Introduction
Myeloma remains an incurable disease despite a
marked improvement of complete remission and survival rates. Median
survival rates have improved from 2–3 to 7–8 years following the
advent of novel agents (including thalidomide, lenalidomide and
bortezomib) and autologous stem cell transplantation (ASCT)
(1). Prolonged survival may occur
in patients with low international staging system (ISS) stage of
disease, good-risk karyotypic aberrations, including hyperdiploidy
or t(11;14) or patients preceded by monoclonal gammopathy of
unknown significance (2). Written
informed consent was obtained from the patient.
Case report
A 56-year-old male was referred for symptomatic
myeloma in February 2012. The patient was first diagnosed with
myeloma in April 1991, presenting with syncope and a hemoglobin
(Hb) level of 6.5 g/dl. The patient exhibited partial response to
melphalan-based regimens, including melphalan and prednisolone
(MP), and vincristine, cyclophosphamide, melphalan and prednisolone
(VCMP); serum IgG levels dropped from 8,750 mg/dl (normal,
819–1,725 mg/dl) at diagnosis to 2,020 mg/dl in February 1992.
Chemotherapy was stopped in 1993 prior to the plateau phase with
extremely good partial remission. Chemotherapy was resumed
intermittently from 1996–1998. In 2002, VBCMP was used followed by
MP maintenance. In late 2005, thalidomide was added to intermittent
MP. The patient was referred to Queen Mary Hospital (Hong Kong,
China) in December 2011. Upon referral, the patient’s serum albumin
was 30 g/l and globulin was 76 g/l. Serum creatinine was 101 mg/ml
(normal, 67–109 nmol/l) and calcium was 2.61 mg/dl (normal, <2.5
mg/dl). Serum IgG measured 6,150 mg/ml (normal, 819–1,725 mg/dl),
IgA was 21 mg/dl (normal, 70–386 mg/dl) and IgM was 31 mg/dl
(normal, 55–307 mg/dl). Serum immunofixation showed monoclonal
IgG/λ with a paraprotein level of 52 g/l. Complete blood count
showed a Hb count of 7.5 g/dl, platelet count of
30×109/l (normal, 150–400×109/l) and
leukocyte count of 4.8×109/l (normal,
4–11×109/l) with blood smear showing 26% circulating
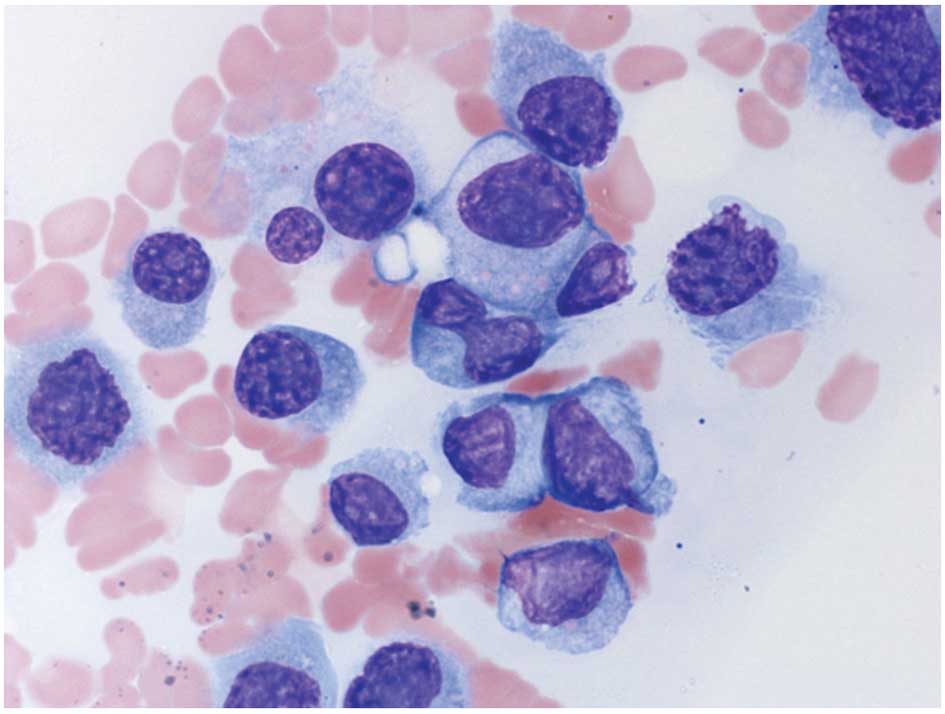
plasma cells and, hence, secondary plasma cell leukemia. Bone
marrow aspiration showed hypercellular bone marrow with 84% sheets
of small- to large-sized CD138+ plasma cells and marked
suppression of hematopoiesis (Fig.
