Introduction
The HER (ErbB) receptor family consists of four
receptors: HER1 (EGFR, ErbB1), HER2 (Neu, ErbB2), HER3 (ErbB3) and
HER4 (ErbB4) that express tyrosine kinase activity in the
intracellular domain. The ErbB abbreviation derives from the
erythroblastic leukemia oncogenic virus (erythroblastic leukemia
viral oncogene), which is structurally homologous to human HER
receptors (1). The signal for
epithelial cell proliferation is transduced to the cell nucleus as
a result of the homo- and heterodimerization of HER receptors and
activation of the complex by corresponding ligand binding. The
preferred partner for EGFR heterodimerization is the HER2 receptor,
which is also known to be overexpressed in breast cancer (2). Mutations within the tyrosine kinase
domain of the EGFR gene, mainly deletions in exon 19 or
substitution L858R in exon 21, are detected in ~10% of Caucasian
patients with non-small cell lung cancer (NSCLC) (3). Additionally, the EGFR gene
mutation affects the efficacy of EGFR tyrosine kinase
inhibitors (TKIs). There is certain evidence that HER2 gene
mutations, and perhaps the high expression of the HER2
receptor, may be involved in the etiology of certain NSCLC cases
(4).
Mutations in the HER2 gene tyrosine kinase
domain are extremely rare in NSCLC patients (5). Preliminary data show that the
prevalence is not higher than 2% in the general patient population
(6). The mutations are most often
indicated in non-smoking females with adenocarcinoma of the lung
(7). The most significant mutations
are two different insertions of 12 base pairs, which impair the
reading frame in exon 20 of the HER2 gene: A775YVMA (66% of
all detected mutations in the HER2 gene) or M774AYVM. These
mutations are identical to the insertion of nine base pairs in exon
20 of the EGFR gene, which makes the structure of the
tyrosine kinase domain of the HER2 protein similar to the structure
of the tyrosine kinase domain of the EGFR gene, modified by
the mentioned mutations (5). Based
on this, it is assumed that A775YVMA or M774AYVM mutations of the
HER2 gene cause similar consequences to the mutations in
exon 20 of the EGFR gene (8). Taking into account that the HER2
receptor predominantly undergoes heterodimerization with EGFR, the
narrowing of the binding pocket for ATP, resulting from a mutation
in exon 20 of the EGFR or HER2 genes in heterodimer
EGFR/HER2, leads to the increased activity of the tyrosine kinases
of those receptors (9). This
results in an increase of the phosphorylation of further signal
proteins, cancer cell proliferation and resistance (or declined
susceptibility) to reversible EGFR TKIs (10).
In the future, the presence of the A775YVMA or
M774AYVM mutations in the HER2 gene may be a potential
predictive marker of effectiveness of HER family TKIs and be a
target for new molecular targeted therapies. The detection of an
insertion in exon 20 of the HER2 gene may play a role in
therapy design, and be as important as the current assessment for
T790M mutations in the EGFR gene, which appears to be a main
cause of resistance for reversible EGFR TKIs (50% of all acquired
resistance). It should be noted that the brain is the most frequent
location for metastases of lung adenocarcinoma. However, there is
limited evidence on the prevalence of HER2 gene mutations in
metastatic NSCLC and in patients with histologies other than
adenocarcinoma.
Materials and methods
Patients
The present study retrospectively analyzed 143
patients (99 male and 44 female) ranging in age between 38 and 81
years (59.8±8.8 years), for whom paraffin-embedded cancer tissue
from NSCLC metastatic lesions in the brain was available. The
patients underwent routine neurosurgical procedures with a
palliative aim. In 32 patients, material from the primary tumor,
obtained during thoracoscopy, intrabronchial, transbronchial or
transthoracic biopsy, was available. Written informed consent was
obtained from all patients. This study was approved by the Ethics
Committee of the Medical University of Lublin, Poland (No.
KE-0254/131/2011).
Lung adenocarcinoma was diagnosed in 61 patients
(42.6%). Squamous and large cell carcinomas were confirmed in 23
(16.1%) and 21 (14.7%) cases, respectively. In 38 patients (26.6%)
the NSCLC subtype was impossible to assess and they were diagnosed
as not otherwise specified (NOS). The median survival time from
lung cancer diagnosis to death was 9.2 months. None of the patients
were treateadted with EGFR TKI (EGFR TKI naïve).
