Introduction
Carcinoid tumors of the ovary are uncommon
neoplasms. A carcinoid tumor is defined as a slow-growing
neuroendocrine tumor that usually appears in the gastrointestinal
tract. The unique complications derived from the secretion of
serotonin are known as carcinoid syndrome, characterized by facial
flushing, diarrhea, abdominal cramping, bronchoconstriction and
heart failure (1–3). Primary carcinoid tumors of the ovary
were first described by Stewart et al in 1939 and constitute
0.5–5% of all carcinoid tumors and <0.1% of all ovarian
malignancies (4–7). Although the majority of ovarian
carcinoid tumors are diagnosed at an early stage and are generally
cured with surgical removal alone, specific cases have been
reported to undergo recurrence following a number of years
(8). The present study reports a
case of recurrent carcinoid tumor of the ovary presenting typical
features of carcinoid heart disease 13-years after the primary
surgery.
Case report
A 67-year-old female was referred to Kyoto
University Hospital with a diagnosis of a paraaortic mass,
identified by an ultrasound at an internal medicine clinic. This
study was approved by the ethics committee of Kyoto University,
Kyoto, Japan. Informed consent was obtained from the patient.
At 54 years old, the patient visited a gynecology
clinic with complaints of lower abdominal distention and pain. An
ultrasound identified a left ovarian tumor. Laboratory tests
revealed elevated serum CA125 (95 IU/ml) levels and normal CEA and
CA19-9. The patient was also diagnosed with heart failure. The
individual underwent a total abdominal hysterectomy and bilateral
salpingo-oophorectomy. The pathological diagnosis was of a
trabecular carcinoid tumor of the left ovary with positive ascites
cytology. The patient then underwent one cycle of intraperitoneal
chemotherapy and three cycles of systemic chemotherapy (detailed
information on the treatment was not available). The post-operative
serum levels of serotonin and urinary 5-hydroxyindole acetate
(5-HIAA) were normal. The heart failure was diagnosed as heart
carcinoid disease. The patient was treated with medication
prescribed by the cardiology department and ceased attending any
gynecology appointments.
At 67 years old, an abnormal paraaortic tumor was
identified by ultrasound screening at an internal medicine clinic,
at which point the patient was referred to hospital. The patient
did not complain of any typical carcinoid syndrome symptoms, which
include skin flushes, diarrhea, abdominal cramping, peripheral
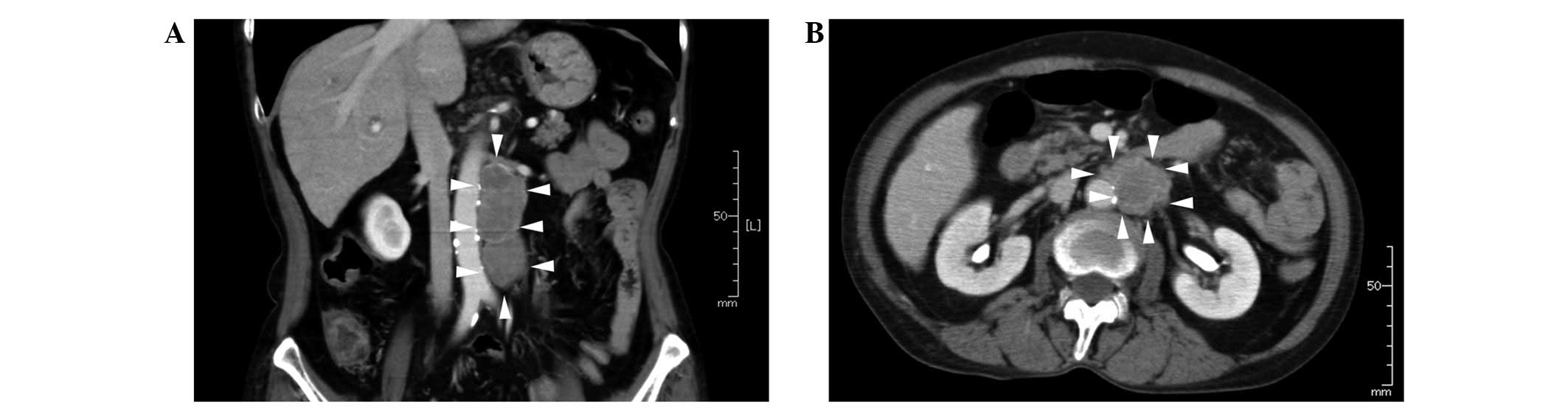
edema or tachycardia. A computed tomography (CT) examination
revealed a solitary tumor 30×30×77 mm in size in the paraaortic
area (Fig. 1), while there were no
abnormal observations in the pelvic cavity. Laboratory tests
revealed normal serum CA125, CEA and CA19-9 levels, but the urinary
5-HIAA level was elevated to 27.5 mg/l. Consequently, the mass was
diagnosed as a recurrence of an ovarian carcinoid tumor.