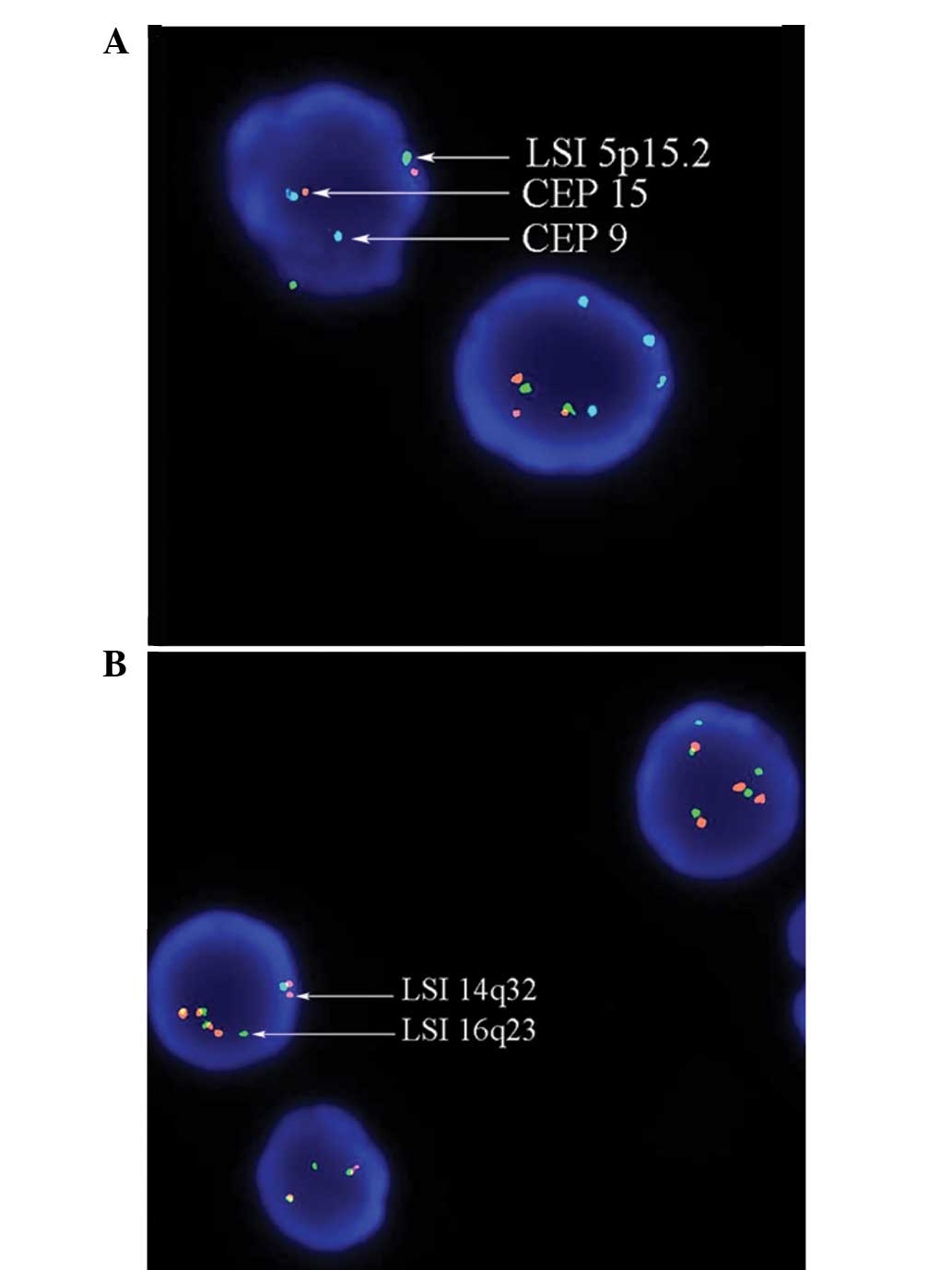
1). Fluorescence in situ hybridization with a panel of
probes for ploidy, t(4;14), t(14;16), del(17p) and chromosome 1q
gain showed hyperdiploidy together with t(14;16) (Fig. 2). The patient was administered
bortezomib, and cyclophosphamide and dexamethasone (VCD) was added.
