Introduction
Branchial cleft cysts (BCCs) are the most common
congenital masses of the lateral neck and are caused by abnormal
embryonic development (1). Second
BCCs are the most common subtype of BCCs and are responsible for
~95% of all cases (2). Second BCCs
are divided into four types based on Bailey’s criterion (3). In previous studies, typical imaging
observations of BCCs have been described (4). However, the imaging appearances of
BCCs may be atypical under specific pathological conditions,
including secondary infection, hemorrhaging or malignant
transformation. The present study retrospectively evaluated
computerized tomography (CT) or magnetic resonance imaging (MRI)
observations of pathologically confirmed BCCs.
Materials and methods
Patients
In total, 17 patients (11 male and 6 female; age
range, 15–88 years; mean age, 39.1 years) with BCCs were reviewed
retrospectively. In these patients, infection, hemorrhaging or
malignant transformation of BCCs was confirmed by surgical or
pathological analysis. In total, 7 of the 17 patients underwent CT
examinations, and MRI scans were performed on an additional 10
patients. All patients exhibited painless swelling, however, 10
patients had a past history of repeated pain and an increase in the
size of the swelling which had been resolved with antibiotics. The
duration of symptoms varied between 10 days and 14 years. The study
was approved by the ethics committee of the First Affiliated
Hospital of Soochow University. Wriitten informed content was
obtained from the patients.
CT examination
CT scans were performed on a 64-row MDCT scanner
(Somaton Sensation 64; Siemens Healthcare, Erlangen, Germany) with
a beam pitch of 0.8, section thickness of 5.0 mm and reconstruction
