Introduction
A choriocarcinoma is a highly malignant tumor
arising from the embryonal chorion. Generally, the term refers to
gestational choriocarcinoma, which most commonly occurs with a
hydatidiform mole, spontaneous abortion, ectopic pregnancy or
normal delivery (1).
Choriocarcinoma is a cancer that typically occurs in females in the
chorionic epithelium of the placenta (2) and is rarely seen in males. The
Department of Neurosurgery, Renji Hospital (Shanghai, China)
treated two male patients with non-gestational choriocarcinoma
between 2003 and 2008. One patient was diagnosed with disseminated
brain metastases with an unknown origin and the other patient was
diagnosed with a primary intracranial third ventricle
choriocarcinoma. Written informed consent was obtained from the
patients.
Case reports
Case 1
A 21-year-old male with a two-month history of
dizziness and fever and a one-week history of vomiting and numbness
of the right limbs was admitted to the Renji Hospital (Shanghai
Jiao Tong University School of Medicine, Shanghai, China). The
patient developed symptoms of dizziness and fever two months prior
to being admitted. At that time, the patient was treated in the
local clinic with a course of anti-inflammatory medication. The
symptoms improved, but a mild fever remained. The chest X-ray
indicated nothing unusual at that time. One week prior to
admission, the patient complained of coughing and sputum with
occasional blood streaks, left upper limb pain and numbness of the
right limbs. The patient also vomited frequently. The vomitus
contained gastric contents. A chest X-ray was performed again at
the outpatient department and revealed multiple nodules in the
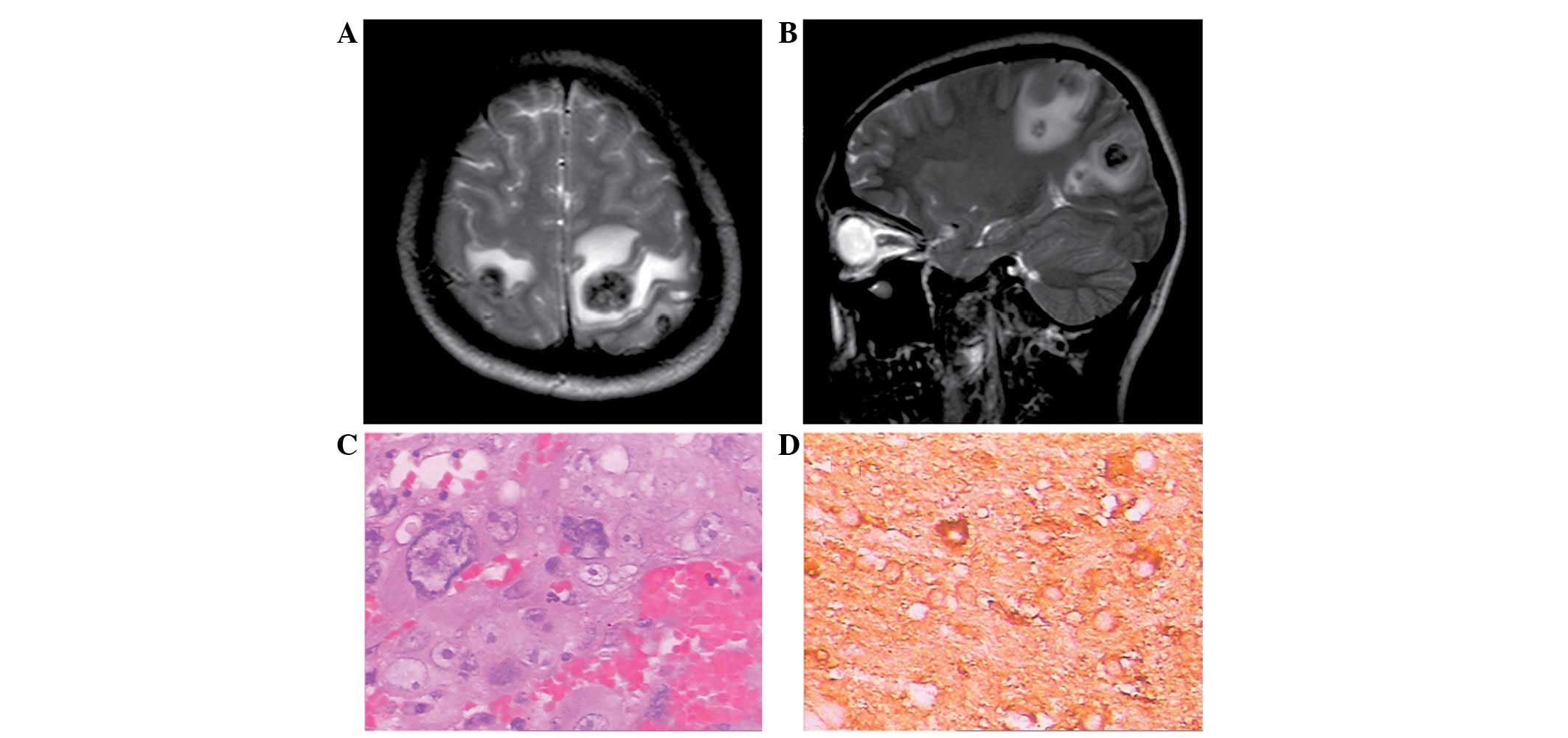
lungs. The brain magnetic resonance imaging (MRI) scans
demonstrated multiple mass lesions occupying the bilateral parietal
and occipital lobes (Fig. 1A and
B). The past history was unremarkable. Upon physical
examination, the patient was identified to be normotensive with a
temperature of 37.8°C. There were no abnormal signs on the nervous
system examination. The superficial lymph nodes were not palpable.
