Introduction
A giant cell tumour (GCT) is generally considered as
a benign tumour originating from the bone. Extraosseous giant cell
tumours have been reported in a number of organs, including the
temporomandibular joint (1), larynx
(2), maxillary sinus (3) and other soft tissues. Primary giant
cell tumours of the parotid gland (GCTPs) were first described by
Eusebi et al in 1984 (4). A
GCTP is considered to be extremely rare, with only a few
well-documented, histopathologically-confirmed cases previously
published in the English literature. In addition, the majority of
previous studies have been performed by pathologists and have
focused on discussing the histopathological observations of GCTP.
The present case report is the first to analyse the treatment
policy and prognosis of GCTP. Therefore, the current study presents
a rare case of GCTP and a review of the literature in order to
improve our understanding of this disease. Written informed consent
was obtained from the patient.
Case report
A 58-year-old male was admitted to Kaohsiung
Veterans General Hospital (Kaohsiung, Taiwan) with an 11-month
history of a non-tender mass over the left preauricular area with
no relevant medical history. A physical examination revealed a
painless, hard, elastic mass (4×3 cm) over the left preauricular
area. The results of a head and neck examination were within normal
limits and facial nerve function was intact. A fine-needle
aspiration was performed over the left parotid gland using a
22-gauge needle and the histopathological study was not able to
exclude the presence of a malignancy. Subsequent observations by
computed tomography showed that a mass (4×3×1.5 cm3) was
occupying the deep lobe of the left parotid gland (Fig. 1).
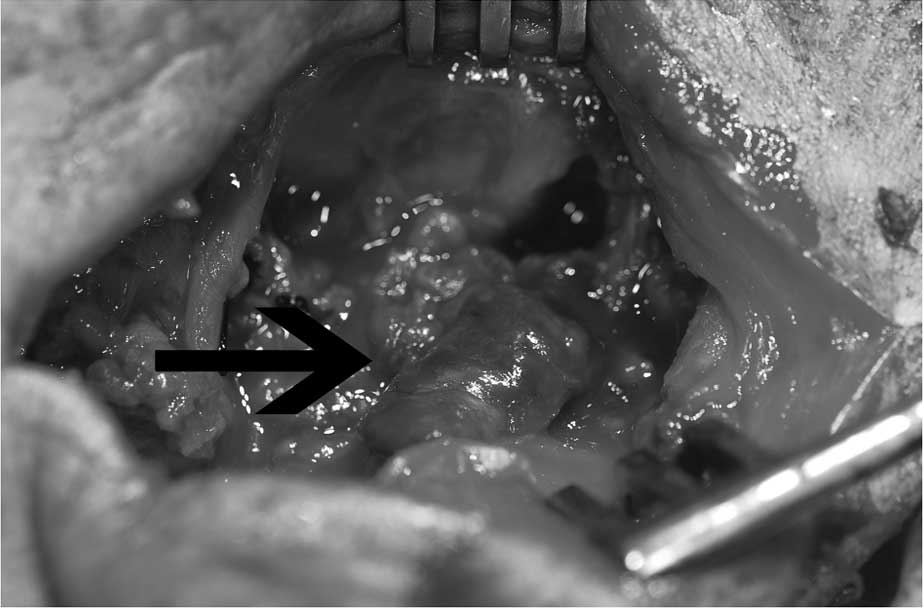
The patient received a total parotidectomy due to
suspected malignancy. Following confirmation of all the facial
nerve branches, the superficial lobe of the left parotid gland was
resected and the tumour was exposed (Fig. 2). The tumour (4×3×1.5
cm3) was observed to be occupying the deep lobe of the
left parotid gland. Following removal of the tumour, the facial
nerve trunk and its branches were preserved over the deep lobe of
the left parotid gland.
