Introduction
Gastric cancer is the second leading cause of
cancer-related mortality worldwide (1,2). The
various clinical manifestations in certain patients make the
diagnosis difficult and indicate a poor prognosis. Although
gastrointestinal obstructions are not uncommon in gastric cancer
(3–5), observing a large bowel obstruction as
the first manifestation of the disease is rare. The present study
describes a case of gastric cancer in a patient who presented with
abdominal pain and an acute large bowel obstruction. To the best of
our knowledge, the present study is the first in the literature to
describe an initial manifestation of a large bowel obstruction
associated with gastric cancer. Written informed consent was
obtained from the patient.
Case report
A 59-year-old female without no significant medical
history visited Linan People’s Hospital (Hangzhou, China)
complaining of central abdominal pain and not being able to
defecate for 15 days. Although the patient had been admitted to
Hangzhou Provincial Hospital due to recurrent abdominal pain six
months previously, the colon was not considered abnormal following
a colonoscopy and ultrasound. A gastroscopy only revealed chronic
superficial gastritis (data not shown). Upon admittance to the
Department of Surgery, the right epigastric region was slightly
tender and active bowel sounds were identified, followed by
intermittent bilious vomiting and weight loss, despite a distended
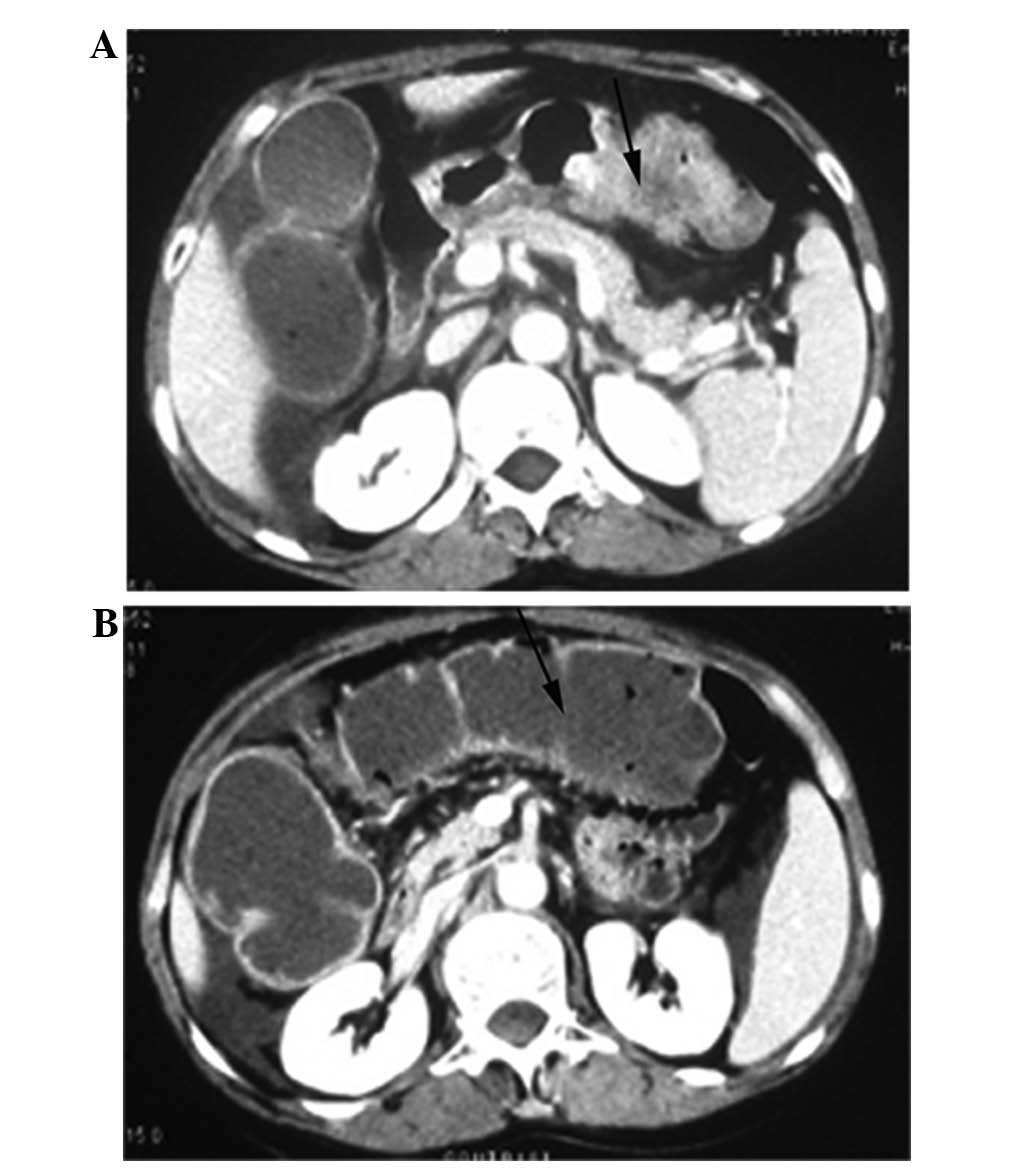
abdomen without rebound pain or hepatomegaly. Computed tomography
(CT) of the abdomen revealed a dilated fluid-filled colon and a
protruding tumor abutting the transverse colon. No other
abnormalities/metastases to the liver or the involvement of
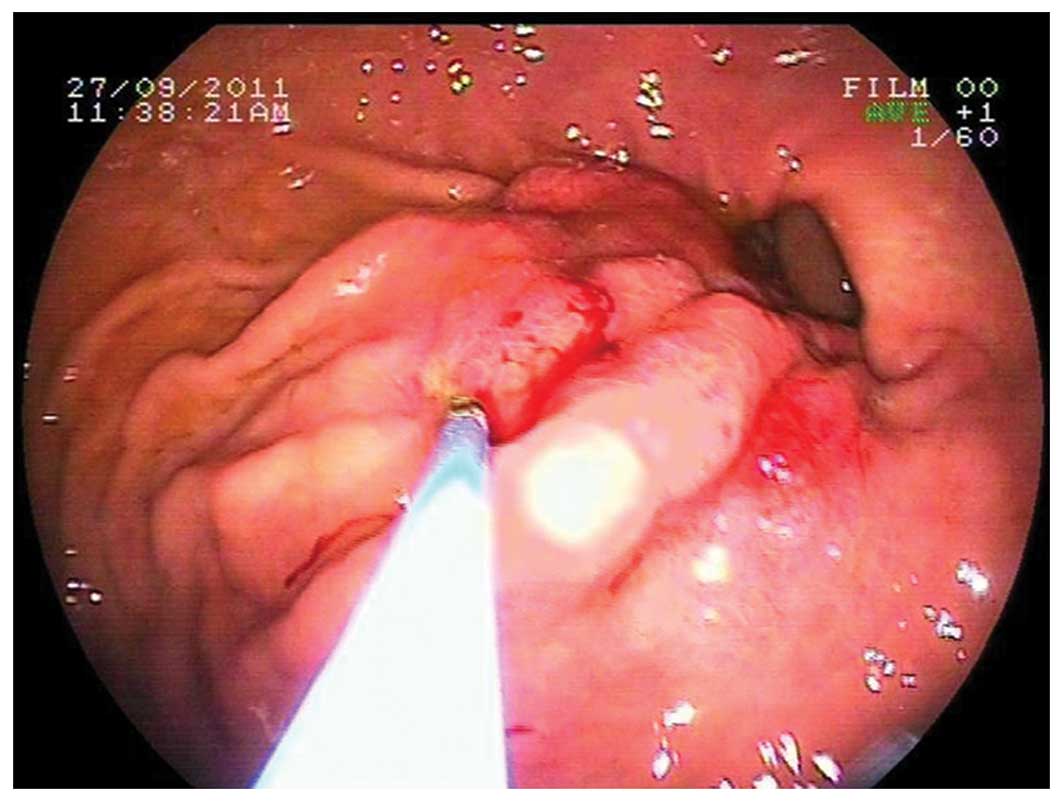
adjacent organs/tissues were observed (Fig. 1). An upper gastrointestinal
endoscopy revealed the existence of a raised margin and thickening
of the gastric mucosal in the antrum, with no evidence of
ulcerative lesions (Fig. 2). The
endoscopic gastric biopsies indicated a diagnosis of a
poorly-differentiated adenocarcinoma. The routine blood test
results were normal, with the exception of an elevated CA19-9 level
(95 U/l; normal range, <39 U/l).
