Introduction
Lipoma is the most common mesenchymal neoplasm in
humans and may appear in any location of the body (1). The condition has a peak incidence in
the fifth to seventh decades of life. Ordinary lipoma usually
presents as a soft, slow-growing, painless mass in the subcutaneous
tissue or deep soft tissues (2).
Cytogenetic analysis has revealed identical translocation,
t(3;12)(q27;q13–15), in a subset of lipomas (1). Occasionally, histological subtypes are
recognized by a mixture of other mesenchymal elements that form an
intrinsic part of the tumor. One example of this is an
osteochondrolipoma, which has distinct osseous and cartilaginous
components. The etiology of this condition is unclear. The present
study reports an unusual example of an osteochondrolipoma arising
in the scapular region of a middle-aged male. The differential
diagnosis of this tumor is also discussed. Written informed consent
for this publication was obtained from the patient.
Case study
A 49-year-old male was referred to Fukuoka
University Hospital with a one-month history of a painless,
palpable mass in the left scapular region. There was no history of
antecedent trauma. A physical examination revealed a hard,
non-tender and minimally mobile mass, measuring ~3.0×3.0 cm. The
range of motion of the left shoulder was normal. The neurological
and vascular examinations were unremarkable. The patient's medical
history was non-contributory.
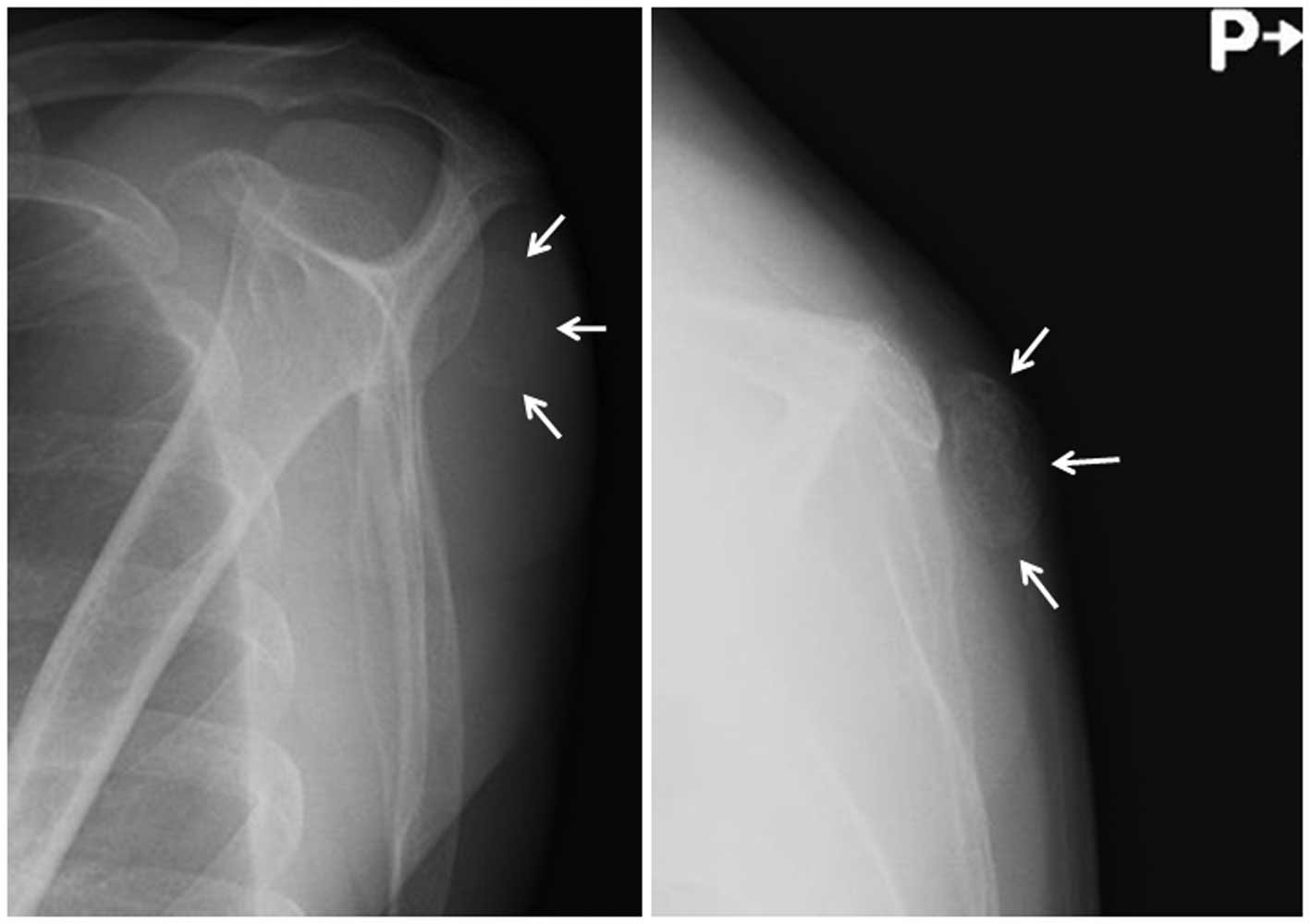
Plain radiographs revealed a faintly ossified,
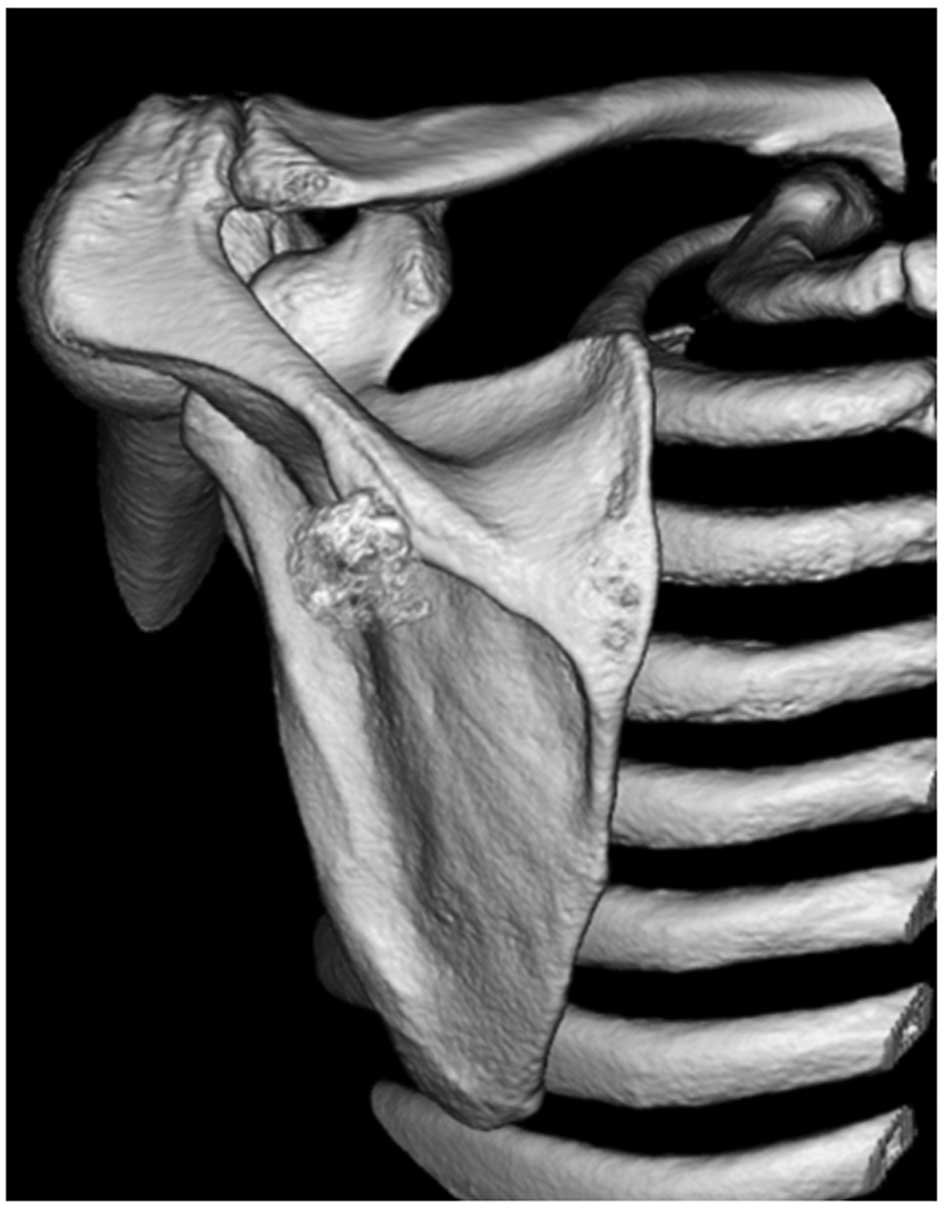
