Introduction
Gastric cancer (GC) is one of the most common causes
of mortality worldwide (1). In GC
patients, survival and prognosis mainly depend on the TNM stage of
the tumor at diagnosis. However, novel, specific, non-invasive
biomarkers that are able to identify high-risk patients with a poor
prognosis are urgently required. microRNAs (miRNAs) are
single-stranded RNA molecules (21–23 nucleotides) that regulate
gene expression by either interfering with transcription or
inhibiting translation. These miRNAs play important roles in
various human biological processes, including metabolism,
differentiation, cell proliferation and apoptosis (2). Altered miRNA expression has been
reported in various types of cancer, indicating that miRNAs may be
involved in cancer tumorigenesis. A number of studies have shown
that microRNAs circulate in the bloodstream in a highly stable,
extracellular form (3,4) and may therefore be used as blood-based
biomarkers for cancer and other diseases (5–7).
One of the most intensively studied miRNAs is
miRNA-21 (miR-21). miRNA-21 has been shown to be overexpressed in
numerous types of tumor tissues (8). It has been demonstrated that miR-21 is
involved in cancer at almost all stages (9). In GC cell lines, miR-21 has been shown
to promote proliferation and invasion, inhibit apoptosis and
regulate cell migration (10,11).
In clinical studies, miR-21 has been consistently overexpressed in
GC tissues compared with corresponding normal gastric tissues
(12). Tissue miR-21 levels have
been reported to be significantly associated with differentiation,
lymph node metastasis (11), tumor
size, depth of invasion and TNM stage (13,14) in
GC patients. Jiang et al(15) reported that miR-21 was significantly
associated with S-1/oxaliplatin responses in GC patients. In
serum/plasma samples from GC patients, miR-21 was also reported to
be overexpressed and was considered to possibly serve as a
diagnostic biomarker (16). Serum
miR-21 has been reported to be significantly reduced after tumor
resection in patients with GC, head and neck squamous cell
carcinoma and lung carcinoma (17).
In patients with diffuse large B-cell lymphoma, high serum miR-21
levels indicate a shorter relapse-free survival time (18). However, data concerning the possible
prognostic role of serum miR-21 levels in GC are limited.
Based on previous data on miR-21, we propose that
serum miR-21 may be related to the prognosis in GC. In the present
study, the expression levels of serum miR-21 were detected in 103
GC cases using quantitative polymerase chain reaction (qPCR).
Survival curves were compared using the log-rank test and Cox
regression analysis to test the hypothesis that serum miR-21 levels
were related to the prognosis in GC. Furthermore, the expression of
serum miR-21 was analyzed and its correlation with the
clinicopathological factors in GC was investigated.
Materials and methods
Patients and serum samples
Serum samples were obtained from 103 patients with
GC that had been surgically treated in the Beijing Friendship
Hospital (Beijing, China) between 2008 and 2009. No patients in
this study had received chemotherapy or radiotherapy prior to blood
sampling. Venous blood (5 ml) was collected from each patient prior
to surgery and centrifuged at 125 × g for 10 min. Supernatants were
recovered and stored at −80°C until further analysis. Follow-up
data for all recruited patients were acquired and the survival time
was calculated from the date of surgery to the date of mortality or
last follow-up on 20 June, 2012. Written informed consent was
obtained from each patient, and study approval was obtained from
the Beijing Friendship Hospital ethics review board.
RNA extraction and reverse
transcription
RNA for serum/plasma samples was isolated using an
miRcute miRNA isolation kit (Tiangen Biotech, Beijing, China),
according to the manufacturer’s instructions, with some
modifications. Briefly, 300 μl human serum was mixed with 300 μl
lysis buffer. Subsequent to phase separation, the aqueous phase was
mixed with ethanol then added to miRspin and miRelute columns. The
microRNA was eluted with 30 μl RNase-free water, with 18 μl used
for reverse transcription. The RNA concentration and purity were
assessed using an Eppendorf BioPhotometer (Eppendorf, Hamburg,
Germany). The RNA concentrations ranged from 26–54 ng/μl. The
purity of RNA was verified by measuring the absorbance of the
samples at 260 and 280 nm and determining the 260/280 ratio
(acceptable range, 1.77–1.92).