Identification of mutations
DNA was isolated from paraffin-embedded material
containing metastatic lesions and from primary tumor tissues using
a QIAamp DNA FFPE tissue kit (Qiagen, Valencia, CA, USA).
Estimation of the insertion in exon 20 of the HER2 gene was
conducted using a PCR reaction with primers flanking the mutated
region of the HER2 gene. Primers were fluorescently labeled
(Cy5). Amplified DNA fragment length analysis (DNA-FLA) was applied
using an ALF Express II sequencer (Amersham Pharmacia Biotech AB,
Uppsala, Sweden) in polyacrylamide gel. The HER2 gene
mutation was also confirmed by the native electrophoretic
separation multi-temperature single-strand conformation
polymorphism (MSSCP) technique (11), which allows separation of the
different conformers of single-stranded (ss)DNA fragments, in order
to differentiate wild-type HER2 from mutated-type
HER2. In the MSSCP-based minor variant enrichment procedure,
the PCR products were analyzed at strictly controlled temperatures
(±0.2°C) using dedicated equipment, the DNAPointer®
System (BioVectis, Warsaw, Poland), as described by Kaczanowski
et al(11). In general, the
PCR products were heat denatured and ssDNA conformers were resolved
on 9% polyacrylamide gel with 5% glycerol in native conditions (TBE
buffer) at three different temperatures (35, 25 and 15°C) during
one run. Subsequently, the DNA bands were visualized by silver
nitrate staining (SilverStain DNA kit; BioVectis). Fragments of the
MSSCP gel containing the bands of interest were cut out and the
ssDNA was eluted and re-amplified using primers and PCR conditions
as described previously. For subsequent DNA Sanger sequencing
(12) a 1/10 volume of obtained PCR
products was used (3730xl DNA Analyzer, Applied Biosystems,
