Introduction
Osteosarcoma (OS) is the most common malignant bone
tumor in adolescents and young adults, and is characterized by the
proliferation of tumor cells producing osteoid or an immature bone
matrix. Despite advances in multimodality treatments, consisting of
aggressive adjuvant chemotherapy and wide local excision, pulmonary
metastasis occurs in 60–80% of patients with OS and remains a major
cause of fatal outcomes (1–3). OS shows a profound propensity for the
involvement of the long bones of the appendicular skeleton, in
particular, the distal femur and the proximal tibia and humerus. OS
also tends to involve lesions of the metaphysis (4,5). The
proximal femur is involved in ~5% of all cases of OS (5).
Pathological fractures are present in 5–10% of
patients with OS (6). Pathological
fractures pose particular problems, as a fracture hematoma, which
nearly always contains tumor cells, may either be intracapsular,
thus contaminating the joint, or extracapsular, and is usually
associated with widespread contamination of the surrounding
tissues. When contamination is localized in the intracapsular
space, an extracapsular wide resection is an adequate treatment
(7). Extracapsular wide resections
around the knee joint are common. However, extracapsular wide
resections of the hip joint are uncommon due to the rarity of cases
of OS in this location. The present study describes the case of a
female who was diagnosed with OS of the proximal femur, with a
pathological fracture. The patient underwent an extracapsular
resection of the hip joint with subsequent reconstruction using a
pasteurized autograft-prosthesis composite. The present study
describes the clinical course of the patient and the novel surgical
procedure that was used to manage the OS with a pathological
fracture of the proximal femur. The study was conducted following a
clinical research review by the ethics committee of Toyama