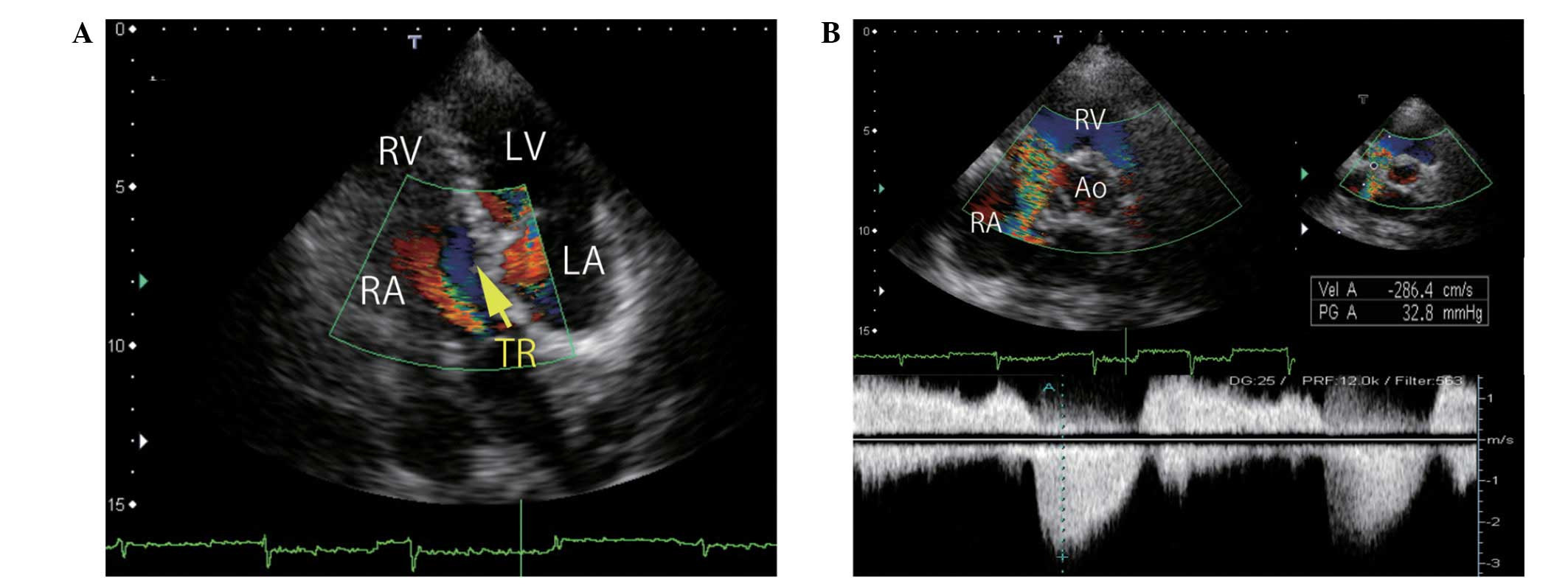
Echocardiographic imaging revealed severe tricuspid regurgitation
(Fig. 2) and mild aortic
regurgitation with a pressure half-time of 655 ms. The ejection
fraction was 66.5%.
