Introduction
The admixture of neoplastic endocrine and
non-endocrine cells have been identified infrequently in gastric
tumors. For such lesions, four distinct categories are
distinguished according to the tissue morphological features:
carcinomas with interspersed endocrine cells, carcinoids with
interspersed non-endocrine cells, mixed tumors and amphicrine
tumors. Mixed tumors may be further classified into composite
tumors, which exhibit an admixture of two histological components
with histological transitions, and collision tumors, where the two
components are not intermixed (1).
While carcinoma with interspersed endocrine cells is the most
frequent, the remaining tumors have rarely been reported in the
stomach, with collision tumor being particularly unusual (1).
In the present study, we report a case with features
of adenocarcinoma colliding with a typical carcinoid component,
along with a review of the literature. The study was approved by
the Ethics Committee of Akdeniz Unversity Medical Faculty, Antalya,
Turkey. Written informed consent was obtained from the patient.
Case report
A 51-year-old female was admitted to the Department
of Internal Medicine of Akdeniz University Medical School, Antalya,
Turkey, with complaints of epigastric pain. On physical examination
there was significant epigastric tenderness. The biochemical
analyses of blood and urine were within normal ranges. While the
CEA level was not elevated, the CA19-9 level was higher than the
normal titer value (82 U/ml; reference range, 0–40 U/ml). An upper
gastrointestinal endoscopy showed an ulcerated polypoid mass
located on the cardia. The histopathological examination of
multiple biopsies from this lesion revealed a gastric
adenocarcinoma. The patient underwent a total gastrectomy with
lymph node dissection.
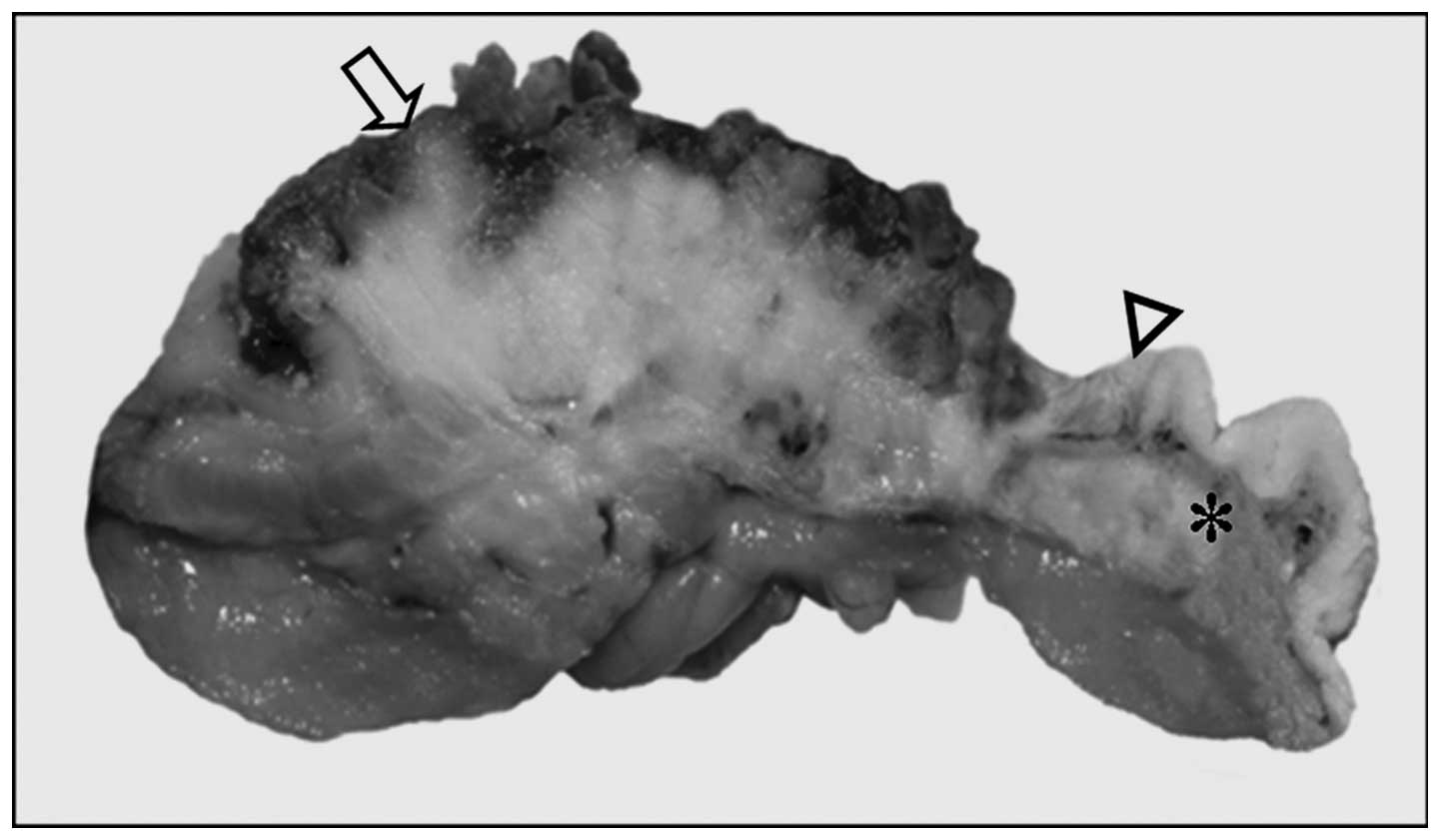
Macroscopic examination revealed an ulcerated
polypoid mass measuring 2.5×1.5×2 cm. The dissected surface showed
a yellow-white area surrounding the area of the ulcer. On closer
inspection, a more yellow region (1 cm) was observed below the