increment of 4.7 mm.
MRI examination
MRI examination was performed on a 0.5 T MRI unit
(GE Vectra; GE Healthcare, Amersham, UK; n=3) and 1.5 T MRI unfit
(Philips Eclipse; Philips Healthcare, Amsterdam, The Netherlands;
n=7). The protocol for MRI for all patients was as follows: i)
axial spin echo (SE) T1-weighted imaging (T1WI; repetition time
(TR)/echo time(TE), 400–500/12–30 ms; n=10); ii) axial fast SE
(FSE) T2-weighted imaging (T2WI; TR/TE, 3,800–4,500/100–112 ms;
n=10); iii) coronal FSE T2WI (TR/TE, 3,500/112 ms; n=10); and iv)
time of flight MR angiography (MRA; TR/TE, 27/6.7 ms; n=4).
Postcontrast T1WI was performed following administration of 0.1–0.2
mmol/kg body weight gadolinium (Gd-DTPA; n=6).
Imaging analysis
All images were interpreted retrospectively by the
consensus of two radiologists with four- and three-years
experience, respectively, in head and neck imaging. The following
characteristics of each lesion were analyzed: Laterality, location,
border, attenuation or signal intensity and internal
architecture.
Results
Patient diagnosis
All 17 cases exhibited with second BCCs with 12
cases located on the left and 5 cases on the right. According to
the Bailey’s criterion, there were 5 cases of type I and 12 cases
of type II.
Atypical imaging features
The atypical imaging features included signal and
morphological abnormalities. The abnormal signal intensities were
caused by intracapsular bleeding (n=2) or solidification of cystic
fluid (n=2). Aberrant morphology mainly presented as the thickening
of the cystic wall (n=13).
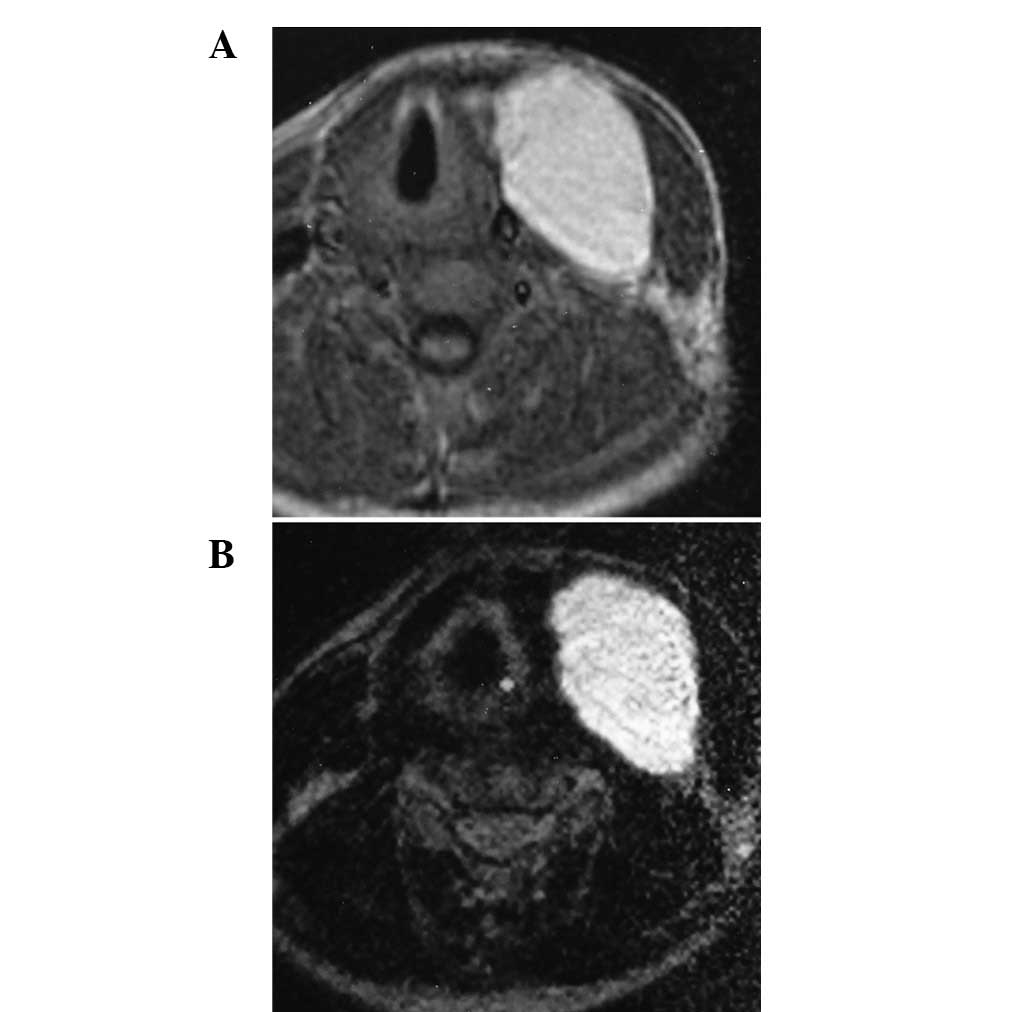
Pathological analysis
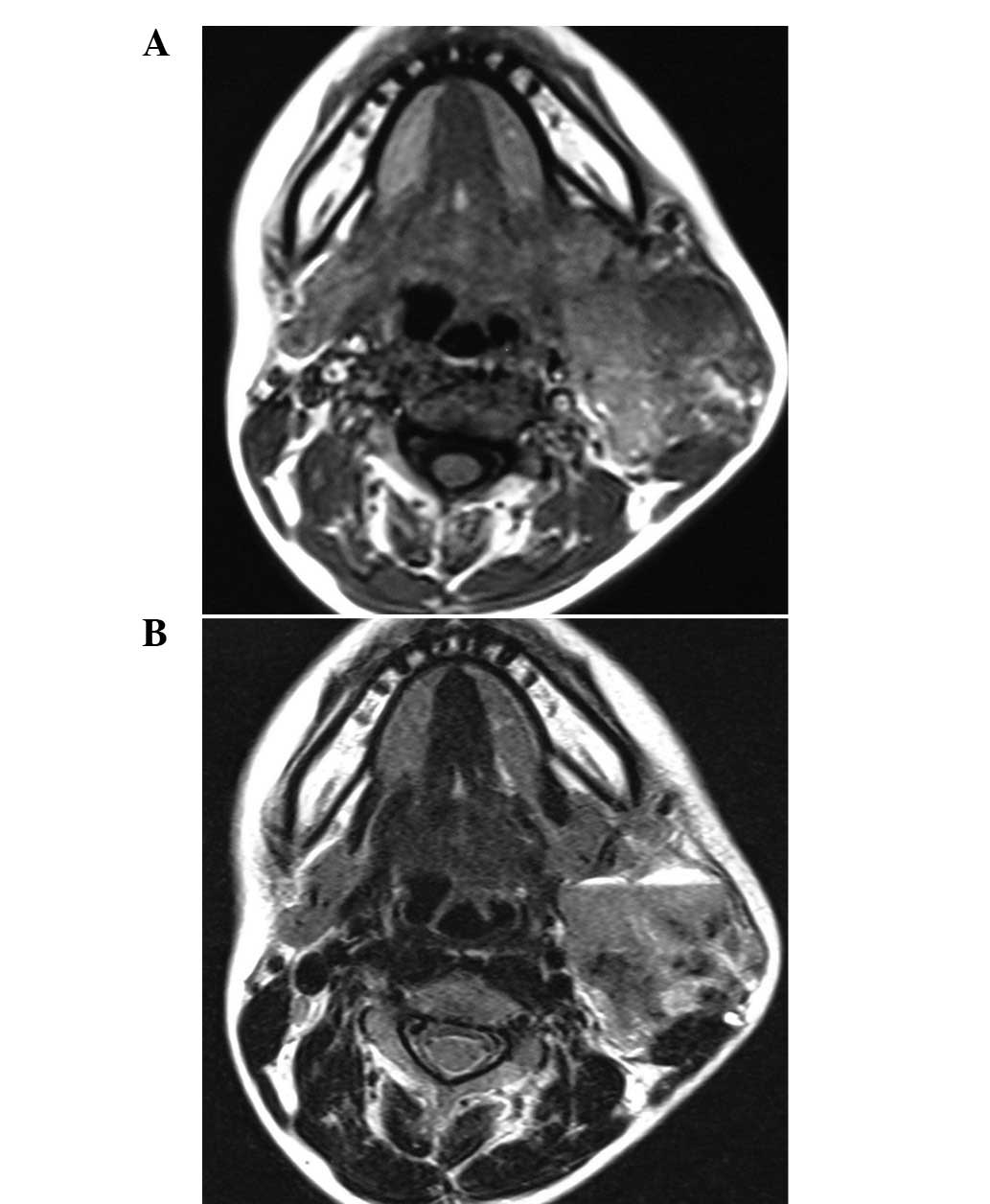
Intracystic hemorrhaging was observed in 2 cases.