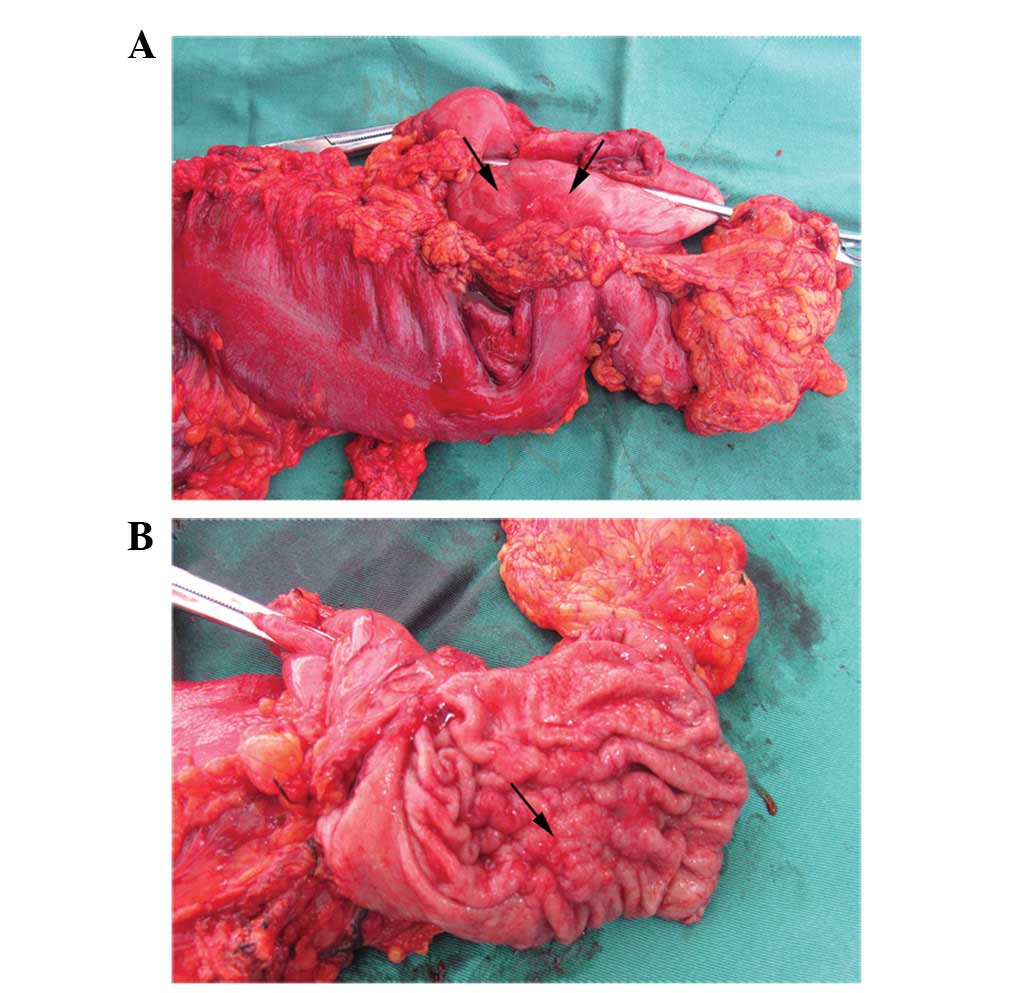
The patient underwent a radical distal gastrectomy
with systematic lymph node dissection and a right colectomy
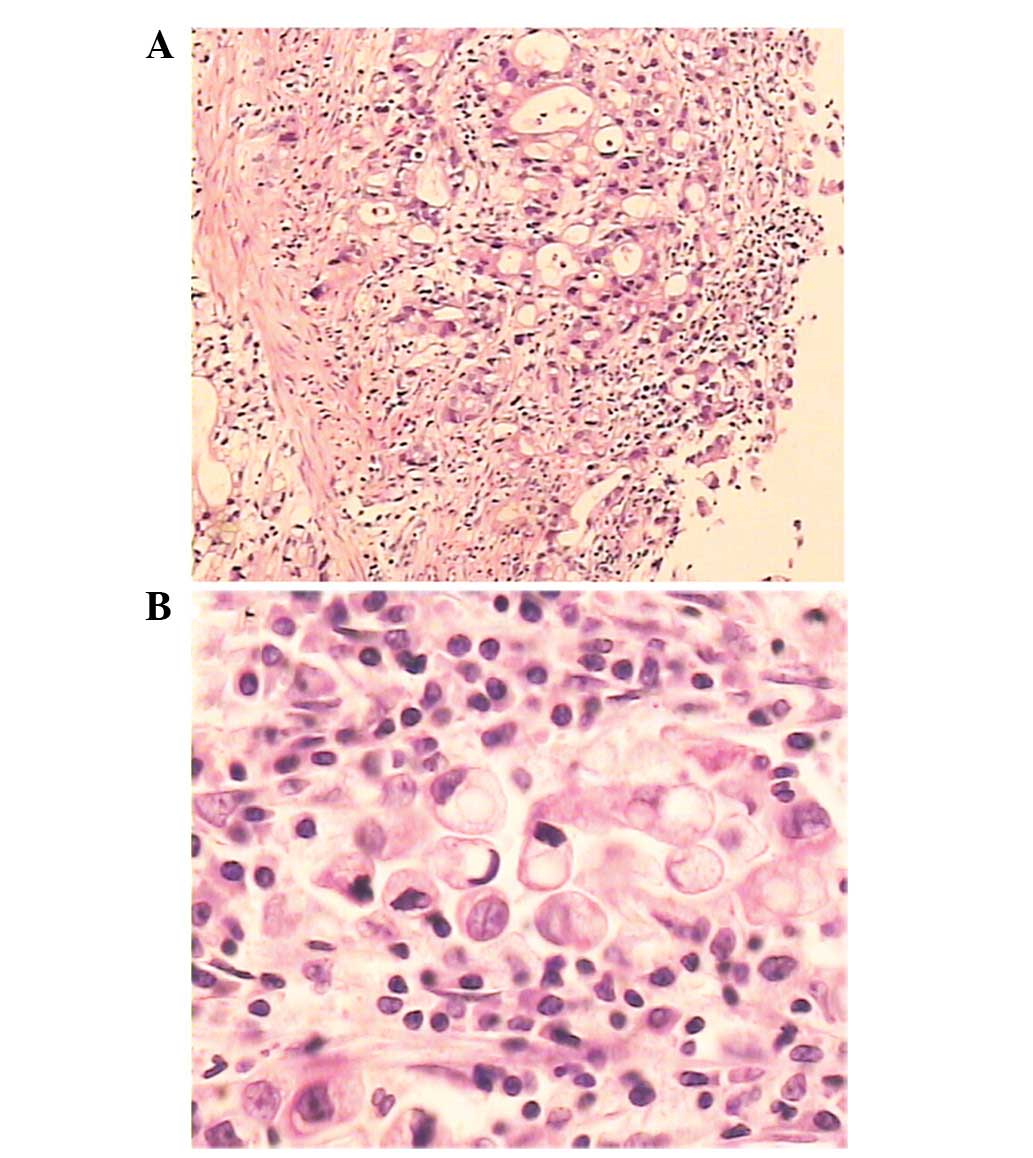
(Fig. 3). The histology of the
specimens indicated a poorly-differentiated adenocarcinoma with the
presence of signet cells and cancer invasion to the transverse
colonic mucosa (pT4; Fig. 4). No
perigastric lymph node metastases were identified (0/15, pN0). The
patient is currently doing well without recurrence at 18 months
post-surgery.