soft-tissue mass without evidence of bone erosion (Fig. 1). Computed tomography (CT)
demonstrated and confirmed an incompletely ossified shell in the
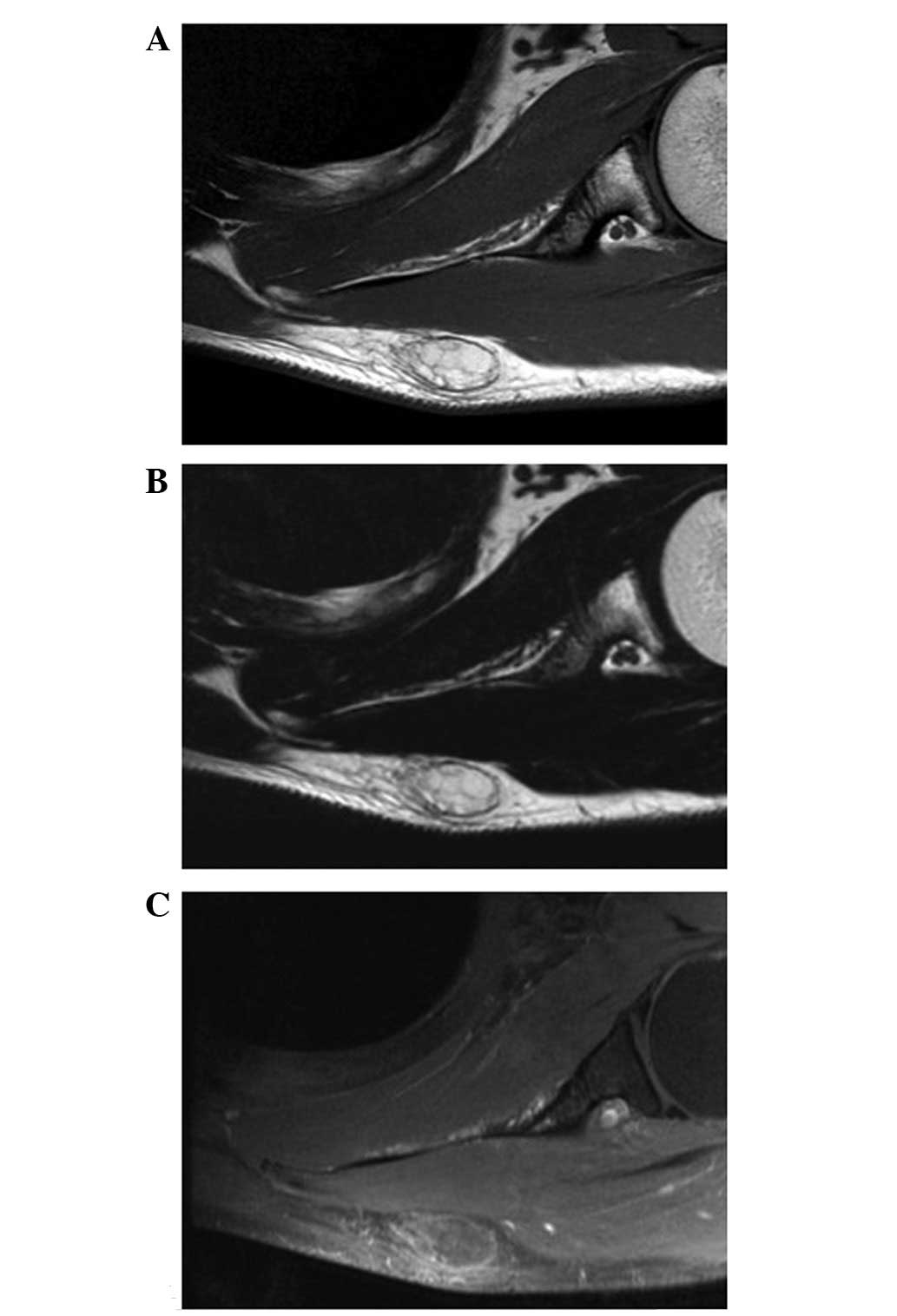
lesion (Fig. 2). Magnetic resonance
imaging (MRI) showed a well-circumscribed subcutaneous mass. The
mass exhibited an almost homogeneous high signal intensity on the
T1- and T2-weighted sequences (Fig. 3A
and B). Contrast-enhanced fat-suppressed T1-weighted sequences
demonstrated a faint peripheral and septal enhancement of the mass
(Fig. 3C). There was no evidence of
bone involvement. A diagnosis of a soft-tissue chondroma,
extraskeletal osteochondroma or a benign soft-tissue tumor, such as
a osteolipoma, was suggested and the lesion was marginally
excised.