normal location of the gastric mucosal folds. This region and the
ulcerated yellow area were abutted to each other (Fig. 1).
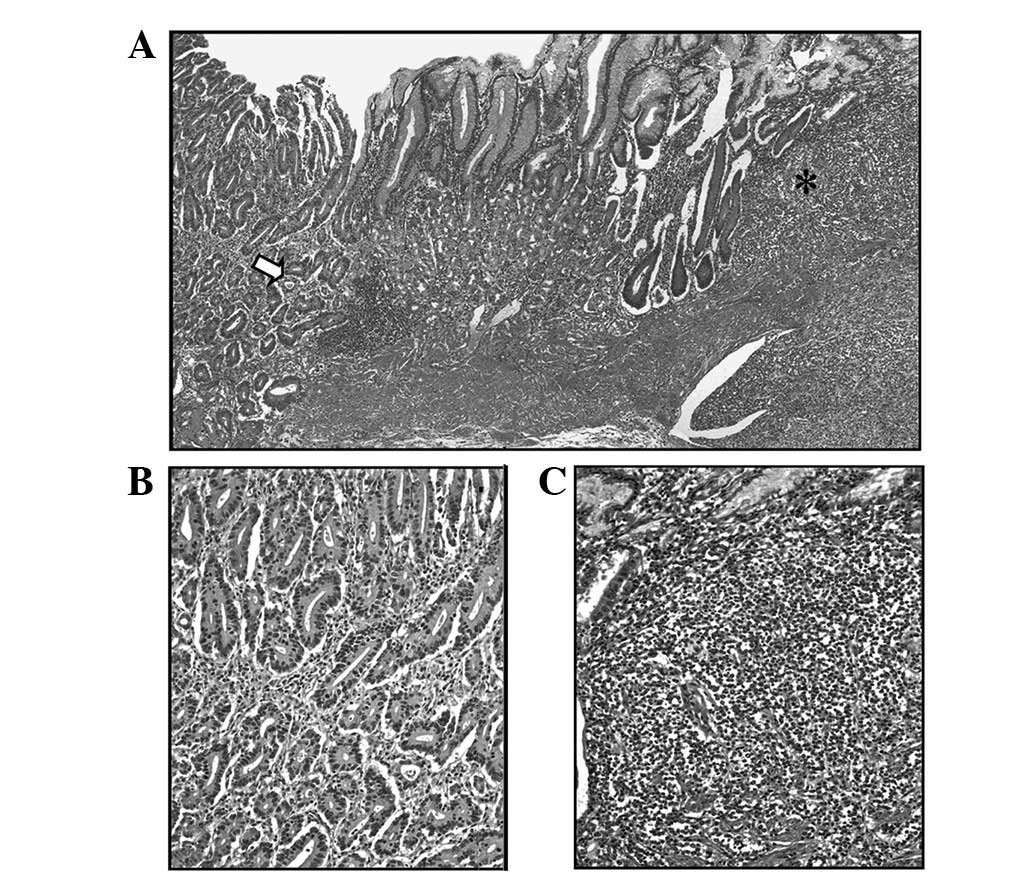
Microscopically, hematoxylin and eosin-stained
tissue sections from two different areas of the mass showed two
different types of tumor. One was a moderately differentiated
intestinal type adenocarcinoma and the other was a tumor composed
of a relatively uniform population of small cells with organoid,
trabecular or focally solid patterns, suggesting neuroendocrine
cell proliferation (Fig. 2). These
cells exhibited a granular cytoplasm and an indistinct cytoplasmic
border. Their nuclei had homogenous chromatin with indistinct
nucleoli. Mitosis was infrequent (1/10 hpf) and necrosis was not
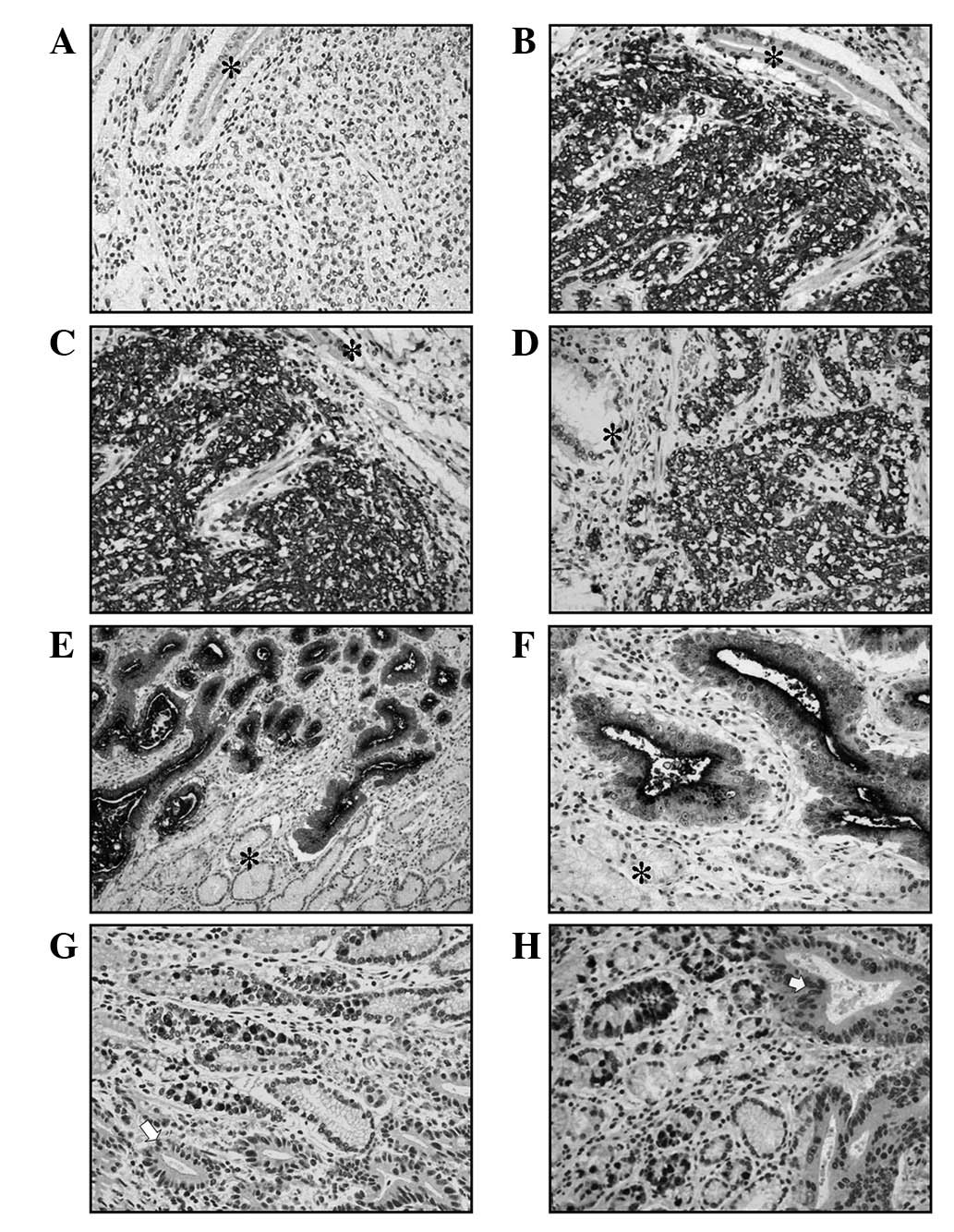
observed. Immunohistochemical analysis showed that these cells had
strong positivity for neuroendocrine markers (synaptophysin,
chromogranin A and NSE) and this section of the tumor was diagnosed
as a typical carcinoid tumor (Fig.