Reverse transcription was carried out using an
all-in-one miRNA first-strand cDNA synthesis kit (GeneCopoeia,
Rockville, MD, USA). Final reaction volumes were 25 μl and
contained 1 μl 2.5 U/μl poly-A polymerase, 1 μl RTase mix, 5 μl 5X
reaction buffer and 18 μl purified miRNA. Reverse transcription was
performed in a PTC-200 peltier thermal cycler (Bio-Rad
Laboratories, Shanghai, China) at 37°C for 60 min and then 85°C for
5 min.
Detection of serum miRNAs by qPCR
The qPCRs were conducted using an Applied Biosystems
(ABI) 7500 thermal cycler (Invitrogen, Carlsbad, CA, USA) in
96-well plates. Each miRNA assay was performed in duplicate with a
non-template control contained in each plate. To control for
inter-assay variation, the samples analyzed on the same plate were
for one specific miRNA. An all-in-one miRNA qPCR kit (GeneCopoeia)
was used, with 20 μl qPCR mixtures containing 10 μl 2X all-in-one
qPCR mix, 2 μl all-in-one miRNA qPCR primer, 2 μl universal adaptor
primer, 0.4 μl 50X ROX reference dye and 5.6 μl cDNA. Amplification
was performed on an ABI 7500 with a cycling profile of 50°C for 2
min and 95°C for 10 min, followed by 50 cycles of 95°C for 15 sec
and 60°C for 1 min. At the end of the 50th cycle, a melt curve
analysis was carried out to verify any non-specific
amplification.
Statistical analysis
The relative quantity (Qrel) of miR-21 was
quantified using the comparative ΔCt method using the following
equation: Qrel = E^ − (Cqtest sample −
CqAverage of miR-16 and miR-93), where E^ is
the power of the PCR amplification efficiency and Cq is the
quantification cycle.
We have previously reported that miR-16 and miR-93
may serve as double reference genes for the qPCR analysis of serum
miRNAs in GC samples (19). In the
present study, the statistical analysis was performed using SPSS
17.0 (SPSS, Inc., Chicago, IL, USA). Fisher’s exact test was used
to compare the difference between the serum miR-21 high and low
expression groups. The correlation between overall survival and
serum miR-21 was analyzed using the Kaplan-Meier method and the
log-rank test. The Cox proportional-hazards regression analysis was
used to evaluate whether serum miR-21 was an independent prognostic
factor for GC. All statistical tests were two-sided and P<0.05
was considered to indicate a statistically significant
difference.
Results
Clinical characteristics of study
participants with GC
The clinical characteristics of the study
participants are listed in Table I.
The study cohort was comprised of 68 males and 35 females. The mean
age was 60 years (range, 27–87 years) and the median follow-up
period was 35.9 months (range, 24.4–53.1 months). Of these
patients, 80 underwent radical surgery and 23 underwent palliative
surgery. None of the patients received peri-operative chemotherapy.
The patients were at TNM stage I (n=23), II (n=8), III (n=58) and
IV (n=14). At the last follow-up on June 20, 2012, 53 patients were
still alive.
 | Table ICorrelation between
clinicopathological factors and expression of miR-21 in serum. |
Table I
Correlation between
clinicopathological factors and expression of miR-21 in serum.