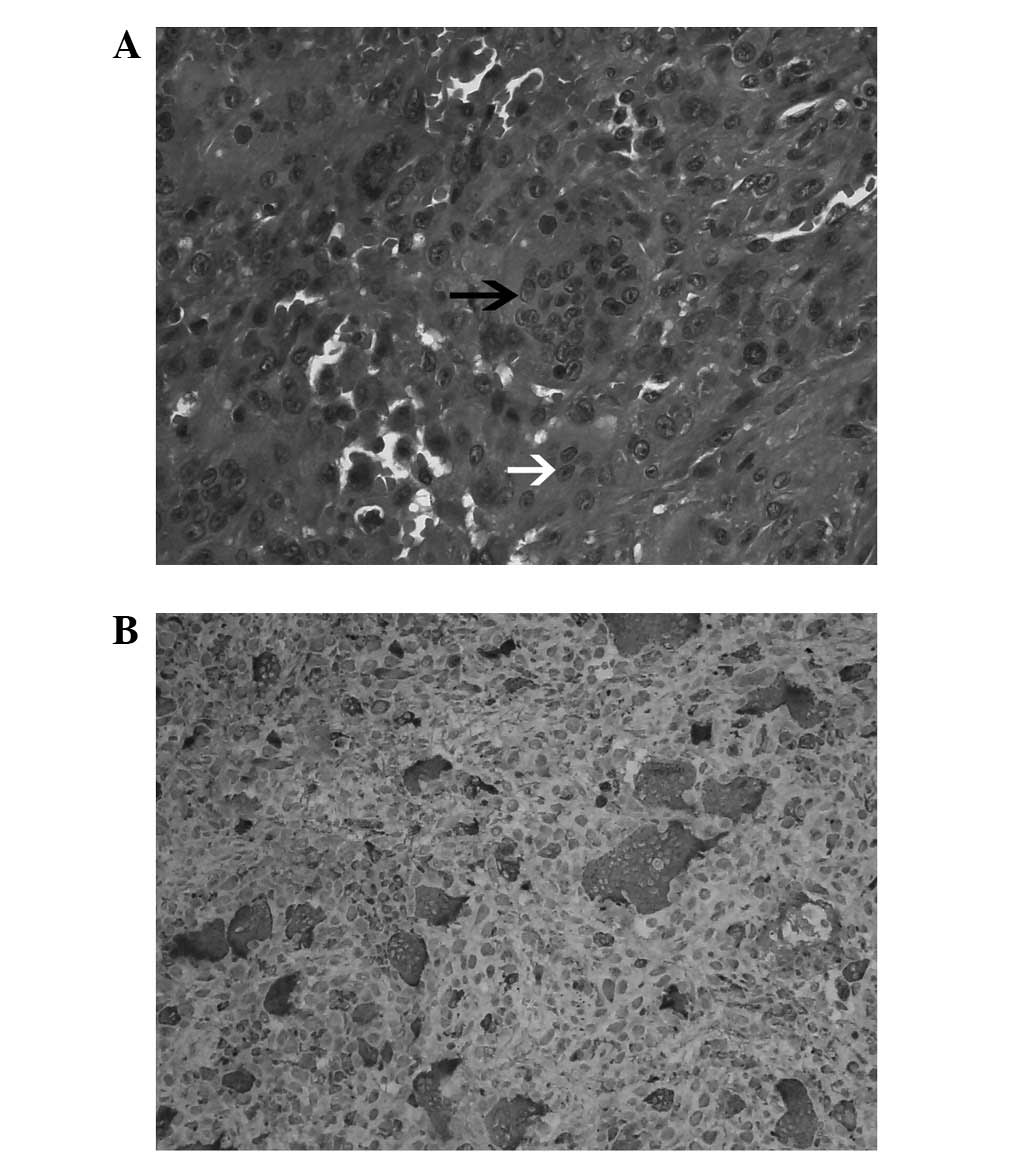
The tumour was sent for histopathological
examination by immunohistochemistry. The sections of the specimen
were identified as that of a giant cell tumour, composed of
uniformly distributed osteoclast-like giant cells, admixed with
mononuclear cells and numerous brown hemosiderin-laden macrophages
(Fig. 3A). The immunohistochemistry
results identified that the osteoclast-like giant and mononuclear
cells were positive for CD68 (Fig.