3). By contrast, adenocarcinoma cells expressed only CEA
(Fig. 3). As the two tumors were
distinctly separated from each other and no merging of tissue
components was noted at the interface of the growth, the final
diagnosis was a collision tumor composed of an adenocarcinoma and a
carcinoid tumor of the stomach. The two tumors invaded the
subserosal layer. While lymphatic permeation by the adenocarcinoma
was noted, the carcinoid component was negative for lymphatic
permeation. Vascular invasion was not observed for either
component. Metastasis of the adenocarcinoma was identified in 7
perigastric lymph nodes among the 12 dissected lymph nodes, while
metastasis of the carcinoid tumor was not detected.
Clinical course
The patient succumbed to the tumor progression five
months after surgery.
Discussion
The present case involved a 51-year-old female with
an ulcerated polypoid mass located at the cardiac region of the
stomach. According to the pathological and immunohistochemical
findings, the mass was diagnosed as a collision tumor comprising an
adenocarcinoma and a carcinoid tumor. Although the presence of
adenocarcinoma or carcinoid tumor individually is not notable, this
collision tumor with two histopathological types in the stomach is
only the eleventh case in the current literature. The patient in
the present case report is younger than those reported in previous
cases (mean, 61.7 years) and contrasts the frequent male
predilection for this type of lesion (male/female, 4:1),
demonstrating that collision tumors of this type are not only
limited to older age groups or to males (Table I) (2–11).
 | Table I.Summary of previous studies on gastric
collision tumor composed of an adenocarcinoma and a carcinoid
tumor. |
Table I.
Summary of previous studies on gastric
collision tumor composed of an adenocarcinoma and a carcinoid
tumor.
| Authors (Ref.) | Age (years) | Gender | Location |
|---|
| Yamashina M et
al (11) | 50 | Male | Corpus |
| Chodankar CM et
al (10) | 69 | Female | Corpus |
| Morishita Y et
al (9) | 49 | Male | Corpus |
| Corsi A et al
(8) | 72 | Male | Unknown |
| Camuñas Mohinelo FA
et al (7) | 66 | Male | Cardia |
| Olinici CD et
al (6) | 68 | Male | Corpus |
| Morishita Y et
al (5) | 84 | Female | Cardia |
| Jayaraman A et
al (4) | 48 | Male | Antrum |
| Doggui MH et
al (3) | 55 | Male | Fundus |
| Mróz A et al
(2) | 56 | Male | Corpus |
| Present case | 51 | Female | Cardia |
As shown in the present case, gastric collision
tumors comprising an adenocarcinoma and a carcinoid tumor are
usually solitary lesions (2,4–11).
The majority of previously reported tumors were located in the
corpus (2,6,9–11).
However, two previous cases were localized at the cardia (similar
to the present case); one case was identified in the antrum and
another in the fundus, suggesting that this tumor type may be
encountered in different locations in the stomach (Table I) (3–5,7).
In general it is difficult to morphologically
distinguish a collision tumor from a composite tumor. However, in
the present case, the tumor comprised two components with different
histopathological and immunohistochemical features. The two
constituents were abutting each other without histological
transition between them. Although metastasis of a composite tumor
comprises both of the tissue components, metastasis of a collision
tumor includes only a single tissue component (1). In our case report, lymph node
metastases were monomorphic and had an adenocarcinoma component.
Another problem in the correct diagnosis of collision tumors
comprising an adenocarcinoma and a carcinoid tumor is that a
diagnosis based on endoscopic biopsy may depend on the sampled site
of the tumor. In these cases, if the biopsy specimen revealed only
the carcinoid component, treatment and surgical intervention may be
different.
Although pathogenic factors that contribute to the
development of an adenocarcinoma or a carcinoid tumor alone have
been extensively described, the pathogenesis of collision tumors
comprising adenocarcinoma and carcinoid tumor is unclear. For
instance, diet, genetics and infection with Helicobacter
pylori may contribute to the development of gastric
adenocarcinoma. Pernicious anemia and gastric atrophy may be a
contributing factor for the development of a gastric carcinoid
tumor (5). Alternatively, it has
been postulated that carcinoid tumors are able to produce
substances with a growth-promoting effect, which may account for
the occurrence of a secondary tumor in the vicinity (12). In the present case, pernicious
anemia and atrophic gastritis were not observed and the fasting
serum gastrin value was not elevated. These tumors are considered
to have arisen independently from multipotential epithelial stem
cells and primitive neuroendocrine cells. In a previous report
which carried out allelotyping analysis to study the genetic
profiles of the endocrine and exocrine components of six mixed
tumors of the gut, Furlan et al observed clonal divergence
in a collision tumor, which was composed of a well-differentiated
endocrine carcinoma associated with an adenocarcinoma (13). This finding confirms the existence
of double tumors which grow next to each other coincidentally, yet
exhibit different histogenesis and different tumorigenetic
pathways.