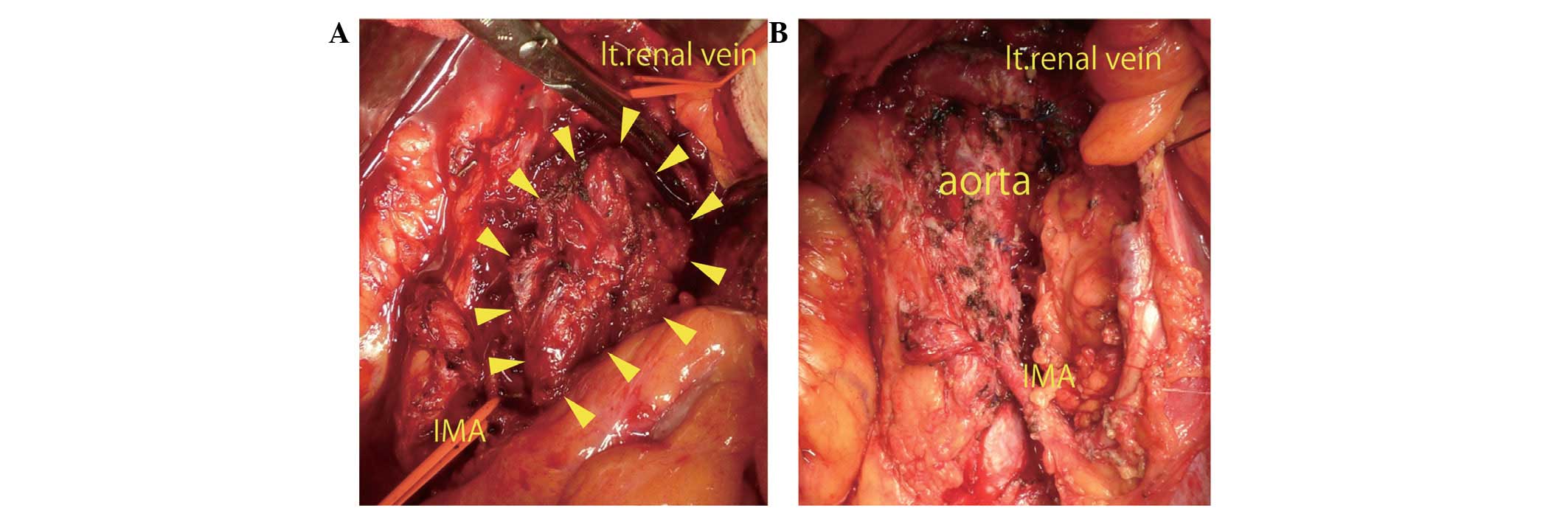
Neither chemotherapy nor radiation is considered to
be an effective for treating carcinoid tumors. Although the patient
in this case had carcinoid heart disease, a surgical resection was
performed (Fig. 3) based on the
recommendations of a cardiologist who confirmed that the cardiac
function would tolerate the surgery. The surgery lasted 8 h and 43
min and the total blood loss was 3,930 ml. A transfusion of 400 ml
autologous blood, 6 units MAP, 8 units FFP and 20 units platelets
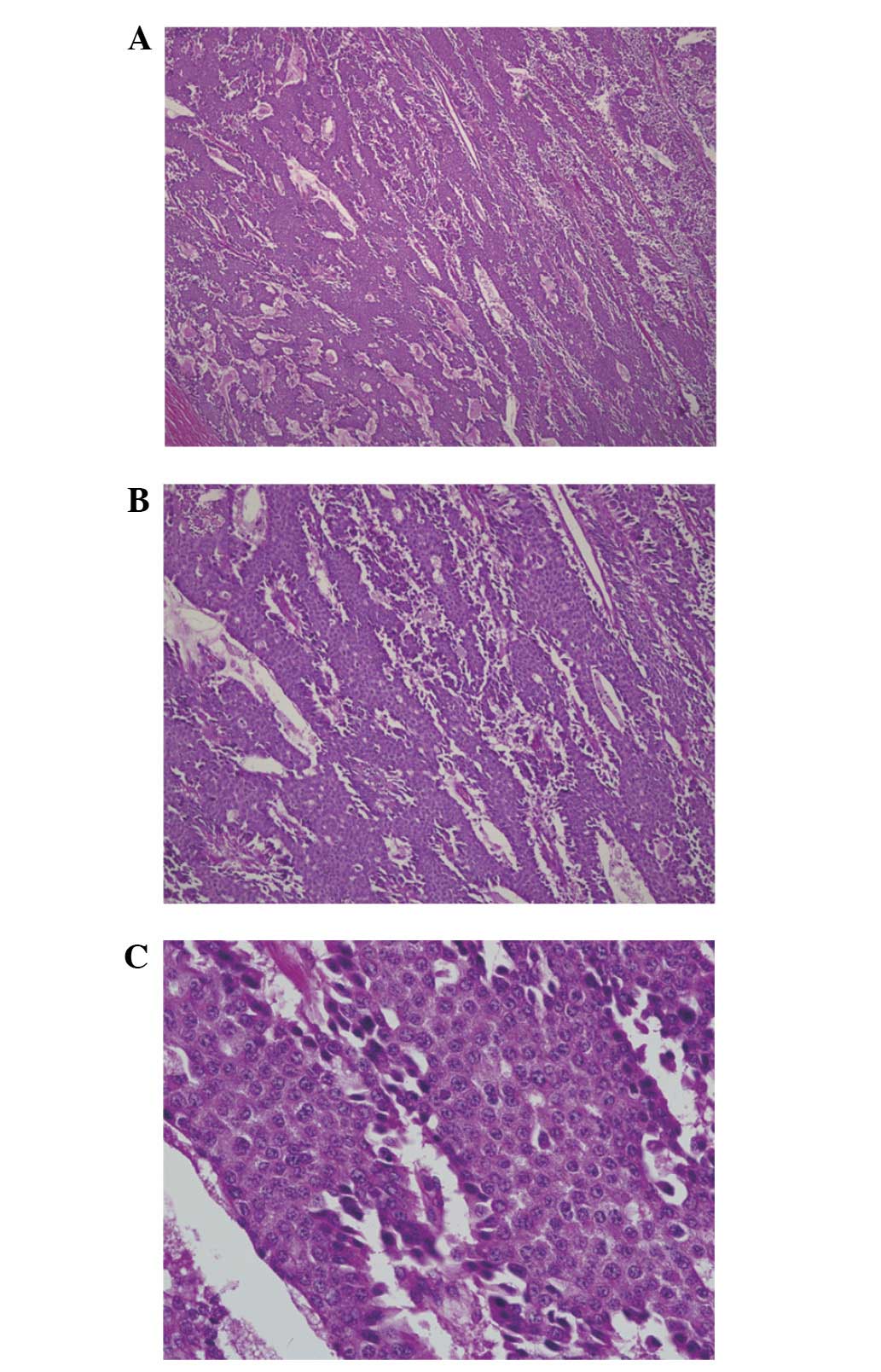
was necessary. The histological diagnosis was that of a diffuse
carcinoid tumor metastatic to the lymph nodes. The carcinoid tumor
was characterized as trabecular or insular in type (Figs. 4 and 5). The patient recovered without any
serious complications and was discharged 33 days after the surgery.
No further treatment was administered.
Discussion
Primary carcinoid tumors of the ovary are rare and
constitute 0.5–5% of all carcinoid tumors and <0.1% of all
ovarian malignancies (5–7). The histology of primary ovarian
carcinoids is classified as insular, trabecular, strumal or
mucinous carcinoid. The insular type often produces a large amount
of serotonin and causes carcinoid syndrome, which is characterized
by flushing of the skin, diarrhea and abdominal pain. More rarely,
carcinoid syndrome presents as heart failure and
bronchoconstriction (1,2).
The most common types of carcinoid tumors are
derived from the intestines and seldom cause carcinoid syndrome
since liver enzymes rapidly inactivate the vasoactive substances
produced by the tumor (1,9). By contrast, primary ovarian carcinoid
tumors release serotonin or other vasoactive substances directly
into the systemic circulation and readily cause carcinoid syndrome,
including carcinoid heart disease (?). Chaowalit et al
previously reported 4 cases of ovarian carcinoid, which presented
signs of right-sided heart failure and required surgical
replacement of the valve on the right side (9). In patients with primary ovarian
carcinoid tumors, ~1/3 may develop carcinoid heart disease at an
early stage without evidence of metastasis. Generally, the heart
failure caused by a carcinoid tumor is characterized by isolated,
severe tricuspid regurgitation without significant left-sided valve
