompanied by inflammatory pseudotumor of the
spleen. J Clin Gastroenterol. 31:258–261. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Thomas RM, Jaffe ES, Zarate-Osorno A and
Medeiros LJ: Inflammatory pseudotumor of the spleen: a
clinicopathologic and immunophenotypic study of eight cases. Arch
Pathol Lab Med. 117:921–926. 1993.PubMed/NCBI
|
|
15
|
Falk GA, Nooli NP, Morris-Stiff G, Plesec
TP and Rosenblatt S: Sclerosing Angiomatoid Nodular Transformation
(SANT) of the spleen: Case report and review of the literature. Int
J Surg Case Rep. 3:492–500. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rosenbaum L, Fekrazad MH, Rabinowitz I and
Vasef MA: Epstein-Barr virus-associated inflammatory pseudotumor of
the spleen: report of two cases and review of the literature. J
Hematop. 2:127–131. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Neuhauser TS, Derringer GA, Thompson LD,
Fanburg-Smith JC, Aguilera NS, Andriko J, Chu WS and Abbondanzo SL:
Splenic inflammatory myofibroblastic tumor (inflammatory
pseudotumor): a clinicopathologic and immunophenotypic study of 12
cases. Arch Pathol Lab Med. 125:379–385. 2001.PubMed/NCBI
|
|
18
|
Takamoto K, Midorikawa Y, Minagawa M and
Makuuchi M: Inflammatory pseudotumor of the spleen: clinical impact
in surgical treatment. Biosci Trends. 1:113–116. 2007.PubMed/NCBI
|
|
19
|
Okura N, Mori K, Morishita Y, Oda T, Tanoi
T and Minami M: Inflammatory pseudotumor of the intrapancreatic
accessory spleen: computed tomography and magnetic resonance
imaging findings. Jpn J Radiol. 30:171–175. 2012. View Article : Google Scholar
|
|
20
|
Kawaguchi T, Mochizuki K, Kizu T, Miyazaki
M, Yakushijin T, Tsutsui T, Morii E and Takehara T: Inlammatory
pseudotumor of the liver and spleen diagnosed by percutaneous
needle biopsy. World J Gastroenterol. 18:90–95. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hsu CW, Lin CH, Yang TL and Chang HT:
Splenic inlammatory pseudotumor mimicking angiosarcoma. World J
Gastroenterol. 14:6421–6424. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Galindo Gallego M, Ortega Serrano MP,
Ortega Lopez M, Esteban Collazo F and Guinea Esquerdo L:
Inflammatory pseudotumor of spleen. Report of two cases and
literature review. Minerva Chir. 52:1379–1388. 1997.PubMed/NCBI
|
|
23
|
Suzumura K, Okada T, Satake M and Fujimito
J: Laparoscopic splenectomy for inflammatory pseudotumor of the
spleen. Hepatogastroenterology. 58:1909–1911. 2011.PubMed/NCBI
|
|
24
|
Shapiro AJ and Adams ED: Inflammatory
pseudotumor of the spleen managed laparoscopically. Can
preoperative imaging establish the diagnosis? Case report and
literature review. Surg Laparosc Endosc Percutan Tech. 16:357–361.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Uchida H, Ohta M, Shibata K, Endo Y, Iwaki
K, Tominaga M, Ishio T and Kitano S: Laparoscopic splenectomy in
patients with inflammatory pseudotumor of the spleen: Report of 2
cases and review of the literature. Surg Laparosc Endosc Percutan
Tech. 16:182–186. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Horiuchi R, Uchida T, Kojima T and Shikata
T: Inflammatory pseudotumor of the liver. Clinicopathologic study
and review of the literature. Cancer. 65:1583–1590. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tsutsumi N, Kawanaka H, Yamaguchi S, Sakai
M, Momosaki S, Endo K and Ikejiri K: Huge inflammatory pseudotumor
of the spleen with postoperative portal vein thrombosis: report of
a case. Surg Today. 42:382–385. 2012. View Article : Google Scholar : PubMed/NCBI
|