3B) and negative for cytokeratin, S100 and HMB-45.
Following surgery, the patient was referred to the
Department of Radiation Oncology (Kaohsiung Veterans General
Hospital, Kaohsiung, Taiwan) for adjuvant radiation therapy since
surgical margins were not achieved. Treatment consisted of surgical
excision associated with adjuvant radiation therapy. No facial
palsy was observed following surgery and radiation therapy (6400
cGy, 32 fractions over the tumor bed in the left parotid fossa),
and the individual exhibited no recurrence of a neoplasm after 2
years of follow-up.
Discussion
GCTs are generally considered as benign tumours that
originate from the bone. Extraosseous giant cell tumours have been
reported in a number of organs, including the temporomandibular
joint (1), larynx (2), maxillary sinus (3) and other soft tissues. Primary GCTPs
were first described by Eusebi et al in 1984 (4), however, due to their rarity, there is
an absence of literature that has analysed GCTP and all published
material has been case reports. A summary of fifteen case reports,
located using PubMed in a search of data up to May 2012, are
presented in Table I(4–13). The
most common clinical presentation of a GCTP was a non-tender,
growing mass over the preauricular area followed by swelling of the
parotid gland. The average age at presentation was 62.6 years and
ranged between 30 and 92 years. In addition, 19% of patients (3/16)
were <50 years old at diagnosis, whereas 56% of patients (9/16)
were >60 years old. The male to female ratio was 7:1, indicating
a male predilection for GCTPs, an observation that, to the best of
our knowledge, has not been previously reported. By contrast, GCTs
of the bone had a female predilection.
 | Table ISummary of GCTPs from previous
studies. |
Table I
Summary of GCTPs from previous
studies.
| First author
(ref.) | Age, years | Gender | Size, cm | Carcinomatous
component | Surgery | Radiation
therapy | Meta | Follow-up
(months) |
|---|
| Eusebi et
al(4) | 30 | M | 2.2 | No | Parotidectomy | No | No | NED (48) |
| Eusebi et
al(4) | 52 | M | 1×0.8×0.8 | No | Parotidectomy | No | No | NED (48) |
| Eusebi et
al(4) | 43 | M | 2×1.5 | Ex pleomorphic
adenoma | Parotidectomy | No | No | NED (60) |
| Balogh et
al(5) | 67 | M | 6×5×4 | Infiltrating
intraductal | Parotidectomy ductal
Ca | RT was stopped due to
poor tolerance | P | DWD (28) |
| Batsakis et
al(6) | 59 | M | 3×2.5×2.5 | High-grade
ductal | Parotidectomy | No | No | NED (12) |
| Batsakis et
al(6) | 92 | M | 2×1.5×1.5 | No | Parotidectomy with en
bloc resection of parapharyngeal space tumour | No | No | NED (9) |
| Ellis et
al(7) | 70 | F | NA | No | NA | NA | No | NA |
| Ellis et
al(7) | 65 | M | NA | No | NA | NA | No | NA |
| Ellis et
al(7) | 73 | M | NA | No | NA | NA | No | NA |
| Itol et
al(8) | 53 | M | 8×6 | No | Parotidectomy | No | No | NA |
| Grenko et
al(9) | 66 | F | 5 | Carcinomsarcoma with
a salivary duct | Parotidectomy | No | P | DWD (13) |
| Donath et
al(10) | 82 | M | 1.5 | Ex pleomorphic
adenoma | NA | No | No | NA |
| Tse et
al(11) | 75 | M | 1.1 | Salivary duct | Parotidectomy | No | No | NA |
| Kadivar (12) | 75 | M | 6.5 | Salivary duct | Parotidectomy and
neck dissection | No | C | NA |
| Fang et
al(13) | 43 | M | 7×7×6.5 | Salivary duct | Parotidectomy | No | No | NED (12) |
| Present case | 58 | M | 4×3×1.5 | No | Parotidectomy | Yes | No | NED (24) |
A GCTP is a rare primary soft-tissue tumour that is
pathologically and clinically similar to a GCT of the bone.