dysfunction (10–12). In this case, the patient suffered
from carcinoid heart disease, although the patient did not require
surgical treatment. Therefore, the recurrence of the carcinoid
tumor, with increased levels of serum serotonin, may have further
impaired the patient’s cardiac function, which was one of the
reasons for selecting a surgical resection of the tumor.
Following the primary treatment, the patient did not
receive regular follow-ups with a gynecologist concerning the
carcinoid tumor. However, patients with carcinoid tumors, and
particularly those with cardiac dysfunction, should see a
gynecologist and a cardiologist for the early detection of any
possible recurrence. No effective treatment exists for carcinoid
tumors, with the exception of surgical resection. Therefore, it is
particularly important to detect recurrence early to ensure that
surgical removal is viable and that the heart function is able to
tolerate the surgery. Urinary 5-HIAA is the most reliable follow-up
marker of serotonin producing-carcinoid tumors. van der
Horst-Schrivers et al reported that persistently low urinary
5-HIAA (<20 mmol/mol creatinine) levels is a marker of a
favorable survival rate (13–15).
However, for detection, 5-HIAA is not as sensitive a tumor marker
(specificity, 100% and sensitivity, 35%) as other markers, for
example, chromogranin A (specificity, 86% and sensitivity, 68%)
(16). In the case of patients who
have abnormal echocardiography results at diagnosis,
echocardiography every 6 months is recommended (17). In addition to the use of markers,
examinations using CT scans and/or magnetic resonance imaging (MRI)
is effective. It has been reported that a CT scan has 75%
sensitivity and 99% specificity, while an MRI has 89% sensitivity
and 100% specificity for abdominal tumor dissemination (18). Octoreotide single-photon emission
computed tomography (SPECT)/CT has also been reported to be useful
for detecting the metastasis or recurrence of carcinoid tumors
(14). In this case, the patient
was at a high risk of recurrence as the ascites cytology at the
first surgery was positive. However, recurrence did not occur until
13 years post-surgery. In cases with a high risk of recurrence,
particularly in patients with carcinoid syndrome at diagnosis,
careful follow-up examinations must be continued for an extended
period of time.