University Hospital (Toyama, Japan). Informed consent was obtained
from the patient, who was advised that the data from the case would
be submitted for publication.
Case report
Patient
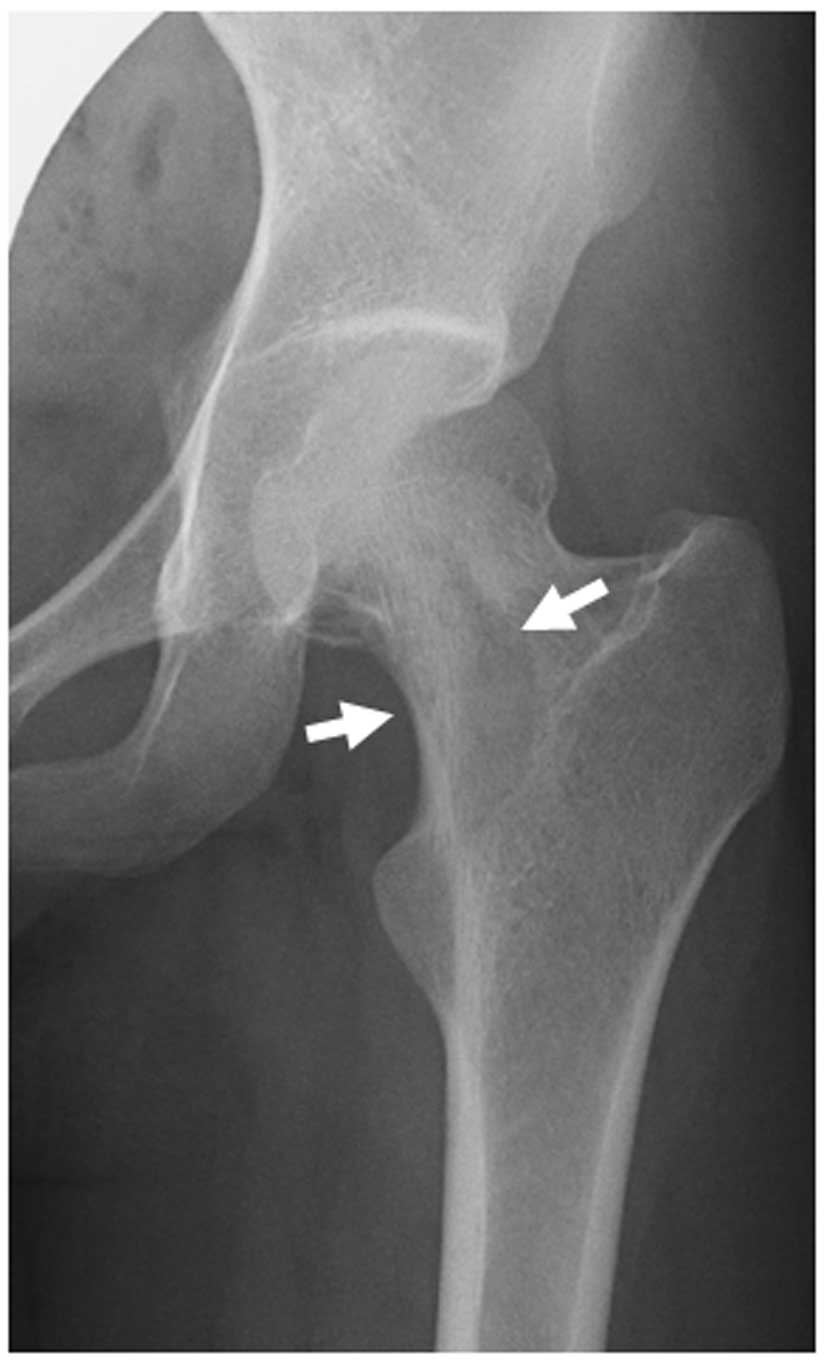
A 17-year-old female presented with a three-month
history of left hip pain. Plain radiography revealed an osteolytic
lesion with an osteosclerotic change to the femoral neck (Fig. 1). A periosteal reaction was not
observed. Computed tomography (CT) revealed an osteolytic lesion
with an osteosclerotic change and a pathological fracture of the
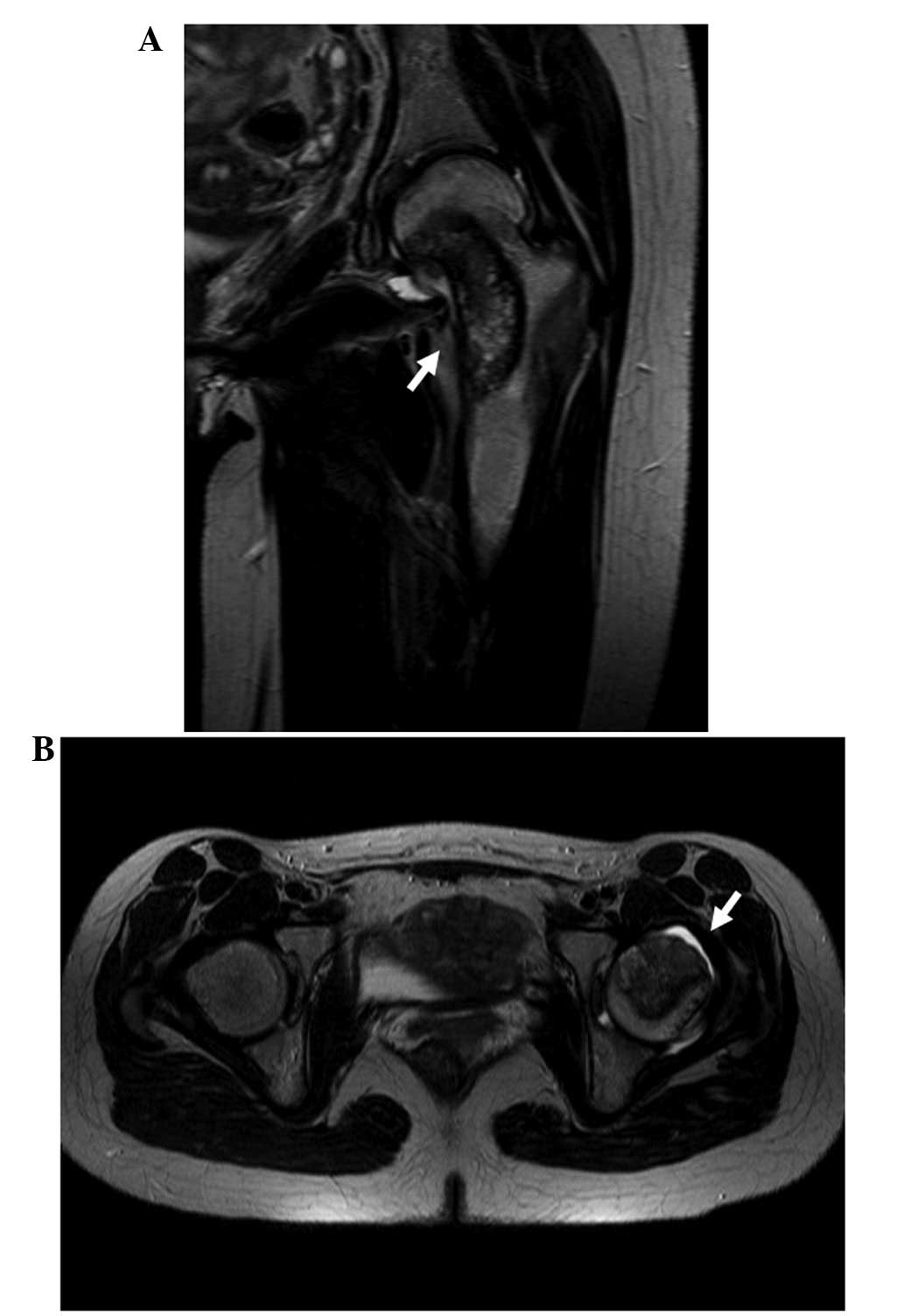
femoral neck (Fig. 2). T2-weighted
coronal magnetic resonance imaging (MRI) showed a heterogeneous
bone tumor arising from the femoral neck and extending to the
trochanteric site, which was hypointense compared with the bone
(Fig. 3A). Hyperintensity was
observed in the capsule of the hip joint due to hemorrhage
(Fig. 3B). Chest radiography and CT