| Clinicopathological
factors | n | miR-21 expression
(mean ± SD) | P-value |
|---|
| Gender | | | 0.504 |
| Male | 68 | −0.611±0.509 | |
| Female | 35 | −0.705±0.434 | |
| Age | | | 0.712 |
| ≤60 | 53 | −0.653±0.491 | |
| >60 | 50 | −0.631±0.483 | |
| Tumor size | | | 0.048a |
| ≤5 cm | 52 | −0.713±0.507 | |
| >5 cm | 51 | −0.571±0.455 | |
| Tumor thickness | | | 0.021a |
| pT1 | 18 | −0.798±0.507 | |
| pT2 + pT3 | 12 | −0.577±0.547 | |
| pT4a | 52 | −0.712±0.407 | |
| pT4b | 21 | −0.375±0.531 | |
| Nodal status | | | 0.376 |
| pN0 | 25 | −0.778±0.543 | |
| pN1 | 14 | −0.592±0.521 | |
| pN2 | 17 | −0.526±0.462 | |
| pN3 | 47 | −0.628±0.447 | |
| Distant
metastasis | | | 0.196 |
| M0 | 89 | −0.667±0.491 | |
| M1 | 14 | −0.486±0.425 | |
| Venous
invasion | | | 0.750 |
| Positive | 28 | −0.617±0.486 | |
| Negative | 75 | −0.652±0.485 | |
| Tumor
differentiation | | | 0.443 |
| Poor | 59 | −0.611±0.452 | |
| Moderate/well | 44 | −0.685±0.528 | |
| UICC stage | | | 0.238 |
| I + II | 31 | −0.744±0.509 | |
| III | 58 | −0.626±0.481 | |
| IV | 14 | −0.486±0.425 | |
| Surgery type | | | 0.100 |
| Radical | 80 | −0.690±0.470 | |
| Palliative | 23 | −0.478±0.508 | |
Correlation between serum miR-21 levels
and GC prognosis
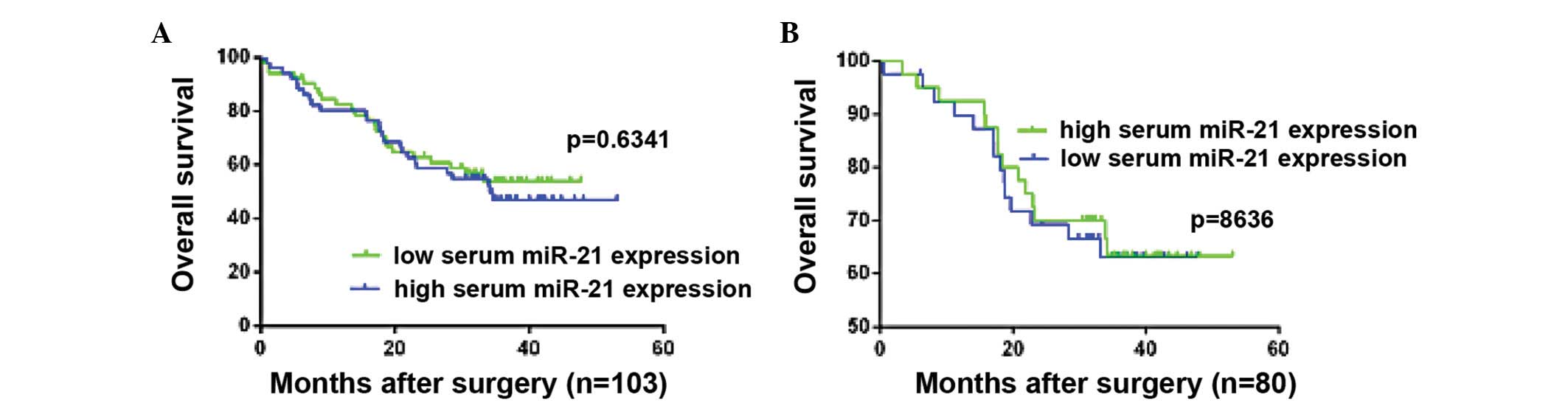
To evaluate whether the serum miR-21 level was
associated with prognosis in patients with GC, a survival analysis
was performed. The patients were divided into high miR-21
expression (n=51) and low miR-21 expression (n=52) groups. This
division was based on the cut-off value determined as the median
level of log-transformed relative quantity (−0.64) for the serum
miR-21 expression levels. According to the Kaplan-Meier method,
survival curves were not significantly different between the two
groups (P=0.6341; Fig. 1A). A
survival analysis for 80 of the 103 recruited patients who
underwent radical surgery yielded the same results (P=0.8636;
Fig. 1B).