References
|
1
|
Fox DJ and Khattar RS: Carcinoid heart
disease: presentation, diagnosis, and management. Heart.
90:1224–1228. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Palaniswamy C, Frishman WH and Aronow WS:
Carcinoid heart disease. Cardiol Rev. 20:167–176. 2012. View Article : Google Scholar
|
|
3
|
Lundin L, Norheim I, Landelius J, Oberg K
and Theodorsson-Norheim E: Carcinoid heart disease: relationship of
circulating vasoactive substances to ultrasound-detectable cardiac
abnormalities. Circulation. 77:264–269. 1988. View Article : Google Scholar
|
|
4
|
Stewart MJ, Willis RA and De Saram GS:
Argentaffine carcinoma (carcinoid tumour) arising in ovarian
teratomas: A report of two cases. J Pathol Bacteriol. 49:207–212.
1939. View Article : Google Scholar
|
|
5
|
Bai X, Li N, Wang F, Li S and Yu Q:
Primary ovarian trabecular carcinoid tumor: a case report and
literature review. Arch Gynecol Obstet. 282:407–411. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Talerman A: Carcinoid tumors of the ovary.
J Cancer Res Clin Oncol. 107:125–135. 1984. View Article : Google Scholar
|
|
7
|
Díaz-Montes TP, Rosenthal LE, Bristow RE
and Grumbine FC: Primary insular carcinoid of the ovary. Gynecol
Oncol. 101:175–178. 2006.
|
|
8
|
Timmins PF, Kuo DY, Anderson PS, Fields
AL, Whitney KD and Goldberg GL: Ovarian carcinoid: management of
primary and recurrent tumors. Gynecol Oncol. 76:112–114. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chaowalit N, Connolly HM, Schaff HV, Webb
MJ and Pellikka PA: Carcinoid heart disease associated with primary
ovarian carcinoid tumor. Am J Cardiol. 93:1314–1315. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Moerman VM, Dewilde D and Hermans K:
Carcinoid heart disease: typical findings on echocardiography and
cardiac magnetic resonance. Acta Cardiol. 67:245–248.
2012.PubMed/NCBI
|
|
11
|
Garg S, Bourantas CV, Nair RK and Alamgir
F: Carcinoid syndrome diagnosed by echocardiography. Int J Cardiol.
147:e1–e3. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hong SN, Saric M and Kronzon I: Carcinoid
heart disease. J Am Coll Cardiol. 55:19962010. View Article : Google Scholar
|
|
13
|
van der Horst-Schrivers AN, Post WJ, et
al: Persistent low urinary excretion of 5-HIAA is a marker for
favourable survival during follow-up in patients with disseminated
midgut carcinoid tumours. Eur J Cancer. 43:2651–2657.
2007.PubMed/NCBI
|
|
14
|
Robiolio PA, Rigolin VH, Wilson JS, et al:
Carcinoid heart disease. Correlation of high serotonin levels with
valvular abnormalities detected by cardiac catheterization and
echocardiography. Circulation. 92:790–795. 1995. View Article : Google Scholar
|
|
15
|
Buda A, Giuliani D, Montano N, Perego P
and Milani R: Primary insular carcinoid of the ovary with carcinoid
heart disease: Unfavourable outcome of a case. Int J Surg Case Rep.
3:59–61. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Seregni E, Ferrari L, Bajetta E,
Martinetti A and Bombardieri E: Clinical significance of blood
chromogranin A measurement in neuroendocrine tumours. Ann Oncol.
12(Suppl 2): S69–S72. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Klöppel G, Couvelard A, Perren A, et al:
ENETS consensus guidelines for the standards of care in
neuroendocrine tumors: towards a standardized approach to the
diagnosis of gastroenteropancreatic neuroendocrine tumors and their
prognostic stratification. Neuroendocrinology. 90:162–166.
2009.
|
|
18
|
Sundin A, Vullierme MP, Kaltsas G and
Plöckinger U: Mallorca Consensus Conference participants; European
Neuroendocrine Tumor Society: ENETS consensus guidelines for the
standards of care in neuroendocrine tumors: radiological
examinations. Neuroendocrinology. 90:167–183. 2009. View Article : Google Scholar
|