Carlsbad, CA, USA).
Additionally, the deletion in exon 19, substitution
L858R in the EGFR gene and mutation V600E in the BRAF
gene, were assessed in the analyzed material.
Results
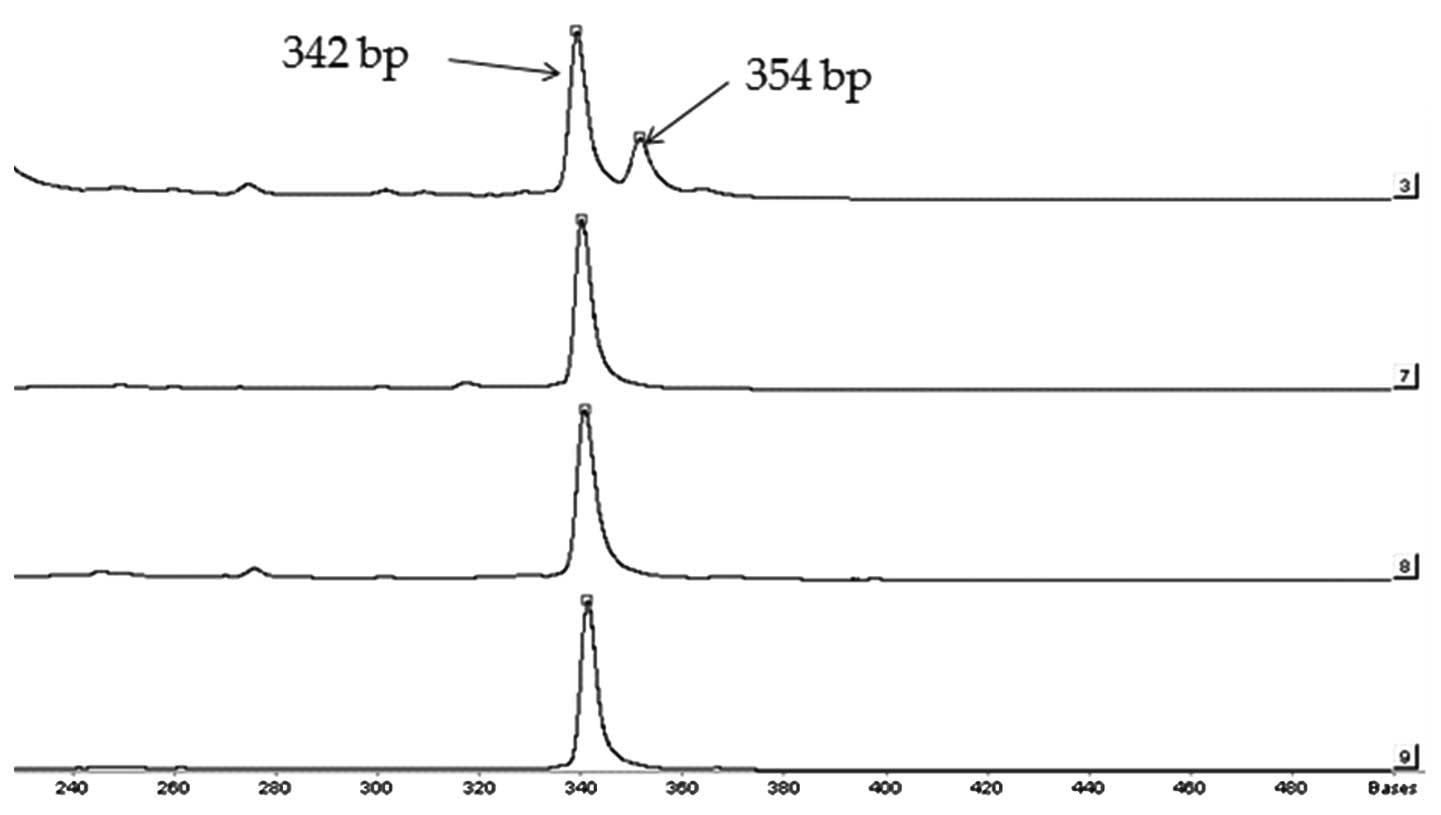
The insertion in exon 20 of the HER2 gene
(insertion version A775YVMA or M774AYVM) was indicated in a single
patient, who only had material from the NSCLC metastatic lesion
available (0.67% of all analyzed patients and 1.5% of
adenocarcinoma patients; Fig. 1).
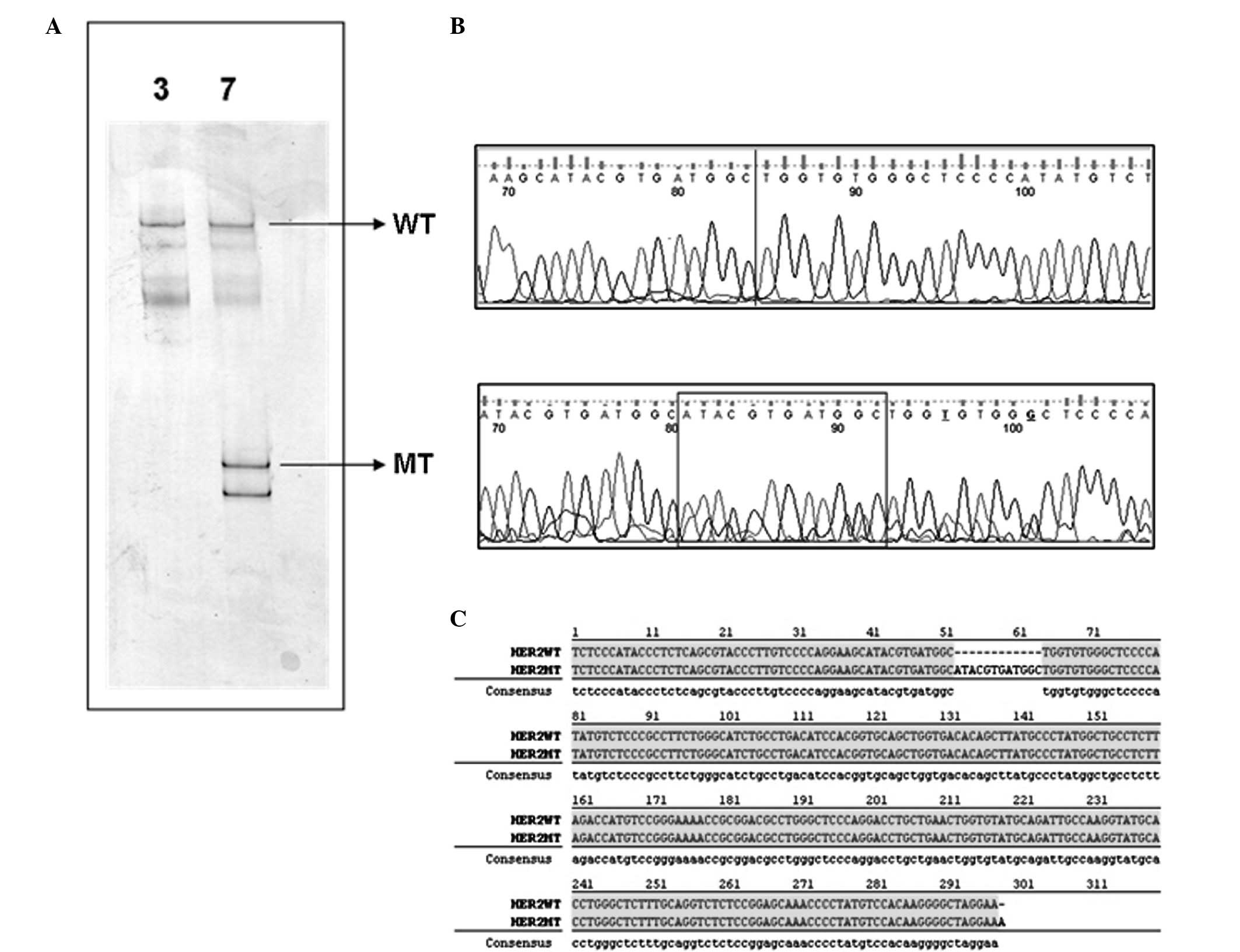
The mutation was confirmed by the MSSCP technique (Fig. 2). The patient was a 77-year-old
non-smoking male, with advanced poorly-differentiated lung
adenocarcinoma with metastases in the cerebellum. Due to the low
performance status following neurosurgery, and taking into account
the advanced stage of the disease, the patient was not treated with
chemotherapy, radiotherapy or molecular targeted therapy.
Additionally, molecular assessments led to exclusion of other
activating mutations in exons 19, 20 (T790M) and 21 (L858R) of the
EGFR gene, as well as V600E substitution in the BRAF
gene in the patient with the HER2 mutation.
In total, 9 activating mutations (6.3%) of the
EGFR gene were detected in brain samples, these consisted of
three delE746-A750 deletions of 15 base pairs in exon 19 (2.1%) and
six with L858R substitutions in exon 21 (4.2%). Two deletions in
exon 19 were detected in giant cell carcinoma patients and one in
an adenocarcinoma patient, while all L858R substitutions were
diagnosed in adenocarcinoma patients. Evaluation of the primary
tumors revealed EGFR mutations similar to those in
corresponding metastases: One delE746-A750 deletion in exon 19 and
one L858R substitution in exon 21. Additionally, V600E
