Introduction
Malignant melanoma occasionally exhibits a variety
of cytomorphological and architectural features and includes the
balloon cell, rhabdoid, small cell, signet-ring cell, myxoid and
adenoid (pseudoglandular) types (1). Although rare, rosette formation has
previously been documented in malignant melanoma and Spitz nevus
(1–5). The present study describes the second
documented case of malignant melanoma with perivascular
pseudorosettes and provides a review of the clinicopathological
features of malignant melanoma with rosette formation. Written
informed consent was obtained from the patient.
Patient and methods
Case Report
A 38-year-old male with no past history of malignant
melanoma presented with a gradually enlarging nodule on his back. A
physical examination revealed that the nodule was black and
measured 35×30 mm in diameter. The left axillary lymph nodes were
enlarged. Computed tomography demonstrated multiple nodules in the
liver, which were clinically suspected to be metastatic lesions. A
total resection of the back nodule and the left axillary lymph
nodes was performed.
Materials
The formalin-fixed, paraffin-embedded tissue blocks
of the resected skin specimen and lymph nodes were cut into 3-μm
thick sections, deparaffinized and rehydrated. Each section was
stained with hematoxylin and eosin and used for immunostaining. The
immunohistochemical analyses were performed using an autostainer
(XT system Benchmark; Ventana Medical System, Tucson, AZ, USA)
according to the manufacturer’s instructions. The following primary
antibodies were used: A mouse monoclonal antibody against CD56
(CD564; Novocastra Laboratories, Ltd., Newcastle upon Tyne, UK), a
mouse monoclonal antibody against chromogranin A (DAK-A3; DAKO
Cytomation, Glostrup, Denmark), a mouse monoclonal antibody against
glial fibrillary acid protein (GFAP; 6F2; DAKO), a mouse monoclonal
antibody against HMB-45 (HMB-45; Novocastra), a mouse monoclonal
antibody against Melan-A (A103; Novocastra), a rabbit polyclonal
antibody against S-100 protein (Nichirei Bioscience, Tokyo, Japan)
and a mouse monoclonal antibody against synaptophysin (27G12;
Novocastra).
Results
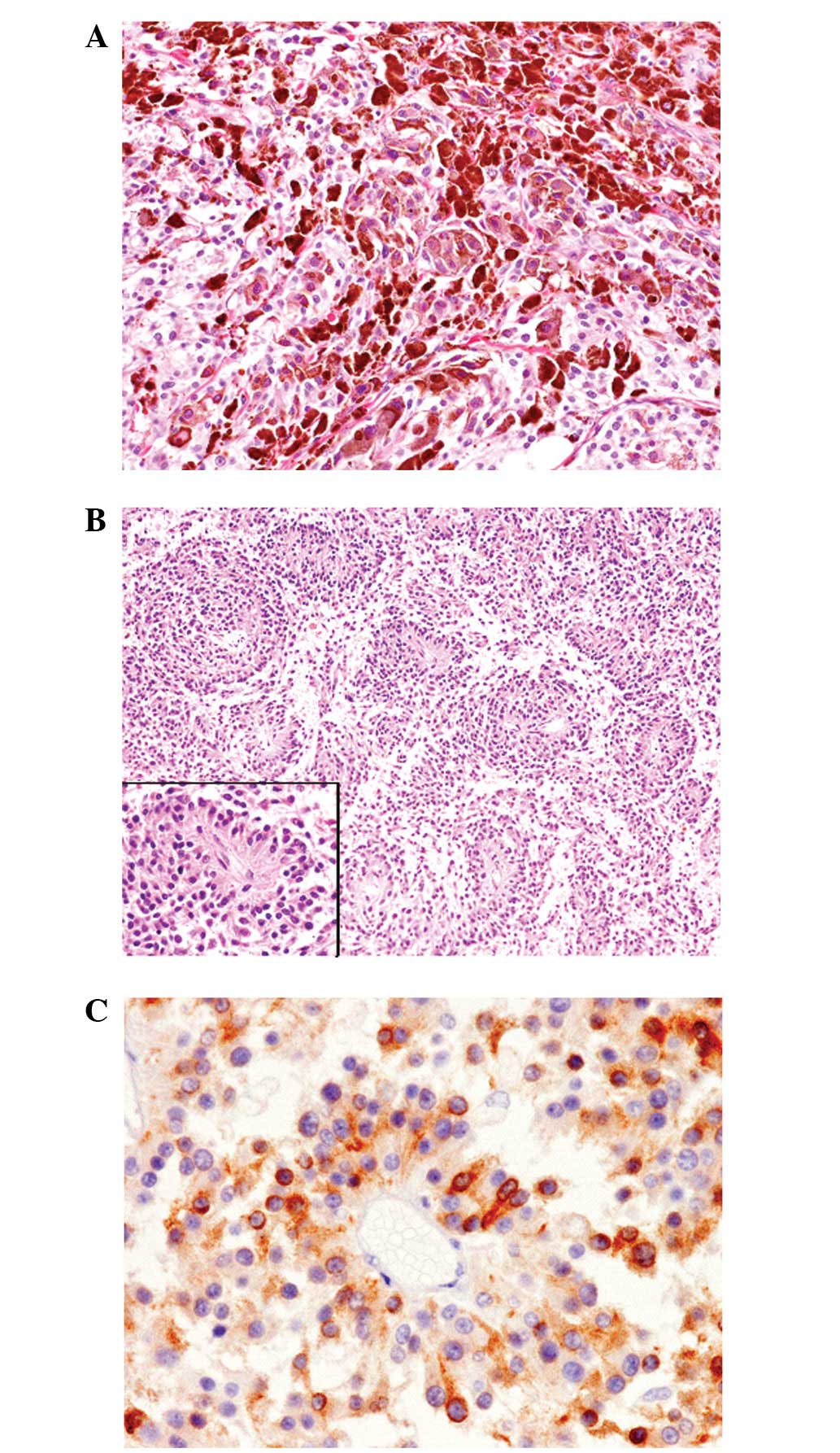
The histopathological study of the resected back
nodule revealed a diffuse proliferation of neoplastic cells
accompanied by scattered geographical necrotic foci from the entire
dermis to the subcutis. The upper section of the lesion (~30% of