However, it is recognised as a distinct entity in the World Health
Organization Classification of Tumours for soft tissue and bone
(14). Although the two tumours may
be indistinguishable morphologically, various clinical results and
histological features aid in the differentiation between the two.
GCTP is biologically more aggressive and, morphologically, may show
decreased mitotic activity, a lack of reactive bone formation at
the periphery of the tumour and is commonly admixed with a
mononuclear component (12). The
resected specimen of the patient was identified as a GCT, composed
of uniformly distributed osteoclast-like giant cells, admixed with
mononuclear cells and exhibiting a lack of bone formation at the
periphery of the tumour. The giant cells were large, multinucleated
(10–50 nuclei) and shown to be positive for CD68 and negative for
cytokeratin, S100 and HMB-45. Mitotic activity measured up to 2/10
HPF, with an absence of atypical mitosis and cytological atypism.
The identification of a GCTP should warrant an investigation for a
carcinomatous component since this component is likely to be focal
and small (12).
Among the 16 patients with available treatment
records, the majority received a parotidectomy alone. One patient
was managed by a parotidectomy with neck dissection due to cervical
lymph node metastasis, and an additional patient received
parotidectomy with en bloc resection of the parapharyngeal space
tumour due to parapharyngeal invasion. Eight patients were
diagnosed with an associated carcinomatous component and were
managed by surgery alone. Of these patients, two succumbed to the
disease within <28 months. All eight patients who were diagnosed
without an associated carcinomatous component remained free of
disease and survived. These observations indicate that GCTP
patients diagnosed with an associated carcinomatous component
exhibit increased mortality rates of up to 25% (2/8).
For the treatment of malignant parotid tumours,
parotidectomies and post-operative adjuvant radiation therapy have
been used (15). A previous study
reported that 59.4% of patients who had received radiation therapy
demonstrated a survival benefit (16). A GCTP is considered as a benign
soft-tissue tumour, but one with malignant potential. The
observations of the current case report indicate that the incidence
of an associated carcinomatous component in GCTP is extremely high
[50% of patients (8/160)] and is not likely to be due to incidental
coexistence (Table I).
The basic treatment for a GCT is extensive resection
of the tumour, allowing for a sufficient margin of the surrounding
normal tissue (8). A GCT is a
radiosensitive tumour and, therefore, radiotherapy is highly
effective. Radiotherapy is a reasonable option under conditions
where negative surgical margins may only be achieved with increased
morbidity or if surgery has been contraindicated (15). The patient presented in the current
case report received a total parotidectomy followed by adjuvant
radiation therapy due to negative surgical margins. Surgery alone
may not be suitable for patients diagnosed with an associated
carcinomatous component. A review of the related literature
revealed that 25% (2/8) of GCTP patients with a carcinomatous
component developed pulmonary metastasis and succumbed to the GCTP
(Table I). Among these eight
patients, seven did not receive radiation therapy, and the
radiation therapy of the single patient who did receive treatment
was terminated due to poor tolerance. By contrast, a GCT of the
temporomandibular joint may be well managed by complete removal of
the tumour alone rather than by complete surgery with combined
radiation therapy (1). The results
of the present report indicated that a combination of complete
surgery and post-operative radiation therapy is the treatment of
choice for achieving greater locoregional control and improved cure
rates for the treatment of patients with a carcinomatous component
or negative surgical margins.
In summary, GCTPs are uncommon benign tumours with a
malignant potential. The identification of a GCTP should warrant a
diligent search for a carcinomatous component. Complete surgical
removal of the tumour is the treatment of choice for a resectable
GCTP. In addition, surgery alone has been justified for the
management of a GCTP without a carcinomatous component. However,
combined radiation therapy is recommended if surgery has been
contraindicated, if surgical margins have not been achieved or if
GCTP has been diagnosed with an associated carcinomatous
component.