There were no abnormal findings upon physical examination of the
thorax and abdomen. A further abdominal ultrasound detected
hyperechoic masses in the liver and kidneys.
Intracranial surgery for the resection of the
multiple lesions was performed one day after admission. The tumor
appeared dark red with a tough texture and rich blood supply. The
boundary with the normal brain tissue was clear. An intra-operative
biopsy of the mass was sent for frozen section analysis and the
result was that of a metastatic poorly-differentiated cancer.
Following the surgery, the patient gradually developed intracranial
hypertension symptoms, including headaches and projectile vomiting.
The symptoms progressively worsened. On post-operative day seven, a
head computed tomography (CT) scan indicated that new hemorrhagic
metastases had emerged in the frontal and parietal lobes. The
parents of the patient rejected a decompressive craniectomy and
chose a conservative treatment. The pathology report revealed that
the brain tumor was a metastatic choriocarcinoma and the
immunohistochemistry is shown in Fig.
1C and D. The urine was strongly positive for β-human chorionic
gonadotropin (β-hCG) and the serum β-hCG was markedly elevated at
16,500 mIU/ml. The testicles were equal in size and ultrasonography
did not reveal anything abnormal. Following a consultation with the
Department of Oncology, conservative therapy was suggested, since
the patient was too ill for chemotherapy. On the day of the
consultation, the situation deteriorated with unstable vital signs.
Two days later, the patient succumbed to the disease.
Case 2
A 20-year-old male was admitted to the Renji
Hospital due to a sudden onset of unconsciousness, with a six-month
history of nausea and vomiting. The neurological findings were
unremarkable, with the exception of a low level of consciousness. A