revealed no evidence of lung metastasis. The initial differential
diagnosis was of a benign bone tumor, including a solitary bone
tumor, an aneurismal bone cyst or fibrous dysplasia. An open biopsy
was performed. The results from the examination of the
intraoperative frozen section were consistent with a fibrous benign
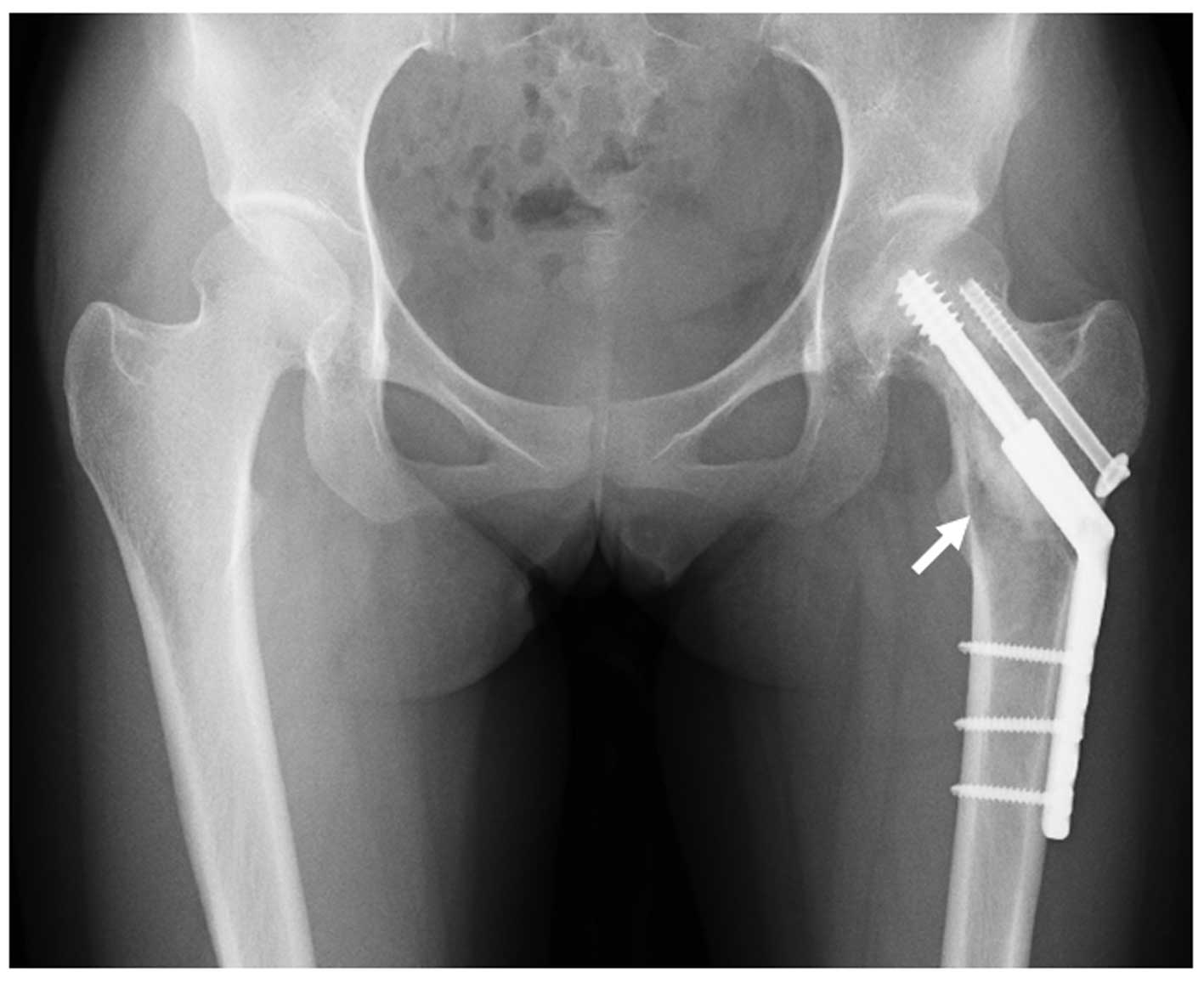
tumor. Due to the presence of the pathological fracture, tumor
curettage, hydroxyapatite (HA) granule (Apaceram®; Hoya
Co., Tokyo, Japan) transplantation and internal fixation using a
compression hip screw (CHS) system (Omega Plus T1; Stryker Japan
Co., Tokyo, Japan) were performed to prevent displacement and
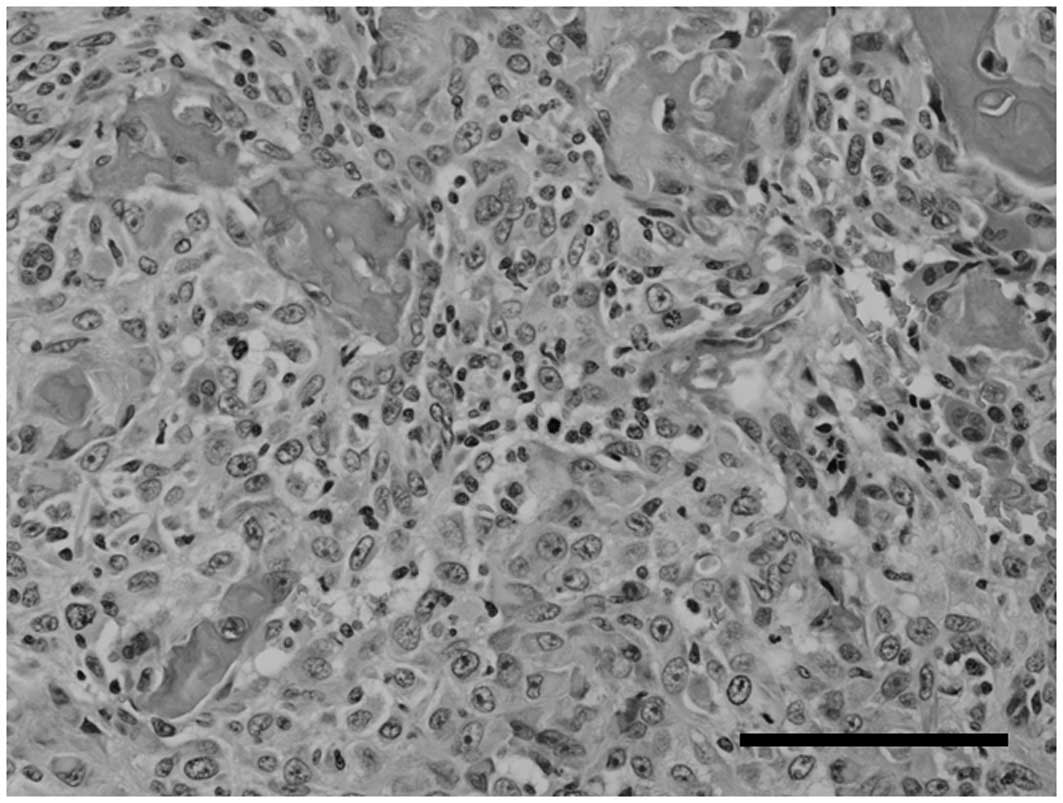
avascular necrosis of the femoral neck (Fig. 4). However, a histopathological study
of the resected specimen revealed that the tissue contained
atypical tumor cells and exhibited a formation of osteoid or
immature bone matrix (Fig. 5).