High serum miR-21 levels were associated
with increased tumor size and advanced pT stage
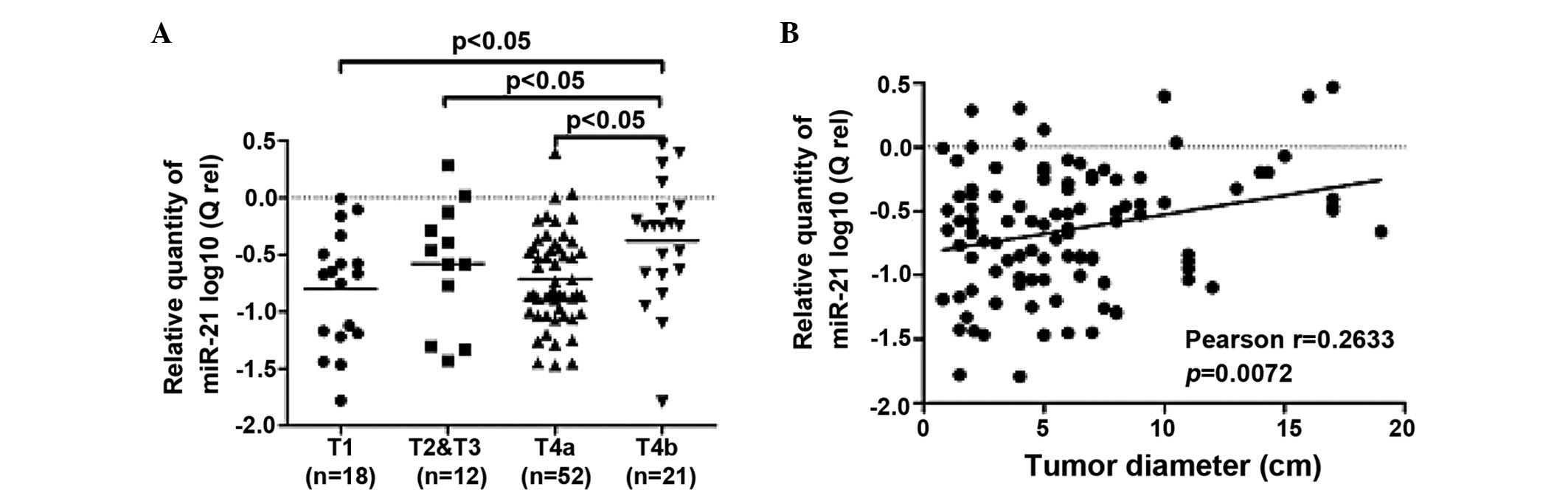
In order to better understand the potential roles of
serum miR-21 in GC development and progression, the correlation
between the serum miR-21 levels and the clinicopathological factors
of the GC patients were also assessed. The Mann-Whitney test showed
that there was no marked correlation between the miR-21 levels and
factors such as age, gender, differentiation, lymph node metastasis
and TNM stage (Table I). However,
the serum miR-21 level was significantly elevated in the pT4b cases
compared with the pT1, pT2 and T3, and pT4a cases (P<0.05;
Fig. 2A). Additionally, a Pearson
correlation analysis showed that the serum miR-21 levels rose
significantly when the tumor size was increased (r=0.2633,
P=0.0072; Fig. 2B).
Cox analyses of clinicopathological
factors in GC patients
A univariate analysis showed that the tumor size,
depth of invasion, lymph node metastasis, TNM stages and surgical
method were significantly correlated with post-operative survival.
The multivariate Cox proportional hazard regression analysis
indicated that TNM stage and surgical method were significantly
independent prognostic factors for patients with GC (P<0.05 and
P=0.024, respectively; Table
II).
| Table IIUnivariate and multivariate Cox
analysis of prognostic factors in patients with GC. |
Table II
Univariate and multivariate Cox
analysis of prognostic factors in patients with GC.