substitutions in the BRAF gene were not detected in the
brain metastases of the NSCLC patients.
Additionally, the results obtained using PCR
analysis were verified with the use of the MSSCP method. As shown
in Fig. 2, MSSCP separation of exon
20 HER2 sample numbers 72 (line 3) and 7 (line 7),
recognized previously as the wild-type (WT) and mutated variant
(MT), respectively, revealed their distinct electrophoretic
profiles. Sample 7 contained additional ssDNA bands, which were not
observed in sample 72 (Fig. 2A). It
was assumed that similar ssDNA bands detected in each of the two
samples indicated the WT HER2 genetic variant. Considering
that the MSSCP method is based on non-denaturing polyacrylamide
electrophoresis, additional ssDNA bands suggested the presence of
DNA conformers, representing additional amplicon sequences. To
verify this hypothesis, indicated ssDNA bands were cut out from the
gel and the DNA was recovered, re-amplified and Sanger sequenced.
Further analysis of the obtained DNA sequences confirmed our
suppositions (Fig. 2B). According
to the BLAST database, the ssDNA bands observed in samples 72 and
7, corresponded to the WT HER2 sequence. Additional ssDNA
bands in sample 7 contained the mutated HER2 sequence with a
12-nucleotide insertion. The described results fully confirmed that
sample number 7 was a mixture of two genetic variants of the
HER2 amplicon. The comparison of the WT and the MT DNA
sequence detected in sample 7 is illustrated in Fig. 2C.
Discussion
The present study has shown that primary HER2
gene mutations are detectable in Caucasian patients with NSCLC.
Furthermore, HER2 gene mutations were indicated in
metastatic lesions of lung cancer in the cerebellum, which, to the
best of our knowledge is the first report of this worldwide.