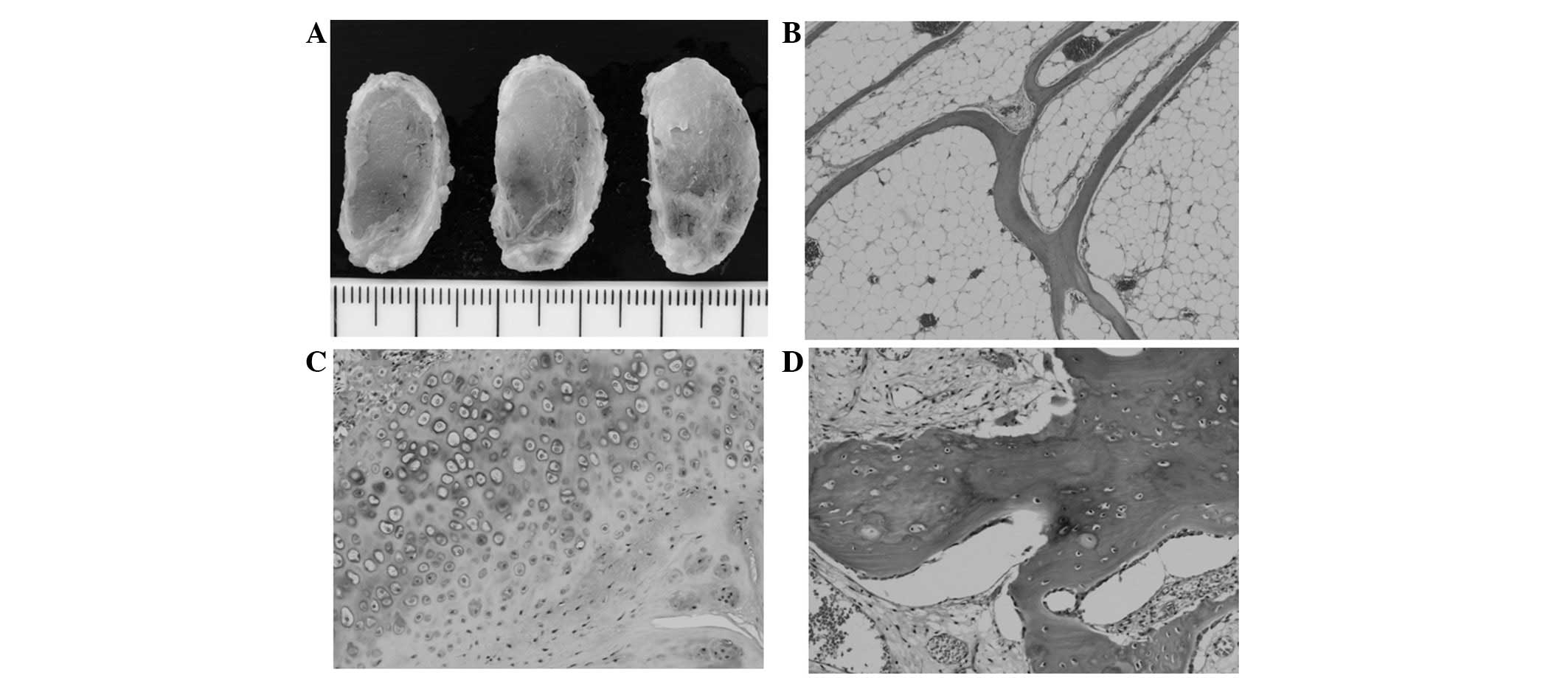
The excised specimen consisted of a
well-circumscribed mass with a smooth surface. The cut sections of
the mass revealed a predominantly yellow, fatty appearance with
small white to gray areas (Fig.