| | Univariate | Multivariate |
|---|
| |
|
|
|---|
| Factors | Categories | RR | RR (95% CI) | P-value | RR | RR (95% CI) | P-value |
|---|
| Gender | Male/female | 0.763 | 0.429–1.335 | 0.356 | - | - | - |
| Age | >60/≤60 | 0.975 | 0.557–1.708 | 0.975 | - | - | - |
| Tumor size | ≥5/<5 | 2.685 | 1.423–5.070 | 0.002a | 0.995 | 0.471–2.10 | 0.989 |
| Depth of
invasion | T1 + T2/T3 +
T4 | 5.960 | 2.140–16.60 | 0.001a | 0.001 | 0.0001–9.40 | 0.941 |
| Lymph node
metastasis |
Positive/negative | 7.001 | 2.173–22.554 | 0.001a | 2.066 | 0.306–13.92 | 0.456 |
|
Differentiation | Poor/moderate | 1.686 | 0.936–3.039 | 0.082 | - | - | - |
| Venous
invasion |
Positive/negative | 1.562 | 0.859–2.842 | 0.144 | - | - | - |
| TNM stage | I + II/IV | 0.097 | 0.034–0.275 | <0.0001a | 0.143 | 0.047–0.435 | 0.001a |
| III/IV | 0.272 | 0.134–0.553 | <0.0001a | 0.401 | 0.177–0.905 | 0.028a |
| Surgery type |
Palliative/radical | 0.195 | 0.110–0.347 | <0.0001a | 0.458 | 0.232–0.904 | 0.024a |
| Serum miR-21
expression | High/low | 0.873 | 0.498–1.530 | 0.873 | - | - | - |
Discussion
In the present study, serum miR-21 was examined in
order to explore its potential role as a prognostic biomarker for
patients with GC. The findings showed that serum miR-21 levels were
not able to predict a prognosis in the patients with GC. The serum
miR-21 expression levels were positively correlated with tumor
size, indicating that patients with higher serum miR-21 levels have
larger tumors.
In contrast to studies with regard to miR-21 in
tissues and cells of various types of cancer, research into miR-21
in the serum of GC patients is lacking. Serum miR-21 has been
reported to be overexpressed in numerous types of cancer, but
reduced levels have been observed after tumor resection (17,20–23).
Therefore, it is thought that miR-21 may serve as a potential
broad-spectrum serum-based biomarker for the diagnosis of certain
solid tumors (24). Despite growing
evidence highlighting its diagnostic value in various types of
cancer, few studies have systematically explored the prognostic
role of serum miR-21. To the best of our knowledge, the present
study is the first to determine whether serum miR-21 levels may be
used to predict a prognosis in patients with GC.
In the present study, the survival curves showed
that there was no significant difference between the higher and
lower serum miR-21 expression groups. The subgroup analysis was
defined according to whether patients underwent radical surgery,
and the same results were shown. Chan et al(12) and Ueda et al(14) reached the conclusion that tissue
miR-21 did not affect the clinical prognosis of GC, consistent with
the present results. Extensive research has revealed that miR-21 is
involved in proliferation, the cell cycle, metastasis and the
chemosensitivity of tumor cells by targeting several tumor
suppressor genes, including PTEN, MARCKS, PDCD4 and Cdc25A
(25–28). The correlation of tissue miR-21
expression levels and clinical stage, lymph node metastasis and
prognosis of cancer patients were also evaluated (13,14). A
correlation has rarely been reported between serum miR-21
expression levels and clinicopathological factors (12). This is likely due to the fact that
the origin and biological function of circulating miRNAs is poorly
understood. Recently, it was reported that miRNAs are selectively
secreted into the circulation and may mediate intercellular
communication (29,30). The miRNA expression profiles in
tissues and cells are likely to be very different from those miRNAs
in circulation. Similar miRNAs expressed in tissues and cells and
those in circulation may play different biological roles in cancer
development. Therefore, it is necessary to determine how serum
miR-21 is involved in GC development. Clarifying the correlation
between the serum miR-21 level and the clinicopathological factors
in patients with GC may provide certain clues as to why serum
miR-21 is not a predictor of GC prognosis.
The present study identified that higher serum
miR-21 levels were associated with an increased tumor size and an
advanced pT stage. Contradicting these results, Zheng et al
identified that miR-21 levels in circulating tumor cells, not
circulating miR-21 in serum, were associated with tumor size, TNM
stages and tissue categories in GC patients (20). Based on the findings of the present
study, we hypothesize that serum miR-21 levels may indirectly
reflect the tumor burden in GC patients, with serum miR-21
expression reduced following effective treatment. There have been
several reports stating that circulating miR-21 serum levels are
significantly reduced after tumor resection (17,20–23).