head CT scan demonstrated acute hydrocephalus and a mass lesion
occupying the third ventricle.
Emergency surgery for external ventricular drainage
was performed upon admission. Following the surgery, the
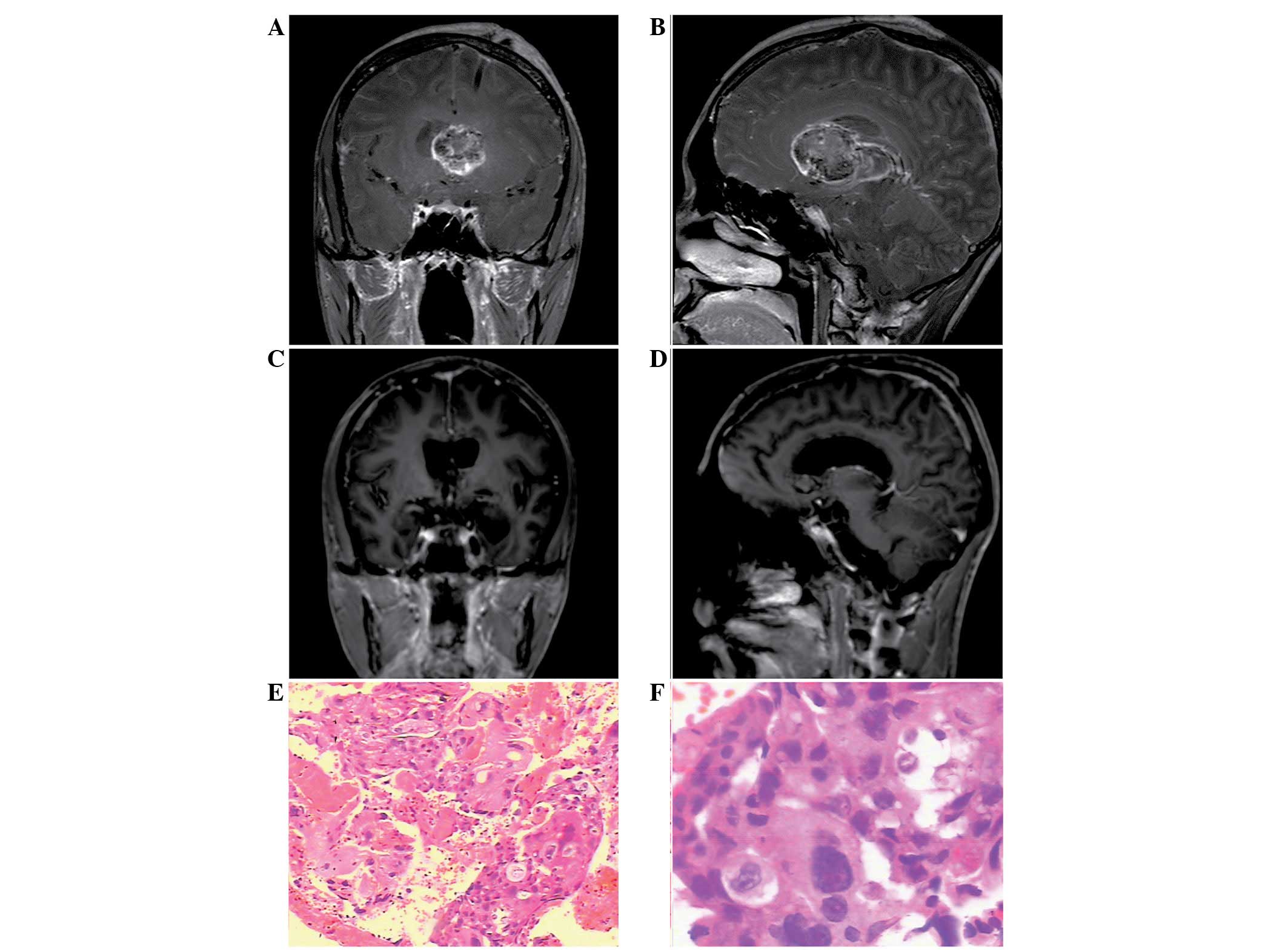
consciousness level improved. A head MRI examination was then
performed and revealed a mass lesion in the ventricle (Fig. 2A and B). The chest X-ray and
abdominal ultrasound revealed nothing unusual. A mass resection
surgery was performed. The histological diagnosis of the surgical
specimen was that of a choriocarcinoma (Fig. 2E and F). The ultrasound of the
testicles did not reveal anything abnormal. The serum β-hCG
concentration was 278 mIU/ml and the urine was weakly positive for
β-hCG. One month later, the serum β-hCG level had risen to 2,760
mIU/ml. Whole-brain and spinal radiation was initiated when the
patient was in a stable condition. Over 36 days, the patient was
administered a cumulative dose of 36 Gy whole-brain irradiation and
a 14-Gy local boost. The total dose was 50 Gy/27 Fx/36 days. An MRI
scan demonstrated that the tumor mass had shrunk during the course
of the radiotherapy (Fig. 2C and
D). The patient was followed up for more than half a year and
remained in a good condition.
Discussion
Choriocarcinomas are aggressive malignancies that
are grouped into two categories, gestational choriocarcinoma, which
is derived from any form of previously normal or abnormal
pregnancy, including a hydatidiform mole, spontaneous abortion or
ectopic pregnancy, and non-gestational choriocarcinoma, which
typically arises from gonadal organs, but also occurs rarely in
extragonadal primary sites. The present study described two cases
of non-gestational choriocarcinoma. One case was of an aggressive
choriocarcinoma with multiple metastases to the brain, but with an
unidentified origin, and the other case was of a primary
intracranial choriocarcinoma.