HER2 gene mutations are believed to be responsible for the
development of these lung cancer types, which occur independent of
smoking and are mainly adenocarcinomas. However, the prevalence of
HER2 gene mutations in Caucasian patients is extremely low;
in the present study, it has been recorded as occurring in <1%
of patients with NSCLC.
Shigematsu et al have searched for
HER2 gene mutations in 671 primary NSCLC tumors and 80 NSCLC
cell lines, as well as in other types of cancer (14). The authors identified different
insertions in exon 20 of the HER2 gene in 11 patients with
NSCLC (1.6%) and in one lung adenocarcinoma cell line (NCI-H1781).
This mutation was not observed in other types of cancer, including
55 SCLC tumors. HER2 gene mutations were more frequent in
non-smokers (3.2%; 8/248) and were present solely in patients with
adenocarcinomas (2.8%; 11/394). Additionally they were more
frequent in female (2.7%; 7/258) compared with male (1%; 4/413)
patients. Notably, only one mutation was diagnosed in Caucasian
patients (0.7%; 1/137) (5). In
another study of 95 patients with NSCLC, Sasaki et al
described only one non-smoking female patient with lung
adenocarcinoma harboring an insertion of 12 nucleotides in exon 20
of the HER2 gene (6).
Buttitta et al diagnosed HER2 gene mutations in 9 out
of 403 Caucasian patients with lung adenocarcinoma (2.2%), but only
7 mutations were determined to be an insertion of 12 nucleotide
pairs in exon 20. Mutations were more frequent in female (4.1%) and
non-smoking (3.1%) patients with bronchioalveolar cancer (6.2%),
however, they were also indicated in male patients (1.8%) and
smokers (1.9%) (7).
The data from the aforementioned studies, as well as
that from the present study, are contrary to the data of Stephen
et al, which showed that mutations in the tyrosine kinase
domain of the HER2 gene (different HER2 mutations and
abnormalities) are observed in up to 4% of patients with NSCLC (120
primary NSCLC tumors tested), of which, 10% of patients had
adenocarcinomas (8). Moreover, Li
et al described as many as 12 HER2 gene mutation
carriers in a group of 202 (6%) non-smoking Asian patients who
underwent surgery for treatment of lung adenocarcinomas (10).
Assuming that HER2 gene mutations are
so-called driver mutations, which drive the epithelial cells into
carcinogenesis, and that they do not coexist with other driver
mutations (in the present article the coincidence of insertions in
exon 20 of the HER2 gene with EGFR and BRAF gene mutations
was not confirmed), patients with these mutations may require
specifically targeted therapy against the tyrosine kinase of
HER2. However, TKIs that inhibit only EGFR tyrosine kinase
activity (gefitinib and erlotinib) in cases of only HER2
gene mutation are ineffective. The reversible, dual EGFR and HER2
tyrosine kinase inhibitor, lapatinib, has showed certain activity
in cell lines, but this is not clinically relevant in patients with
NSCLC (13,14). The irreversible ErbB family receptor
blocker, afatinib (BIBW 2992), which inhibits EGFR, HER2 and HER4
tyrosine kinases, has been shown to be effective in the elimination
of cancer cells with HER2 gene mutations in cell lines and
animal models (15–19). Moreover, the first case reports of
afatinib effectiveness in female patients with lung adenocarcinoma
who are carriers of HER2 gene mutations have been presented
(20). There are ongoing in
vitro experiments evaluating the feasibility of the use of
combined therapy with afatinib and sirolimus (an mTOR inhibitor) in
patients with HER2 gene mutations (4). Moreover, trastuzumab, a monoclonal
antibody directed against the extracellular HER2 domain,
which has effectively been used in breast cancer patients with
HER2 overexpression, may be effective in patients with NSCLC
that harbor HER2 gene mutations (21).
Based on the overall data we may conclude that gene
profile analysis in cancer patients may extend the scope of
molecular therapies used in patients with NSCLC. Moreover, in the
near future, the personalized therapy of NSCLC based on the
assessment of numerous different gene mutations in cancer cells may
become a reality.
Acknowledgements
This study was partially funded by the European
Community’s Seventh Framework Programme (FP7/2007–2013) under the
grant agreement in HEALTH-F2-2010-258677.