Discussion
Although highly advanced stage gastric cancer often
causes gastric outlet obstruction and results in gastrointestinal
symptoms, including abdominal pain, nausea and vomiting, an acute
large bowel obstruction as the first presentation of gastric cancer
is a rare event. The main route of cancer infiltrating the
abdominal organs is known as the diffusion of the adjacent tissues
and the invasion of the superficial serosal layer (6). In the present study, the wall of the
transverse colon was thickened on the CT and a
poorly-differentiated adenocarcinoma was confirmed by the histology
examination, revealing the true invasion from the primary gastric
cancer. Gastroscopy indicated that the gastric mucosa was partly
raised and the distant organs did not contain any lesions. However,
the cancer cells invaded the adjacent tissues, suggesting that the
biological behavior of cancer cells and the performance and
progress of gastric cancer may vary.
The poor prognosis of gastric cancer is mainly due
to a late diagnosis (7). Therefore,
an early diagnosis of the disease is the most significant factor in
order to improve the results of treatment. However, an early
diagnosis is difficult if a lesion is not identified in the stomach
by a gastroscopy examination in the early stages. In certain cases,
the diagnosis also relies on a combination of CT, magnifying
endoscopy or endoscopic ultrasound techniques to analyze the
symptoms, which are now the most common methods for detecting
gastrointestinal invasion from gastric adenocarcinoma (8–11). The
disease often characteristically manifests with a wall thickening
detected by a helical CT. In the present case, the patient
experienced abdomen pain, which may be associated with the
oppression of the gastrointestinal tract due to cancer. The present
study serves to illustrate the significance of a careful
examination in all patients who present with symptoms of abdominal
pain.
References
|
1
|
Hartgrink HH, Jansen EP, van Grieken NC
and van de Velde CJ: Gastric cancer. Lancet. 374:477–490. 2009.
View Article : Google Scholar
|
|
2
|
Fernández-Fernández FJ and Sesma P:
Gastric cancer. Lancet. 374:1594–1595. 2009.
|
|
3
|
Tomikashi K, Mitsufuji S, Kanemasa H,
Sakai M, Wakabayashi N and Tsuchihashi Y: Gastric cancer metastatic
to the colon. Gastrointest Endosc. 55:5612002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kumagai K, Saikawa Y, Fukuda K, et al:
Octreotide acetate successfully treated a bowel obstruction caused
by peritoneally disseminated gastric cancer, thereby enabling the
subsequent use of oral S-1 chemotherapy. Int J Clin Oncol.
14:372–375. 2009. View Article : Google Scholar
|
|
5
|
Fukuda Y, Fujio N, Ihara T, et al: A case
of advanced gastric cancer with direct invasion of the transverse
colon responding to paclitaxel/5′-DFUR combined therapy. Gan To
Kagaku Ryoho. 32:1945–1948. 2005.In Japanese.
|
|
6
|
Feczko PJ, Collins DD and Mezwa DG:
Metastatic disease involving the gastrointestinal tract. Radiol
Clin North Am. 31:1359–1373. 1993.PubMed/NCBI
|
|
7
|
Power DG, Kelsen DP and Shah MA: Advanced
gastric cancer - slow but steady progress. Cancer Treat Rev.
36:384–392. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yin XD, Huang WB, Lü CY, Zhang L, Wang LW
and Xie GH: A preliminary study on correlations of triple-phase
multi-slice CT scan with histological differentiation and
intratumoral microvascular/lymphatic invasion in gastric cancer.
Chin Med J (Engl). 124:347–351. 2011.
|
|
9
|
Oh JY, Cho JH, Kang MJ, et al: CT
findings. Clin Radiol. 66:966–973. 2011. View Article : Google Scholar
|
|
10
|
Kaise M, Kato M and Tajiri H:
High-definition endoscopy and magnifying endoscopy combined with
narrow band imaging in gastric cancer. Gastroenterol Clin North Am.
39:771–784. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Furukawa K, Miyahara R, Itoh A, et al:
Diagnosis of the invasion depth of gastric cancer using MDCT with
virtual gastroscopy: comparison with staging with endoscopic
ultrasound. AJR Am J Roentgenol. 197:867–875. 2011. View Article : Google Scholar : PubMed/NCBI
|