The prognosis of this rare entity is unclear;
however, from the few known cases it appears that the
adenocarcinoma impacts more heavily on prognosis (1,5). The
patient in this case succumbed to the tumor five months after
gastric resection due to widespread liver metastasis of the
adenocarcinoma.
In conclusion, the present case is the eleventh
gastric collision tumor of its type, composed of an adenocarcinoma
and a carcinoid tumor and this confirms their presence at this
location. As further cases of this tumor type are reported, the
clinicopathological properties and pathogenesis of this entity are
likely to be revealed in more detail.
Acknowledgements
This study was supported by Akdeniz
University Scientific Projects Unit.
References
|
1.
|
Graeme-Cook F: Neuroendocrine tumors of
the GI tract and appendix. Surgical Pathology of the GI Tract,
Liver, Biliary tract, and Pancreas. Odze RD, Goldblum JR and
Crawford JM: 1st edition. WB Saunders; Philadelphia, PA: pp.
491–496. 2004
|
|
2.
|
Mróz A, Kiedrowski M, Malinowska M and
Sopyło R: Collision tumour of the stomach - adenocarcinoma and
neuroendocrine carcinoma: case report and review of the literature.
Pol J Pathol. 60:94–97. 2009.PubMed/NCBI
|
|
3.
|
Doggui MH, Ben Yaghlène L, Hefaiedh R,
Bouguassas W, Mestiri A and Dellagi K: A gastric collision tumor
composed of adenocarcinoma and gastrinoma: case report. Tunis Med.
86:755–757. 2008.PubMed/NCBI
|
|
4.
|
Jayaraman A, Ramesh S, Jeyasingh R and
Bagyalakshmi KR: Gastric collision tumour - a case report. Indian J
Pathol Microbiol. 48:264–265. 2005.
|
|
5.
|
Morishita Y, Sugitani M, Sheikh A, Nemoto
N, Fujii M and Takayama T: Collision tumor of the stomach: a rare
case of an adenocarcinoma and carcinoid tumor. Arch Pathol Lab Med.
129:407–409. 2005.PubMed/NCBI
|
|
6.
|
Olinici CD, Crişan D and Racu I:
Synchronous gastric adenocarcinoma and carcinoid. Rom J
Gastroenterol. 13:135–137. 2004.PubMed/NCBI
|
|
7.
|
Camuñas Mohinelo, FA Melgar, Requena P,
Martínez Zaragoza J, et al: Gastric collision tumor with osseous
metaplasia. Rev Esp Enferm Dig. 89:317–319. 1997.(In Spanish).
|
|
8.
|
Corsi A and Bosman C: Adenocarcinoma and
atypical carcinoid: morphological study of a gastric collision-type
tumour in the carcinoma-carcinoid spectrum. Ital J Gastroenterol.
27:303–308. 1995.PubMed/NCBI
|
|
9.
|
Morishita Y, Tanaka T, Kato K, et al:
Gastric collision tumor (carcinoid and adenocarcinoma) with
gastritis cystica profunda. Arch Pathol Lab Med. 115:1006–1010.
1991.PubMed/NCBI
|
|
10.
|
Chodankar CM, Pandit SP, Motiwale SS and
Deodhar KP: Collision tumour of stomach. Indian J Gastroenterol.
8:297–298. 1989.
|
|
11.
|
Yamashina M and Flinner RA: Concurrent
occurrence of adenocarcinoma and carcinoid tumor of the stomach: a
composite tumor or collision tumors? Am J Clin Pathol. 83:233–236.
1985.PubMed/NCBI
|
|
12.
|
Gerstle JT, Kauffman GL and Koltun WA: The
incidence, management, and outcome of patients with
gastrointestinal carcinoids and second primary malignancies. J Am
Coll Surg. 180:427–432. 1995.PubMed/NCBI
|
|
13.
|
Furlan D, Cerutti R, Genasetti A, et al:
Microallelotyping defines the monoclonal or the polyclonal origin
of mixed and collision endocrine-exocrine tumors of the gut. Lab
Invest. 83:963–971. 2003. View Article : Google Scholar : PubMed/NCBI
|