The measurement of serum miR-21 levels may have several promising
clinical applications inpatients with GC, including confirming the
completeness of the tumor resection, evaluating the efficacy of
adjuvant therapies and monitoring disease recurrence during the
follow-up period.
In the present study, a Cox hazard regression model
analysis showed that the tumor size and depth of invasion were
predictors of prognosis in the GC patients, but they were not
independent factors. This may explain why the serum miR-21 levels
were correlated with tumor size and depth of invasion, but were not
able to predict prognosis. As expected, the TNM stages and surgical
method were significant independent prognostic factors in the
patient cohort.
In addition, only serum miR-16 (without internal
references) has previously been used for quantifying serum miRNAs.
In the present study, serum miR-16 and miR-93 were used as double
internal references (19) when
calculating the Qrel of serum miR-21 by qPCR (31), leading to more convincing and
reliable qPCR data.
In conclusion, serum miR-21 levels were not able to
predict the prognosis of patients with GC. However, it was
associated with increased tumor size and advanced pT stage. The
expression level of serum miR-21 may be an indicator for the tumor
burden in GC patients, thereby making serum miR-21 a reliable
biomarker for effective therapies, such as chemotherapy and
surgical resection.
Acknowledgements
The authors are extremely grateful for the skilled
technical assistance of Dr Yingguang Gao and De Jie Yin. The
authors would also like to thank Yuan Li for invaluable
contributions towards the collection of the clinical data.
Abbreviations:
|
GC
|
gastric cancer
|
|
miRNAs
|
microRNAs
|
|
miR-21
|
microRNA-21
|
References
|
1
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
2
|
Huang Y, Shen XJ, Zou Q, Wang SP, Tang SM
and Zhang GZ: Biological functions of microRNAs: a review. J
Physiol Biochem. 67:129–139. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen X, Ba Y, Ma L, et al:
Characterization of microRNAs in serum: a novel class of biomarkers
for diagnosis of cancer and other diseases. Cell Res. 18:997–1006.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mitchell PS, Parkin RK, Kroh EM, et al:
Circulating microRNAs as stable blood-based markers for cancer
detection. Proc Natl Acad Sci USA. 105:10513–10518. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Huang Z, Huang D, Ni S, Peng Z, Sheng W
and Du X: Plasma microRNAs are promising novel biomarkers for early
detection of colorectal cancer. Int J Cancer. 127:118–126. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhao H, Shen J, Medico L, Wang D,
Ambrosone CB and Liu S: A pilot study of circulating miRNAs as
potential biomarkers of early stage breast cancer. PLoS One.
5:e137352010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zen K and Zhang CY: Circulating MicroRNAs:
a novel class of biomarkers to diagnose and monitor human cancers.
Med Res Rev. 32:326–348. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Volinia S, Calin GA, Liu CG, et al: A
microRNA expression signature of human solid tumors defines cancer
gene targets. Proc Natl Acad Sci USA. 103:2257–2261. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Selcuklu SD, Donoghue MT and Spillane C:
miR-21 as a key regulator of oncogenic processes. Biochem Soc
Trans. 37:918–925. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang Z, Li Z, Gao C, et al: miR-21 plays
a pivotal role in gastric cancer pathogenesis and progression. Lab
Invest. 88:1358–1366. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhang BG, Li JF, Yu BQ, Zhu ZG, Liu BY and
Yan M: microRNA-21 promotes tumor proliferation and invasion in
gastric cancer by targeting PTEN. Oncol Rep. 27:1019–1026.
2012.PubMed/NCBI
|
|
12
|
Chan SH, Wu CW, Li AF, Chi CW and Lin WC:
miR-21 microRNA expression in human gastric carcinomas and its
clinical association. Anticancer Res. 28:907–911. 2008.PubMed/NCBI
|
|
13
|
Motoyama K, Inoue H, Mimori K, et al:
Clinicopathological and prognostic significance of PDCD4 and
microRNA-21 in human gastric cancer. Int J Oncol. 36:1089–1095.