Non-gestational choriocarcinoma typically arises
from the gonadal organs. When the primary origin is extragonadal,
choriocarcinoma occurs preferentially at the midline section,
including the pineal body, mediastinum and retroperitoneum
(3). In the rare occurrences in
males, choriocarcinoma is most commonly observed in the testes. A
total of 106 male choriocarcinoma cases were reported between 1995
and 2006 (4). The testis was the
most common primary site in 33.0% (35/106). Metastasis was common,
with a frequency of 83% (81/98, the data from eight patients were
missing). The majority of the cases included multiple metastases.
The most common metastatic sites were the lung, liver and brain,
and the metastases progressed rapidly.
Several theories explaining the pathogenesis of
these extragonadal choriocarcinomas have been proposed, but no
conclusions have yet been reached. There are presently three
hypotheses: i) The tumor is a metastasis from a testicular
choriocarcinoma that regressed spontaneously (5); ii) the tumors arise from the
primordial germ cells that migrate abnormally during embryonic
development, which may explain the choriocarcinomas that originate
from organs that are remote from the genital tract (6); and iii) the tumor is a cancer that
develops originally as a non-trophoblastic neoplasm and is
transformed into a choriocarcinoma (7).
A diagnosis is possible if the site is near the body
surface, and a partial or total biopsy may be performed relatively
safely. However, a biopsy may not be performed at a number of
sites, including the mediastinum, pineal body, lung and
retroperitoneum, making a pre-operative diagnosis extremely
difficult. When a diagnosis of non-gestational choriocarcinoma is
suspected, it is necessary to fully examine the patient’s testes.
Generally, the physical examination of testicular tumors includes
palpation for testis enlargement and occasionally, an assessment of
trigger points for pain.
Furthermore, since non-gestational choriocarcinoma
has a trophoblastic element, the tumor secretes β-hCG. Therefore,
the tumor is associated with a markedly raised serum β-hCG
concentration, which is significant in the diagnosis and monitoring
of the clinical progress. Yokoi et al(4) reported that 96.4% of choriocarcinoma
patients have abnormally elevated serum β-hCG. This percentage
indicates that the test is highly precise. In the patient from case
1, the urine β-hCG was strongly positive and the serum β-hCG
concentration was 16,500 mIU/ml. This is consistent with the
aforementioned feature of choriocarcinoma. The serum β-hCG
concentration in the patient from case 2 was 278 mIU/ml, and one
month later, the concentration rose to 2,760 mIU/ml. An increased
level was not as evident as with the patient of case 1. This
finding may be explained by the resection of the primary site. In
addition, since the assay for β-hCG concentration is easy to
perform and non-invasive, it may be repeated and performed quickly,
placing little burden on the patient.
The clinical manifestation of non-gestational
choriocarcinoma is varied. The cancer from the primary site spreads
via the blood and lymphatics, with early hematogenous dissemination
to the lungs, liver, brain and other visceral sites (8). The usual mode of presentation in a
testicular choriocarcinoma is testicular enlargement, occasionally
with pain. Common metastatic symptoms include hemoptysis secondary
to pulmonary metastases, back pain secondary to retroperitoneal
spread, gastrointestinal bleeding due to gastrointestinal tract
metastases and neurological symptoms from brain metastases
(9).
It is evident that an early diagnosis was not
established in the first case, and the condition of the patient
deteriorated prior to the appropriate therapy being instituted.
Subsequent to the pathology results confirming the diagnosis, a
physical examination and ultrasound of the testis was performed,
and nothing abnormal was identified. Since an autopsy was not
allowed, the primary site was not identified. According to the
‘burned out tumor’ theory, as the primary site in the testis may be
quite small or even totally regressed, a clinical examination of
the testis may appear normal (10).
Therefore, the presumed primary site was the testis. Furthermore,
the second patient was diagnosed at a relatively early stage.
A total or subtotal resection of an intracranial
choriocarcinoma is useful for the prognosis of the patient.