4A). Microscopically, the tumor was predominantly composed of
mature adipocytes mixed with thin trabeculae of mature bone
(Fig. 4B). In addition, small
amounts of mature hyaline cartilage and osteoid were identified in
the periphery of the lesion (Fig. 4C
and D). Cellular atypia or mitotic figures were not observed.
Based on these features, the tumor was diagnosed as an
osteochondrolipoma.
The post-operative course was uneventful. At the
six-month follow-up appointment, the patient was doing well without
evidence of local recurrence.
Discussion
Osteochondrolipoma is one of the less common
histological subtypes of lipoma. The condition may occur at almost
any site of the body, notably in the oral cavity (3). Unlike the mass of the present case,
osteolipomas tend to be large lesions that have been present for a
long period of time (4–6). A marginal excision is curative and
local recurrence is rare. An osteochondrolipoma has the same
prognosis as a simple lipoma. Recently, a reciprocal translocation
t(3;12)(q27;q13–15) has been observed in three cases of osteolipoma
(7), supporting the association
between osteolipomas and simple lipomas.
The pathogenesis of osteochondrolipomas remains
uncertain. Lin et al(8)
reported that mesenchymal stem cells (MSCs) may be identified in
human lipomas and that their characteristics are similar to
adipose-derived MSCs. Therefore, the occurrence of osseous and
cartilaginous differentiation may be a reflection of the presence
of MSCs in certain lipomas. In contrast, certain authors have
proposed a hypothesis that ossification/calcification may be caused
by repetitive trauma or, possibly, ischemia (4,5,7,9).
CT is of great value in the evaluation of
osteochondrolipoma (10). The
procedure is useful for documenting the presence of fatty and
osseous elements. In the current case, CT clearly demonstrated the
presence of surrounding ossification and an association between the
tumor and the adjacent bone. MRI is generally considered to be the
preferred imaging modality for the evaluation of adipocytic tumors.
Simple lipomas have been described as showing homogeneous signal
intensities that are identical to subcutaneous fat on all MR pulse
sequences, with a complete loss of signal following fat suppression
(11). Ossification, calcification
and fibrous connective tissue appear as low signal intensity areas
on all MR pulse sequences (10,12).
In the present case, however, it was difficult to detect and
evaluate the peripheral ossifications using MRI.
The differential diagnosis for osteochondrolipoma
includes soft-tissue chondromas, extraskeletal osteochondromas,
myositis ossificans, ossifying fibromyxoid tumors, chondroid
lipomas and well-differentiated liposarcomas.
Soft-tissue chondromas, also known as extraskeletal
chondromas, are relatively rare, benign cartilaginous tumors that
usually occur in middle-aged adults, with a slight male
predominance (13). These
chondromas typically present as slow-growing, painless nodules or
masses in the hands and feet, particularly in the fingers. MRI
usually reveals a low-intermediate signal intensity on T1-weighted
sequences and an extremely high signal intensity on T2-weighted
sequences (14). Histologically, a
soft-tissue chondroma is composed of mature hyaline cartilage with
variable amounts of fibrosis or myxoid change. An extraskeletal
osteochondroma is a variant of an extraskeletal chondroma that has
undergone extensive enchondral ossification (15,16).
Myositis ossificans is a benign, self-limiting
condition that predominantly affects active adolescents and young
adults, with a slight male predominance. It usually presents as a
rapidly-growing, painful mass that expands for six-eight weeks in
the extremities, particularly in the anterior thigh. Palin
radiographs and CT scans are used to examine this condition and
demonstrate the zoning phenomenon, with a peripheral rim of
ossification that represents mature bone. MRI usually shows an
intermediate signal intensity on T1-weighted sequences and a high
signal intensity on T2-weighted sequences (14,17).