Immunohistochemically, the majority of the tumor cells were
strongly positive for vimentin and alkaline phosphatase (ALP).
Based on these data, a histopathological diagnosis of conventional
osteoblastic OS was made.
The patient was administered multiagent
chemotherapy, including high-dose methotrexate (HD-MTX; 10
g/m2 day 1), cisplatin (CDDP; 120 mg/m2 day
1) and adriamycin (ADM; 30 mg/m2 day 2), according to
the neoadjuvant chemotherapy for osteosarcoma (NECO) 95-J protocol
(8). When the neoadjuvant
chemotherapy was completed, the response to chemotherapy was
evaluated using MRI, CT and plain radiography and a partial
response was observed.
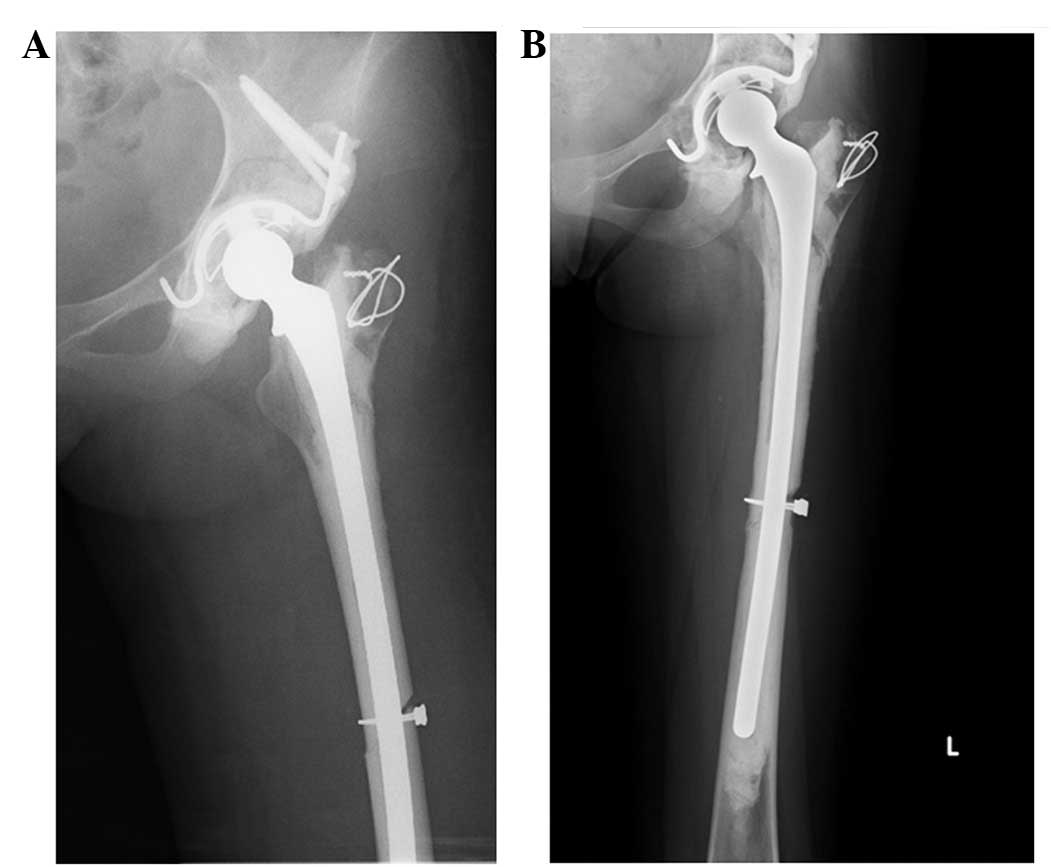
The patient subsequently underwent a wide resection
and reconstruction using a pasteurized autograft-prosthesis
composite, as described later in this study (Fig. 6). The histopathological response to
chemotherapy was grade IV according to the criteria of Rosen et
al(9). The patient was
administered adjuvant chemotherapy, as above. No recurrence or
metastases were identified during a follow-up period of three
years. Radiography revealed a partial union of the medial junction
of the distal femur after 1 year (Fig.