References
|
1
|
De Benedittis M, Turco M, Petruzzin M and
Cortelazzi R: Extra-articular diffuse-type giant cell tumour of the
temporomandibular joint. Int J Oral Maxillofac Surg. 42:380–385.
2013.PubMed/NCBI
|
|
2
|
Nishimura K, Satoh T, Maesawa C, et al:
Giant cell tumor of the larynx: a case report and review of the
literature. Am J Otolaryngol. 28:436–440. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hoffman CD, Huntley TA, Wiesenfeld D,
Kleid S and Kung IT: Maxillar giant cell tumour associated with
Paget’s disease of bone. Int J Oral Maxillofac Surg. 23:161–164.
1994.
|
|
4
|
Eusebi V, Martin SA, Govoni E and Rosai J:
Giant cell tumor of major salivary glands: report of three cases,
one occurring in association with a malignant mixed tumor. Am J
Clin Pathol. 81:666–675. 1984.PubMed/NCBI
|
|
5
|
Balogh K, Wolbarsht RL, Federman M and
O’Hara CJ: Carcinoma of the parotid gland with osteoclastlike giant
cells. Immunohistochemical and ultrastructural observations. Arch
Pathol Lab Med. 109:756–761. 1985.PubMed/NCBI
|
|
6
|
Batsakis JG, Ordonez NG, Sevidal PA Jr and
Baker JR: Osteoclast-type giant cell neoplasms of the parotid
gland. J Laryngol Otol. 102:901–904. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ellis GL, Auclair PL and Gnepp DR:
Surgical pathology of the salivary glands. Major Problems in
Pathology Series. 25. WB Saunders; Philadelphia, PA: pp. 490–509.
1991
|
|
8
|
Itoh Y, Taniguti Y and Arai K: A case of
giant cell tumor of the parotid gland. Ann Plast Surg. 28:183–186.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Grenko RT, Tytor M and Boeryd B:
Giant-cell tumor of the salivary gland with associated
carcinosarcoma. Histopathol. 23:594–595. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Donath K, Seifert G and Röser K: The
spectrum of giant cells in tumours of the salivary glands: an
analysis of 11 cases. J Oral Pathol Med. 26:431–436. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tse LL, Finkelstein SD, Siegler RW and
Barnes L: Osteoclast-type giant cell neoplasm of salivary gland. A
microdissection-based comparative genotyping assay and literature
review: extraskeletal ‘giant cell tumor of bone’ or osteoclast-type
giant cell ‘carcinoma’? Am J Surg Pathol. 28:953–961.
2004.PubMed/NCBI
|
|
12
|
Kadivar M, Nilipour Y and Sadeghipour A:
Osteoclast-like giant-cell tumor of the parotid with salivary duct
carcinoma: case report and cytologic, histologic, and
immunohistochemical findings. Ear Nose Throat J. 86:628–630.
2007.PubMed/NCBI
|
|
13
|
Fang X, Hicks DG, Hicks W Jr and Zhang S:
Osteoclastlike giant cell tumor of the salivary gland. Ann Diagn
Pathol. 13:114–118. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Barnes L, Eveson JW, Reichart P and
Sidransky D: World Health Classification of Tumours. Pathology and
Genetics of Head and Neck Tumours. IARC Press; Lyon: 2005
|
|
15
|
Lin CC, Tai MH, Huang CC, et al: Parotid
tumors: a 10-year experience. Am J Otolaryngol. 29:94–100.
2008.PubMed/NCBI
|
|
16
|
Bhattacharyya N and Fried MP: Determinants
of survival in parotid gland carcinoma: a population-based study.
Am J Otolaryngol. 26:39–44. 2005. View Article : Google Scholar : PubMed/NCBI
|