Histologically, myositis ossificans is characterized by a zonal
proliferation of fibroblasts and bone-forming osteoblastic
elements.
Ossifying fibromyxoid tumors, first described by
Enzinger et al in 1989 (18), are rare soft-tissue tumors of
uncertain lineage that usually occur in adults, with a male
predominance. These tumors typically present as slow-growing,
painless, well-circumscribed, subcutaneous masses in the
extremities (19). Plain
radiographs reveal a non-specific soft-tissue mass with an
incomplete rim of ossification. MRI usually shows an intermediate
signal intensity on T1-weighted sequences and an intermediate to
high signal intensity on T2-weighted sequences (20). Histologically, ossifying fibromyxoid
tumors are composed of uniform round, ovoid or spindle-shaped cells
that are arranged in nests and cords and deposited in a variably
fibromyxoid stroma. A balanced or unbalanced translocation,
t(6;12)(p21;q24), appears to be characteristic of an ossifying
fibromyxoid tumor (19).
Chondroid lipomas are rare variants of lipomas that
usually occur in young and middle-aged adults, with a female
predominance. These lipomas typically present as slow-growing,
painless masses in the proximal extremities and limb girdles
(1). Chondroid lipomas may also
exhibit ossification or calcification (21–23).
MRI usually reveals a heterogeneous signal intensity on T1-weighted
sequences and a variable heterogeneous high signal intensity on
T2-weighted sequences (22).
Histologically, chondroid lipomas are composed of strands and nests
of round cells and mature adipocytes in a myxochondroid matrix. A
reciprocal translocation, t(11;16)(q13;p13), resulting in a
C11orf95-MKL2 fusion gene, is highly specific for a chondroid
lipoma (24).
Well-differentiated liposarcomas are the most common
form of liposarcoma that are encountered in late adult life. The
condition typically presents as a slow-growing, painless mass in
the lower extremities, particularly the thigh. The presence of
ossification within a well-differentiated liposarcoma is a rare
occurrence (25). MRI usually shows
a largely lipomatous mass representing >75% of the lesion and
non-adipose components in a thick septa (>2 mm) of irregular
aspect or nodular foci (11).
Histologically, a well-differentiated liposarcoma predominantly
consists of mature adipocytes with a variable number of
spindle-shaped cells with hyperchromatic nuclei and multivacuolated
lipoblasts. Cytogenetically, a well-differentiated liposarcoma is
characterized by the presence of a supernumerary ring and giant
marker chromosomes (1).
In summary, the imaging features of an
osteochondrolipoma with a clinicopathological correlation have been
described. Clinicians should consider osteochondrolipoma as a
possible diagnosis for a well-defined, calcified/ossified,
subcutaneous mass in the scapular region.
Acknowledgements
This study was supported in part by the Ogata
Foundation and the Foundation for the Promotion of Medical
Science.
References
|
1
|
Nishio J: Contributions of cytogenetics
and molecular cytogenetics to the diagnosis of adipocytic tumors. J
Biomed Biotechnol. 2011:5240672011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nielsen GP and Mandahl N: Lipoma. World
Health Organization Classification of Tumours of Soft Tissue and
Bone. Fletcher CDM, Bridge JA, Hogendoorn PCW and Mertens F: IARC
Press; Lyons: pp. 20–21. 2013
|
|
3
|
Kuyama K, Fifita SF, Komiya M, Sun Y,
Akimoto Y and Yamamoto H: Rare lipomatous tumors with osseous
and/or chondroid differentiation in the oral cavity report of two
cases and review of the literature. Int J Dent. 2009:1434602009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Obermann EC, Bele S, Brawanski A, Knuechel
R and Hofstaedter F: Ossifying lipoma. Virchows Arch. 434:181–183.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Demiralp B, Alderete JF, Kose O, Ozcan A,
Cicek I and Basbozkurt M: Osteolipoma independent of bone tissue: a
case report. Cases J. 2:87112009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cheng S, Lu SC, Zhang B, Xue Z and Wang
HW: Rare massive osteolipoma in the upper part of the knee in a
young adult. Orthopedics. 35:e1434–e1437. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fritchie KJ, Renner JB, Rao KW and Esther
RJ: Osteolipoma: radiological, pathological, and cytogenetic
analysis of three cases. Skeletal Radiol. 41:237–244. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lin TM, Chang HW, Wang KH, Kao AP, Chang
CC, Wen CH, Lai CS and Lin SD: Isolation and identification of
mesenchymal stem cells from human lipoma tissue. Biochem Biophys
Res Commun. 361:883–889. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Heffernan EJ, Lefaivre K, Munk PL, Nielsen
TO and Masri BA: Ossifying lipoma of the thigh. Br J Radiol.