6). The functional score, according to the study by Enneking
et al(10), was 92%. The
patient showed a slight Trendelenburg gait due to disorder of the
gluteus medius muscle.
Surgical technique
The patient was placed in a lateral position. A long
posterolateral incision was made to contain the biopsy scar and all
the potentially contaminated areas that were included in the scars
from the drains. Contaminated areas, including the subcutaneous
tissue, iliotibial band and vastus lateralis muscle, were resected
and an adequate wide resection of the bone was performed. The
distal femur was resected 5 cm away from the tip of the CHS plate.
The pelvis was resected according to the rotational acetabular
osteotomy (RAO) technique described previously (11). Briefly, the osteotomy was performed
using a specially curved osteotome that was designed to
approximately correspond to the circumferential curvature of the
acetabulum. The line of the osteotomy followed the proximal side of
attachment of the capsule to the pelvis. The osteotomy was carried
out anteriorly and posteriorly around the circumference of the
acetabulum, with the osteotome being allowed to follow its own
curve. En bloc resection of the hip joint was performed without
breaking the capsule (Fig. 7).
Pasteurization of the resected tissue was then performed (12). Briefly, the bone was heated in
physiological saline at 65°C for 30 min following curettage of the
tumor tissue and intramedullary reaming. The capsule of the hip
joint was removed from the bone. The acetabular cartilage was
removed from the pasteurized bone using curets and careful reaming,
with an attempt to leave the subchondral bone of the acetabulum
intact. The pasteurized acetabulum was fixed to the ilium, ischium
and pubic bone using a SuperFIXSORB screw (Takiron Co., Osaka,
Japan). For further reinforcement of the acetabulum, a
Kerboull-type (KT) plate (Japan Medical Materials Corp., Osaka,
Japan) was installed. Following the fixation of the graft to the
host bone, the pasteurized acetabulum was resurfaced with a
polyethylene cup that was cemented in place. The distal side of the
pasteurized femur was fixed with wire. Conventional cemented total
hip arthroplasty (THA; Stryker Japan, Co.) was performed using an
Omnifit Cemented Long Stem. To prevent infection, the bone cement
was mixed with antibiotics. Every 40 g of cement contained 1 g
vancomycin hydrochloride and 400 mg amikacin sulfate.
Discussion
In OS, the presence of a pathological fracture at
the time of diagnosis (5–10% of all cases) is associated with a
poor outcome (13). This may be due
to fact that the fracture causes a local hematoma, which
facilitates the dissemination of the tumor. Therefore, the presence
of a pathological fracture has been considered a contraindication
for limb salvage and an indication for an immediate amputation
(14). However, studies have
suggested that limb salvage surgery for a pathological fracture, if
combined with adjuvant chemotherapy, does not increase the risk of
local recurrence (15) and does not
decrease overall survival compared with amputation (16). In the present study, a pathological
femoral neck fracture was recognized and dissemination was limited
to the space within the capsule.
In the present study, a periosteal reaction, which
is a characteristic finding in OS, was not recognized at the time
of the initial consultation, as the main lesion was located in the
intra-articular area and not in the periosteum. Furthermore, the
imaging findings were consistent with a differential diagnosis of a
benign bone tumor, including a solitary bone cyst and fibrous
dysplasia. The examination of the intraoperative frozen section
showed features of a fibrous benign tumor, probably due to crush
artifacts. Therefore, tumor curettage, HA transplantation and
osteosynthesis by CHS were performed during the first surgery. This
scenario illustrates the limitations of the initial diagnostic
measures. However, even when a diagnosis of OS is made at the first
surgery, osteosynthesis using a screw may be required to prevent
displacement.