the tumor) was composed of a conventional malignant melanoma
component. The section was comprised of large polygonal neoplastic
cells that contained large nuclei with or without conspicuous
nucleoli. The majority of these cells contained the melanin pigment
within the cytoplasm (Fig. 1A). The
remaining area of the tumor was composed of medium-sized polygonal
cells with slightly eosinophilic cytoplasm and small-to-medium
round nuclei with or without nucleoli. Melanin pigment was rarely
observed in these neoplastic cells. A noteworthy observation was
the presence of perivascular pseudorosette formations within these
areas (Fig. 1B). These tumor cells
were arranged radially around the blood vessels, with a
perivascular anuclear zone (Fig.
1B, inset). Mitotic figures were scattered in the entire lesion
(17/10 high-power fields).
Immunohistochemical studies revealed that S-100
protein and Melan-A were diffusely expressed in the two components
(Fig. 1C). HMB-45 was diffusely
positive in the conventional component, but focally expressed in
the areas with perivascular pseudorosettes. Synaptophysin,
chromogranin A, CD56, and GFAP were not expressed in the two
components.
The left axillary lymph nodes contained metastatic
malignant melanoma with the two components and their
immunohistochemical characteristics were the same as those of the
back lesion.
According to these findings, a diagnosis of
malignant melanoma with perivascular pseudorosettes accompanied by
lymph node metastases was made.
Discussion
In diagnostic pathology, rosettes are classically
referred to as discrete cell clusters showing peripheral nuclear
palisading and a central space. Although rosettes are commonly
considered to be of neuroepithelial differentiation, they are
occasionally observed in other types of tumors, including
neuroendocrine carcinomas, granulosa cell tumors and thymomas.
Certain histopathological subtypes of rosettes are well known,
including the Homer-Wright type and perivascular pseudorosettes.
Homer-Wright rosettes are characterized by a radial arrangement of
cells with centrally situated fibrillary material and are often
observed in neuroblastomas, medulloblastomas and primitive
neuroectodermal tumors. Perivascular pseudorosettes are composed of
columnar cells arranged radially around the blood vessels, with a
perivascular anuclear zone. This structure is a well-known
characteristic feature of an ependymoma (2–4).