2010.PubMed/NCBI
|
|
14
|
Ueda T, Volinia S, Okumura H, et al:
Relation between microRNA expression and progression and prognosis
of gastric cancer: a microRNA expression analysis. Lancet Oncol.
11:136–146. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jiang J, Zheng X, Xu X, et al: Prognostic
significance of miR-181b and miR-21 in gastric cancer patients
treated with S-1/Oxaliplatin or Doxifluridine/Oxaliplatin. PLoS
One. 6:e232712011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kim SY, Jeon TY, Choi CI, et al:
Validation of circulating miRNA biomarkers for predicting lymph
node metastasis in gastric cancer. J Mol Diagn. Jun 24–2013.(Epub
ahead of print).
|
|
17
|
Tsujiura M, Ichikawa D, Komatsu S, et al:
Circulating microRNAs in plasma of patients with gastric cancers.
Br J Cancer. 102:1174–1179. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lawrie CH, Gal S, Dunlop HM, et al:
Detection of elevated levels of tumour-associated microRNAs in
serum of patients with diffuse large B-cell lymphoma. Br J
Haematol. 141:672–675. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Song J, Bai Z, Han W, et al:
Identification of suitable reference genes for qPCR analysis of
serum microRNA in gastric cancer patients. Dig Dis Sci. 57:897–904.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zheng Y, Cui L, Sun W, et al: MicroRNA-21
is a new marker of circulating tumor cells in gastric cancer
patients. Cancer Biomark. 10:71–77. 2011.PubMed/NCBI
|
|
21
|
Hsu CM, Lin PM, Wang YM, Chen ZJ, Lin SF
and Yang MY: Circulating miRNA is a novel marker for head and neck
squamous cell carcinoma. Tumour Biol. 33:1933–1942. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Le HB, Zhu WY, Chen DD, et al: Evaluation
of dynamic change of serum miR-21 and miR-24 in pre- and
post-operative lung carcinoma patients. Med Oncol. 29:3190–3197.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Komatsu S, Ichikawa D, Takeshita H, et al:
Circulating microRNAs in plasma of patients with oesophageal
squamous cell carcinoma. Br J Cancer. 105:104–111. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang B and Zhang Q: The expression and
clinical significance of circulating microRNA-21 in serum of five
solid tumors. J Cancer Res Clin Oncol. 138:1659–1666. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lou Y, Yang X, Wang F, Cui Z and Huang Y:
MicroRNA-21 promotes the cell proliferation, invasion and migration
abilities in ovarian epithelial carcinomas through inhibiting the
expression of PTEN protein. Int J Mol Med. 26:819–827.
2010.PubMed/NCBI
|
|
26
|
Li T, Li D, Sha J, Sun P and Huang Y:
MicroRNA-21 directly targets MARCKS and promotes apoptosis
resistance and invasion in prostate cancer cells. Biochem Biophys
Res Commun. 383:280–285. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Fassan M, Pizzi M, Giacomelli L, et al:
PDCD4 nuclear loss inversely correlates with miR-21 levels in colon
carcinogenesis. Virchows Arch. 458:413–419. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang P, Zou F, Zhang X, et al: microRNA-21
negatively regulates Cdc25A and cell cycle progression in colon
cancer cells. Cancer Res. 69:8157–8165. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Vickers KC, Palmisano BT, Shoucri BM,
Shamburek RD and Remaley AT: MicroRNAs are transported in plasma
and delivered to recipient cells by high-density lipoproteins. Nat
Cell Biol. 13:423–433. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang K, Zhang S, Weber J, Baxter D and
Galas DJ: Export of microRNAs and microRNA-protective protein by
mammalian cells. Nucleic Acids Res. 38:7248–7259. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Schmittgen TD and Livak KJ: Analyzing
real-time PCR data by the comparative C(T) method. Nat Protoc.
3:1101–1108. 2008. View Article : Google Scholar : PubMed/NCBI
|