References
|
1
|
Hirsch FR, Varella-Garcia M and Cappuzzo
F: Predictive value of EGFR and HER2 overexpression in advanced
non-small lung cancer. Oncogene. 28:32–37. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sun M, Behrens C, Feng L, et al: HER
family receptor abnormalities in lung cancer brain metastases and
corresponding primary tumors. Clin Cancer Res. 15:4829–4837. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mounawar M, Mukeria A, Le Calvez F, et al:
Patters of EGFR, HER2, TP53, and KRAS mutation of p14arf expression
in non-small lung cancer in relation to smoking history. Cancer
Res. 67:5667–5672. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pao W and Girard N: New driver mutations
in non-small-cell lung cancer. Lancet Oncol. 12:175–180. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shigematsu H, Takahashi T, Nomura M, et
al: Somatic mutations of the HER2 kinase domain in lung
adenocarcinomas. Cancer Res. 65:1642–1646. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sasaki H, Shimizu S, Endo K, et al: EGFR
and erbB2 mutation status in Japanese lung cancer patients. Int J
Cancer. 118:180–184. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Buttitta F, Barassi F, Fresu G, et al:
Mutational analysis of the HER2 gene in lung tumors from Caucasian
patients: mutations are mainly present in adenocarcinomas with
bronchioloalveolar features. Int J Cancer. 119:2586–2591. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Stephen P, Hunter C, Bignell G, et al:
Lung cancer: intragenic ERBB2 kinase mutations in tumours. Nature.
431:525–526. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang SE, Narasanna A, Perez-Torres M, et
al: HER2 kinase domain mutation results in constitutive
phosphorylation and activation of HER2 and EGFR and resistance to
EGFR tyrosine kinase inhibitors. Cancer Cell. 10:25–38. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li C, Fang R, Sun Y, et al: Spectrum of
oncogenic driver mutations in lung adenocarcinomas from east asian
never smokers. PLoS One. 6:e282042011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kaczanowski R, Trzeciak L and Kucharczyk
K: Multitemperature single-strand conformation polymorphism.
Electrophoresis. 22:3539–3545. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sanger F, Nicklen S and Coulson AR: DNA
sequencing with chain terminating inhibitors. Proc Natl Acad Sci.
74:5463–5467. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Diaz R, Nguewa PA, Parrondo R, et al:
Antitumor and angiogenic effect of the dual EGFR and HER-2 tyrosine
kinase inhibitor lapatinib in a lung cancer model. BMC Cancer.
10:188–197. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shimamura T, Ji H, Minami Y, et al:
Non-small-cell lung cancer and Ba/F3 transformed cells harboring
the ERBB2 G776insV_G/C mutation are sensitive to the dual-specific
epidermal growth factor receptor and ERBB2 inhibitor HKI-272.
Cancer Res. 66:6487–6491. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Reid A, Vidal L, Shaw H and de Bono J:
Dual inhibition of ErbB1 (EGFR/HER1) and ErbB2 (HER2/neu). Eur J
Cancer. 43:481–489. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li D, Ambrogio L, Shimamura T, et al:
BIBW2992, an irreversible EGFR/HER2 inhibitor highly effective in
preclinical lung cancer models. Oncogene. 27:4702–4711. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Perera SA, Li D, Shimamura T, et al:
HER2YVMA drives rapid development of adenosquamous lung tumors in
mice that are sensitive to BIBW2992 and rapamycin combination
therapy. Proc Natl Acad Sci USA. 106:474–479. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shimamura T, Greulich H, Solca FF and Wong
KK: Efficacy of BIBW-2992, potent irreversible inhibitor of EGFR
and HER2 in human NSCLC xenografts in a transgenic mouse
lung-cancer model: C7–04. J Thorac Oncol. 2(suppl): S3802007.
|
|
19
|
Hirsh V: Afatinib (BIBW 2992) development
in non-small-cell lung cancer. Future Oncol. 7:817–825. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
De Greve J, Teugels E, De Mey J, et al:
Clinical activity of BIBW2992, an irreversible inhibitor of EGFR
and HER2 in adenocarcinoma of the lung with mutations in the kinase
domain of HER2neu. J Thorac Oncol. 4:S307(abstr). 2009.PubMed/NCBI
|
|
21
|
Heinmöller P, Gross C, Beyser K, et al:
HER2 status in non-small cell lung cancer: results from patient
screening for enrollment to a phase II study of herceptin. Clin
Cancer Res. 9:5238–5243. 2003.PubMed/NCBI
|