81:e207–e210. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yabe Y, Kumagai J, Koizumi N, Kawamura M,
Ono S and Hatori M: Osteolipoma arising adjacent to the
sternoclavicular joint. A case report. Ups J Med Sci. 111:257–261.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gaskin CM and Helms CA: Lipomas, lipoma
variants, and well-differentiated liposarcomas (atypical lipomas):
results of MRI evaluations of 126 consecutive fatty masses. AJR Am
J Roentgenol. 182:733–739. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Minutoli F, Mazziotti S, Gaeta M, Vinci S,
Mastroeni M and Blandino A: Ossifying lipoma of the parapharyngeal
space: CT and MRI findings. Eur Radiol. 11:1818–1821. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chung EB and Enzinger FM: Chondroma of
soft parts. Cancer. 41:1414–1424. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kransdorf MJ and Meis JM: From the
archives of the AFIP. Extraskeletal osseous and cartilaginous
tumors of the extremities. Radiographics. 13:853–884. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gulati Y, Maheshwari A, Sharma V, Mattoo
R, Arora D and Gupta N: Extraskeletal osteochondroma of the thigh:
a case report. Acta Orthop Belg. 71:115–118. 2005.PubMed/NCBI
|
|
16
|
Sheff JS and Wang S: Extraskeletal
osteochondroma of the foot. J Foot Ankle Surg. 44:57–59. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nishio J, Nabeshima K, Iwasaki H and Naito
M: Non-traumatic myositis ossificans mimicking a malignant neoplasm
in an 83-year-old woman: a case report. J Med Case Rep.
4:2702010.PubMed/NCBI
|
|
18
|
Enzinger FM, Weiss SW and Liang CY:
Ossifying fibromyxoid tumor of soft parts: A clinicopathological
analysis of 59 cases. Am J Surg Pathol. 13:817–827. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nishio J: Updates on the cytogenetics and
molecular cytogenetics of benign and intermediate soft tissue
tumors. Oncol Lett. 5:12–18. 2013.PubMed/NCBI
|
|
20
|
Ideta S, Nishio J, Aoki M, Ishimatsu T,
Nabeshima K, Iwasaki H and Naito M: Imaging findings of ossifying
fibromyxoid tumor with histopathological correlation: A case
report. Oncol Lett. 5:1301–1304. 2013.PubMed/NCBI
|
|
21
|
Hyzy MD, Hogendoorn PC, Bloem JL and De
Schepper AM: Chondroid lipoma: findings on radiography and MRI
(2006:7b). Eur Radiol. 16:2373–2376. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hoch B, Hermann G, Klein MJ and Abdelwahab
IF: Ossifying chondroid lipoma. Skeletal Radiol. 37:475–480. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Setiawati R, Dimpudus FJ and Sun Z:
Chondroid lipoma of the right thigh: Correlation of imaging
findings and histopathology of an unusual benign lesion. Australas
Med J. 5:355–358. 2012.PubMed/NCBI
|
|
24
|
Huang D, Sumegi J, Dal Cin P, Reith JD,
Yasuda T, Nelson M, Muirhead D and Bridge JA: C11orf95-MKL2 is the
resulting fusion oncogene of t(11;16)(q13;p13) in chondroid lipoma.
Genes Chromosomes Cancer. 49:810–818. 2010.PubMed/NCBI
|
|
25
|
Javery O, Jagannathan JP, Saboo SS,
O'Regan K, Hornick JL and Ramaiya N: Case report: atypical
lipomatous tumor with unusual extensive metaplastic ossification.
Cancer Imaging. 12:25–30. 2012. View Article : Google Scholar : PubMed/NCBI
|