In the present case, a resection of the
extra-articular hip joint, femoral neck and pubic rami, i.e., a
type II resection according to the principles outlined by Enneking
et al(17) and Bickels and
Malawer (18), was adequate.
Although several methods for reconstruction following resection
have been reported, including pelvic prosthesis arthroplasty
(19–21), allograft reconstruction (with or
without a total hip prosthesis) (22–25),
arthrodesis and pseudarthrosis, a ‘gold standard’ has yet to be
established due to poor post-operative function and high
complication rates. Regardless of the methods that are used,
infection and dislocation are common post-operative complications.
Infection rates range from 18–33% in saddle prosthesis arthroplasty
(19–21) and 8–60% in allograft reconstruction
(with or without a total hip prosthesis) (22–25).
Pasteurization is a method of autograft recycling in
which extracorporeal heating of the tumor-bearing bone segment is
followed by its reimplantation (26,27).
This strategy is a well-established method of reconstruction in
certain countries, particularly in Asia and Africa. It is a simple,
easily accessible and economical alternative to the usual
reconstructive modalities, with comparable and acceptable
functional outcomes and complication rates, in addition to its
social and religious acceptance in these countries (26,27).
However, a variety of complications associated with pasteurized
autografts have been described, including graft fracture, collapse,
infection, delayed or non-union of the junction and mechanical
implant failure (28,29). Although the present patient had a
favorable clinical course, longer term follow-up is necessary.
Acknowledgements
This study was supported in part by Grants-in-Aid
for Scientific Research (C) 24592227 (KAKENHI). The authors would
like to thank Akemi Sano for providing excellent technical
assistance.
References
|
1
|
Ferrari S and Palmerini E: Adjuvant and
neoadjuvant combination chemotherapy for osteogenic sarcoma. Curr
Opin Oncol. 19:341–346. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wittig JC, Bickels J, Priebat D, Jelinek
J, Kellar-Graney K, Shmookler B and Malawer MM: Osteosarcoma: a
multidisciplinary approach to diagnosis and treatment. Am Fam
Physician. 65:1123–1132. 2002.PubMed/NCBI
|
|
3
|
Bacci G and Lari S: Current treatment of
high grade osteosarcoma of the extremity: review. J Chemother.
13:235–243. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Unni KK, Inwards CY, Bridge JA, Kindblom
LG and Wold LE: Chondromyxoid fibroma. AFIP Atlas of Tumor
Pathology, Tumor of the Bones and Joints. Silverberg SG and Sobin
LH: ARP Press; Silver Spring, MD, USA: pp. 67–73. 2005
|
|
5
|
Raymond AK, Ayala AG and Knuutila S:
Conventional osteosarcoma. World Health Organization classification
of tumours, pathology and genetics of tumours of soft tissue and
bone. Fletcher CDM, Unni KK and Mertens F: IARC Press; Lyon,
France: pp. 264–270. 2002
|
|
6
|
O'Hara JM, Hutter RV, Foote FW Jr, Miller
T and Woodard HQ: An analysis of thirty patients surviving longer
than ten years after treatment for osteogenic sarcoma. J Bone Joint
Surg Am. 50:335–354. 1968.PubMed/NCBI
|
|
7
|
Gebert C, Wessling M, Hoffmann C, et al:
Hip transposition as a limb salvage procedure following the
resection of periacetabular tumors. J Surg Oncol. 103:269–275.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Iwamoto Y, Tanaka K, Isu K, et al:
Multiinstitutional phase II study of neoadjuvant chemotherapy for
osteosarcoma (NECO study) in Japan: NECO-93J and NECO-95J. J Orthop
Sci. 14:397–404. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rosen G, Caparros B, Huvos AG, et al:
Preoperative chemotherapy for osteogenic sarcoma: selection of
postoperative adjuvant chemotherapy based on the response of the
primary tumor to preoperative chemotherapy. Cancer. 49:1221–1230.
1982. View Article : Google Scholar
|
|
10
|
Enneking WF, Dunham W, Gebhardt MC,
Malawar M and Pritchard DJ: A system for the functional evaluation
of reconstructive procedures after surgical treatment of tumors of
the musculoskeletal system. Clin Orthop Relat Res. 286:241–246.
1993.PubMed/NCBI
|
|
11
|
Ninomiya S and Tagawa H: Rotational
acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am.