Advances in neuroimaging, microsurgical techniques, surgical
instruments and surgery-supporting systems allow a subtotal or
greater resection of an intracranial choriocarcinoma to be feasible
and safe. However, the total removal of the tumor remains
difficult. Radiotherapy is an indispensable therapeutic modality
for intracranial choriocarcinoma. Kohyama et al(11) reported a successfully treated case
that underwent stereotactic radiation therapy. Stereotactic
radiation therapy was undertaken for the residual tumor of the
pineal region following a partial tumor removal, external
radiotherapy and chemotherapy, and the patient has been in a good
condition for more than four years. An increased risk of impaired
brain function due to radiotherapy has been recognized in young
patients with brain tumors, and the minimum dose of irradiation
supplemented with chemotherapy is now recommended (12). In Japan, a phase II study of
combined chemotherapy and radiotherapy was undertaken for
choriocarcinoma (14 neurosurgical clinics in Japan). In the study,
following a surgical tumor resection or subtotal resection, a
combination chemotherapy using carboplatin, etoposide and
ifosfamide followed by whole brain and spinal radiotherapy with
doses of 30 Gy and a 30 Gy boost delivered to a generous local
field was used. Thereafter, additional chemotherapy with the same
regimen was repeated a total of five times every three to four
months (13).
Choriocarcinoma is one of the most aggressive and
malignant germ cell tumors and the clinical outcome is poor. An
investigation based on 97 cases revealed that the mean survival
time was 7.7 months and that the one-month mortality rate was 23.8%
(4). As the patient of case 1
illustrated, the cancer had already metastasized to multiple
organs, including the brain, lungs, liver and kidneys, when the
patient was admitted, and the choriocarcinoma was identified at the
terminal stage. At post-operative day 7, the head CT scan
demonstrated new metastatic lesions that accompanied hemorrhaging.
The symptom of intracranial hypertension was grave and the patient
succumbed on post-operative day 9.
Acknowledgements
This study was sponsored by the Shanghai Rising-Star
Program (no. 10QH1401700), supported by the Shanghai Science and
Technology Commission and ‘Shu Guang’ project, the Shanghai
Municipal Education Commission and the Shanghai Education
Development Foundation, China (09SG20).
References
|
1
|
Hoffner L and Surti U: The genetics of
gestational trophoblastic disease: a rare complication of
pregnancy. Cancer Genet. 205:63–77. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Olsen JH, Mellemkjaer L, Gridley G,
Brinton L, Johansen C and Kjaer SK: Molar pregnancy and risk for
cancer in women and their male partners. Am J Obstet Gynecol.
181:630–634. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen F, Tatsumi A and Numoto S: Combined
choriocarcinoma and adenocarcinoma of the lung occurring in a man:
case report and review of the literature. Cancer. 91:123–129. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yokoi K, Tanaka N, Furukawa K, et al: Male
choriocarcinoma with metastasis to the jejunum: a case report and
review of the literature. J Nippon Med Sch. 75:116–121. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sesterhenn IA and Davis CJ Jr: Pathology
of germ cell tumors of the testis. Cancer Control. 11:374–387.
2004.PubMed/NCBI
|
|
6
|
Fine G, Smith RW Jr and Pachter MR:
Primary extragenital choriocarcinoma in the male subject. Case
report and review of the literature. Am J Med. 32:776–794. 1962.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Deshpande JR and Kinare SG:
Choriocarcinomatous transformation in metastases of an anaplastic
lung carcinoma - a case report. Indian J Cancer. 24:161–166.
1987.PubMed/NCBI
|
|
8
|
Mostofi FK: Proceedings: Testicular
tumors. Epidemiologic, etiologic, and pathologic features. Cancer.
32:1186–1201. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ohr J: Tumors of the testis, adnexa,
spermatic cord, and scrotum. Arch Pathol Lab Med.
124:18552000.PubMed/NCBI
|
|
10
|
Ahsaini M, Tazi F, Mellas S, et al: Pure
choriocarcinoma of the testis presenting with jaundice: a case
report and review of the literature. J Med Case Rep. 6:2692012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kohyama S, Uematsu M, Ishihara S, Shima K,
Tamai S and Kusano S: An experience of stereotactic radiation
therapy for primary intracranial choriocarcinoma. Tumori.
87:162–165. 2001.PubMed/NCBI
|
|
12
|
Jinguji S, Yoshimura J, Nishiyama K, et
al: Factors affecting functional outcomes in long-term survivors of
intracranial germinomas: a 20-year experience in a single
institution. J Neurosurg Pediatr. 11:454–463. 2013.PubMed/NCBI
|
|
13
|
Matsutani M, Ushio Y, Abe H, et al;
Japanese Pediatric Brain Tumor Study Group. Combined chemotherapy
and radiation therapy for central nervous system germ cell tumors:
preliminary results of a Phase II study of the Japanese Pediatric
Brain Tumor Study Group. Neurosurg Focus. 5:e71998. View Article : Google Scholar
|