The patient developed left pleural effusion in July 2012, which
showed pleomorphic plasma cells. Upon discussion with the family,
VCD was switched to bortezomib, lenalidomide and dexamethasone
(VRD). In late July 2012, the patient was admitted due to malaise
and recurrent left pleural effusion, for which chemical pleurodesis
was performed. The patient succumbed to refractory myeloma in
December 2012.
Discussion
In the present case report, although ISS and
karyotyping were unavailable at diagnosis, a prolonged survival of
>20 years without ASCT or bortezomib is rare. The presence of
hyperdiploidy may explain the prolonged survival, even without ASCT
or the use of novel agents, such as bortezomib or lenalidomide.
In addition, t(14;16) has been associated with poor
prognosis and typically inferior survival (2). In the present patient, the diagnostic
marrow was unavailable and, hence, it was not certain whether
t(14;16) was present at diagnosis or acquired later on, during the
course of disease. In a previous study of additional cytogenetic
aberrations in hyperdiploid myeloma at diagnosis (3), it was shown that hyperdiploidy with
concomitant t(14;16) occurs rarely at diagnosis, which has been
associated with poor survival (3).
Therefore, if t(14;16) occurred at diagnosis, the present patient
may have exhibited considerably shorter survival. Thus, t(14;16)
may have been acquired during the course of the patient’s myeloma,
which has not been previously reported.
The current patient presented at follow-up in Feb
2012. The value of circulating plasma cells in the peripheral blood
was 26%, consistent with secondary plasma cell leukemia. The
extramedullary disease nature was further illustrated by the
refractory malignant pleural effusion prior to the patient’s
demise. Secondary genetic aberrations, such as TP53 deletion and/or
1q23 amplification, may develop at chemoresistant relapse or
terminal myeloma with extramedullary disease (4,5).
However, in the current study, del(17p) and amp(1q) were absent
and, hence, the genetic events triggering the extramedullary
myeloma remain unknown.
In summary, the current case report presents the
prolonged survival of >20 years in a myeloma patient with
secondary plasma cell leukemia and myelomatous pleural effusion.
FISH on marrow plasma cells showed hyperdiploidy and concomitant
t(14;16), and karyotypes predicting superior and short survival.
The possibility of a primary hyperdiploidy with t(14;16) as a
secondary event has been discussed. While hyperdiploidy in myeloma
usually predicts superior survival, additional IgH translocation
may adversely impact prognosis. The possibility of t(14;16) as a
secondary genetic event requires further investigation.
References
|
1
|
Palumbo A and Anderson K: Multiple
myeloma. N Engl J Med. 364:1046–1060. 2011. View Article : Google Scholar
|
|
2
|
Fonseca R, Blood E, Rue M, Harrington D,
Oken MM, Kyle RA, Dewald GW, Van Ness B, Van Wier SA, Henderson KJ,
et al: Clinical and biologic implications of recurrent genomic
aberrations in myeloma. Blood. 101:4569–4575. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chng WJ, Santana-Dávila R, Van Wier SA,
Ahmann GJ, Jalal SM, Bergsagel PL, Chesi M, Trendle MC, Jacobus S,
Blood E, et al: Prognostic factors for hyperdiploid-myeloma:
effects of chromosome 13 deletions and IgH translocations.
Leukemia. 20:807–813. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tiedemann RE, Gonzalez-Paz N, Kyle RA,
Santana-Davila R, Price-Troska T, Van Wier SA, Chng WJ, Ketterling
RP, Gertz MA, Henderson K, et al: Genetic aberrations and survival
in plasma cell leukemia. Leukemia. 22:1044–1052. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fonseca R, Van Wier SA, Chng WJ,
Ketterling R, Lacy MQ, Dispenzieri A, Bergsagel PL, Rajkumar SV,
Greipp PR, Litzow MR, et al: Prognostic value of chromosome 1q21
gain by fluorescent in situ hybridization and increase CKS1B
expression in myeloma. Leukemia. 20:2034–2040. 2006. View Article : Google Scholar : PubMed/NCBI
|