Although rare, rosette formation has been previously
documented in malignant melanomas (1–4).
Table I summarizes the
clinicopathological features of the four previously reported cases
of malignant melanoma with rosette formation, in addition to the
present case. The types of rosettes include the Homer-Wright type
(two cases), perivascular pseudorosettes (two cases) and an
unclassifiable type (one case). Banerjee and Harris described a
case of metastatic small-cell melanoma in the bone marrow that was
accompanied by perivascular pseudorosettes (1), and the present case is the second
documented case of this type. In the two cases, the rosettes were
present at the primary site and at the metastatic lymph nodes. In
the other two cases, the rosettes were observed only at the
metastatic sites. Although the case described by Alonso et
al described melanin pigment within the cytoplasm of the
neoplastic melanocytes forming the Homer-Wright rosette, melanin
pigment was barely observed within the cytoplasm of the
rosette-forming tumor cells in the present case and in the case
reported by Falconieri et al(4). Therefore, differential diagnoses from
other types of rosette-forming tumors, including neuroblastomas and
malignant peripheral nerve sheath tumors, are necessary. However,
Melan-A or HMB-45 are expressed in all cases of malignant melanoma
with rosette formation (Table I).
Therefore, immunohistochemical analyses may facilitate the
achievement of a correct diagnosis.
 | Table IClinicopathological features of
malignant melanoma with rosettes. |
Table I
Clinicopathological features of
malignant melanoma with rosettes.
| First author/s, year
(ref.) | Case no. | Age, years | Gender | Location | Type of rosette |
Immunohistochemistry |
|---|
| Banerjee and Harris,
2002 (1) | 1 | N/A | N/A | Bone marrow | Perivascular | N/A |
| Pföhler et al,
2003(2) | 2 | 29 | Female | Upper arm/lymph
node | Unclassifiable | S-100
protein+, HMB-45+ |
| Alonso et al,
2003 (3) | 3 | 61 | Male | Lymph node | Homer-Wright | S-100
protein+, Melan-A+, chromogranin
A−, synaptophysin−,
neurofilament−, GFAP− |
| Falconieri et
al, 2010 (4) | 4 | 43 | Female | Back | Homer-Wright | S-100
protein+, Melan-A+, HMB-45+ |
| Present Case | - | 38 | Male | Back/lymph node | Perivascular | S-100
protein+, Melan-A+, HMB-45+
(focally), chromogranin A−, synaptophysin−,
neurofilament−, GFAP− |
Although the mechanism of rosette formation in
malignant melanoma remains unclear, it has been speculated that the
neoplastic melanoma cells share the same capabilities for
differentiation as neural crest precursors (4).
In conclusion, the present study describes the
second documented case of a malignant melanoma with perivascular
pseudorosettes. Rosette formation in malignant melanoma is a
distinct histopathological variant and may be an under-recognized
phenomenon. Additional studies are required to clarify the
clinicopathological features of this variant of melanoma, whose
recognition is significant for obtaining an accurate diagnosis of a
malignant melanoma.
References
|
1
|
Banerjee SS and Harris M: Morphological
and immunophenotypic variations in malignant melanoma.
Histopathology. 36:387–402. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pföhler C, Thirkill CE and Tilgen W:
Rosette formation in melanoma: more frequent than suspected? Am J
Dermatopathol. 25:360–361. 2003.PubMed/NCBI
|
|
3
|
Alonso S, Rodriguez-Peralto JL, Ballestin
C and Ortiz P: Metastatic malignant melanoma with Homer-Wright
rosettes mimicking a neuroblastic tumor. An unusual morphological
manifestation. Virchows Arch. 443:108–110. 2003. View Article : Google Scholar
|
|
4
|
Falconieri G, Luzar B, Angione V, DeMaglio
G and Pizzolitto S: Primary cutaneous nevoid melanoma with
Homer-Wright rosettes: a hitherto unrecognized variant with
immunohistochemical and ultrastructural study. Am J Dermatopathol.
32:606–609. 2010. View Article : Google Scholar
|
|
5
|
Miller K, Hall RC and Brenn T: Spitz nevus
with Homer-Wright rosette-like structures. Am J Dermatopathol.
34:457–459. 2012. View Article : Google Scholar : PubMed/NCBI
|