66:430–436. 1984.PubMed/NCBI
|
|
12
|
Eid AS, Jeon DG and Cho WH: Can bone
scintigraphy predict the final outcome of pasteurized autografts?
Skeletal Radiol. 39:1009–1016. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ferguson PC, McLaughlin CE, Griffin AM,
Bell RS, Deheshi BM and Wunder JS: Clinical and functional outcomes
of patients with a pathologic fracture in high-grade osteosarcoma.
J Surg Oncol. 102:120–124. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jaffe N, Spears R, Eftekhari F, et al:
Pathologic fracture in osteosarcoma. Impact of chemotherapy on
primary tumor and survival. Cancer. 59:701–709. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Natarajan MV, Govardhan RH, Williams S and
Raja Gopal TS: Limb salvage surgery for pathological fractures in
osteosarcoma. Int Orthop. 24:170–172. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bacci G, Ferrari S, Longhi A, et al:
Nonmetastatic osteosarcoma of the extremity with pathologic
fracture at presentation: local and systemic control by amputation
or limb salvage after preoperative chemotherapy. Acta Orthop Scand.
74:449–454. 2003. View Article : Google Scholar
|
|
17
|
Enneking WF, Spanier SS and Malawer MM:
The effect of the Anatomic setting on the results of surgical
procedures for soft parts sarcoma of the thigh. Cancer.
47:1005–1022. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bickels J and Malawer MM: Overview of
pelvic resections: surgical considerations and classification.
Musculoskeletal Cancer Surgery. Malawer MM and Sugarbacker PH:
Kluwer Academic Publishers; Dordrecht, The Netherlands: pp.
203–213. 2001
|
|
19
|
Renard AJ, Veth RP, Schreuder HW, et al:
The saddle prosthesis in pelvic primary and secondary
musculoskeletal tumors: functional results at several postoperative
intervals. Arch Orthop Trauma Surg. 120:188–194. 2000. View Article : Google Scholar
|
|
20
|
Cottias P, Jeanrot C, Vinh TS, Tomeno B
and Anract P: Complications and functional evaluation of 17 saddle
prostheses for resection of periacetabular tumors. J Surg Oncol.
78:90–100. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Natarajan MV, Bose JC, Mazhavan V,
Rajagopal TS and Selvam K: The Saddle prosthesis in periacetabular
tumours. Int Orthop. 25:107–109. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bell RS, Davis AM, Wunder JS, Buconjic T,
McGoveran B and Gross AE: Allograft reconstruction of the
acetabulum after resection of stage-IIB sarcoma. Intermediate-term
results. J Bone Joint Surg Am. 79:1663–1674. 1997.PubMed/NCBI
|
|
23
|
Langlais F, Lambotte JC and Thomazeau H:
Long-term results of hemipelvis reconstruction with allografts.
Clin Orthop Relat Res. 388:178–186. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ozaki T, Hillmann A, Bettin D, Wuisman P
and Winkelmann W: High complication rates with pelvic allografts.
Experience of 22 sarcoma resections. Acta Orthop Scand. 67:333–338.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Yoshida Y, Osaka S and Mankin HJ:
Hemipelvic allograft reconstruction after periacetabular bone tumor
resection. J Orthop Sci. 5:198–204. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Manabe J, Ahmed AR, Kawaguchi N, Matsumoto
S and Kuroda H: Pasteurized autologous bone graft in surgery for
bone and soft tissue sarcoma. Clin Orthop Relat Res. 419:258–266.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sakayama K, Kidani T, Fujibuchi T,
Kamogawa J, Yamamoto H and Shibata T: Reconstruction surgery for
patients with musculoskeletal tumor, using a pasteurized autogenous
bone graft. Int J Clin Oncol. 9:167–173. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ahmed AR, Manabe J, Kawaguchi N, Matsumoto
S and Matsushita Y: Radiographic analysis of pasteurized autologous
bone graft. Skeletal Radiol. 32:454–461. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jeon DG, Kim MS, Cho WH, Song WS and Lee
SY: Reconstruction with pasteurized autograft-total hip prosthesis
composite for periacetabular tumors. J Surg Oncol. 96:493–502.
2007. View Article : Google Scholar : PubMed/NCBI
|