Hemorrhaging appeared as homogeneously hyperintense on T1WI and
T2WI (Fig. 1). In gross pathology,
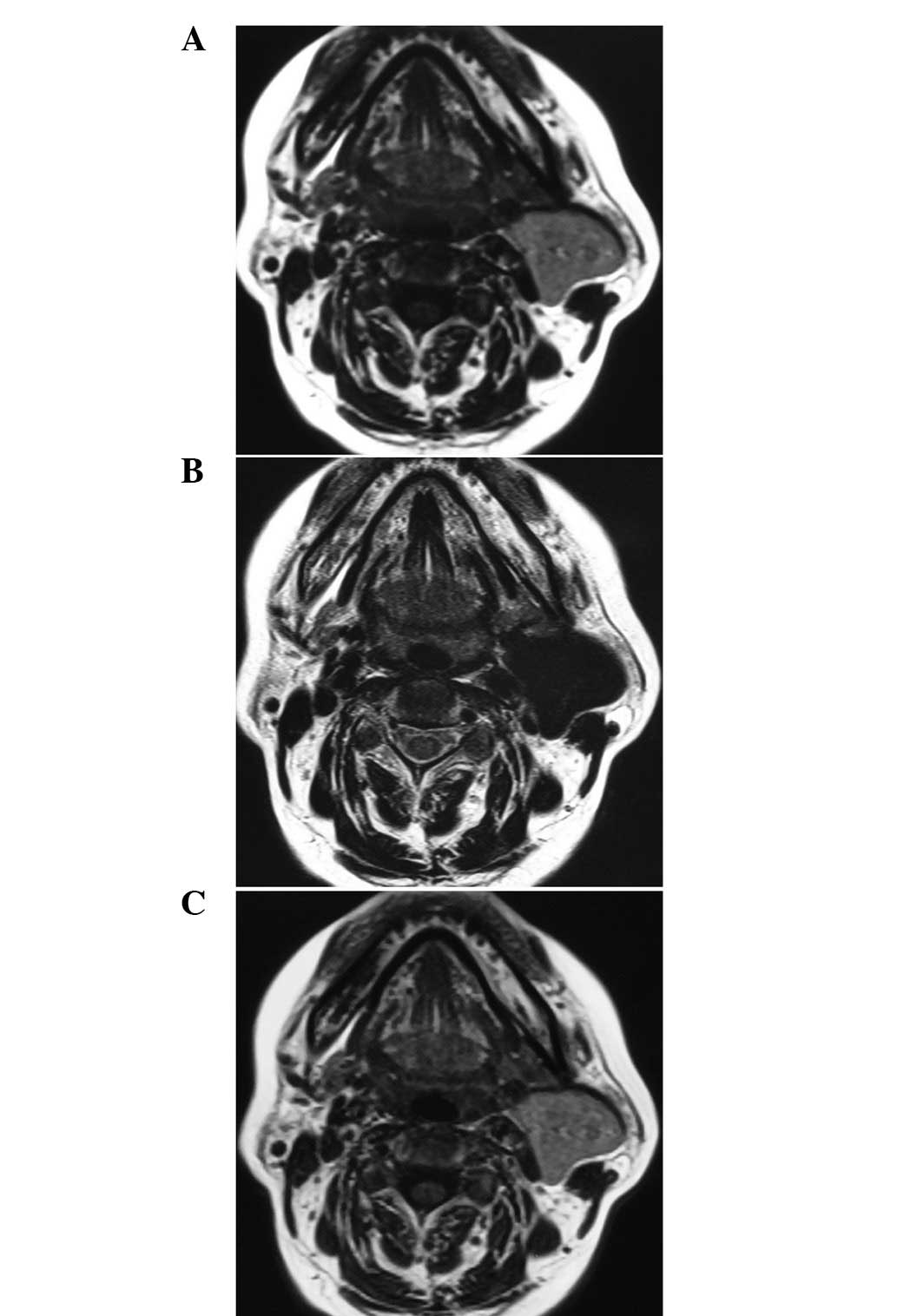
the content of the cysts was a dark-red liquid and the
solidification of cystic fluid was confirmed in an additional 2
cases, which appeared as jelly-like contents. Solidification of
cystic fluid showed slightly homogeneous hyperintensity compared
with muscle on T1WI and was homogeneously hypointensitive on T2WI.
Following the administration of Gd-DTPA, no significant enhancement
was observed (Fig. 2). Keratinizing
and non-keratinizing epithelial cells were observed
pathologically.
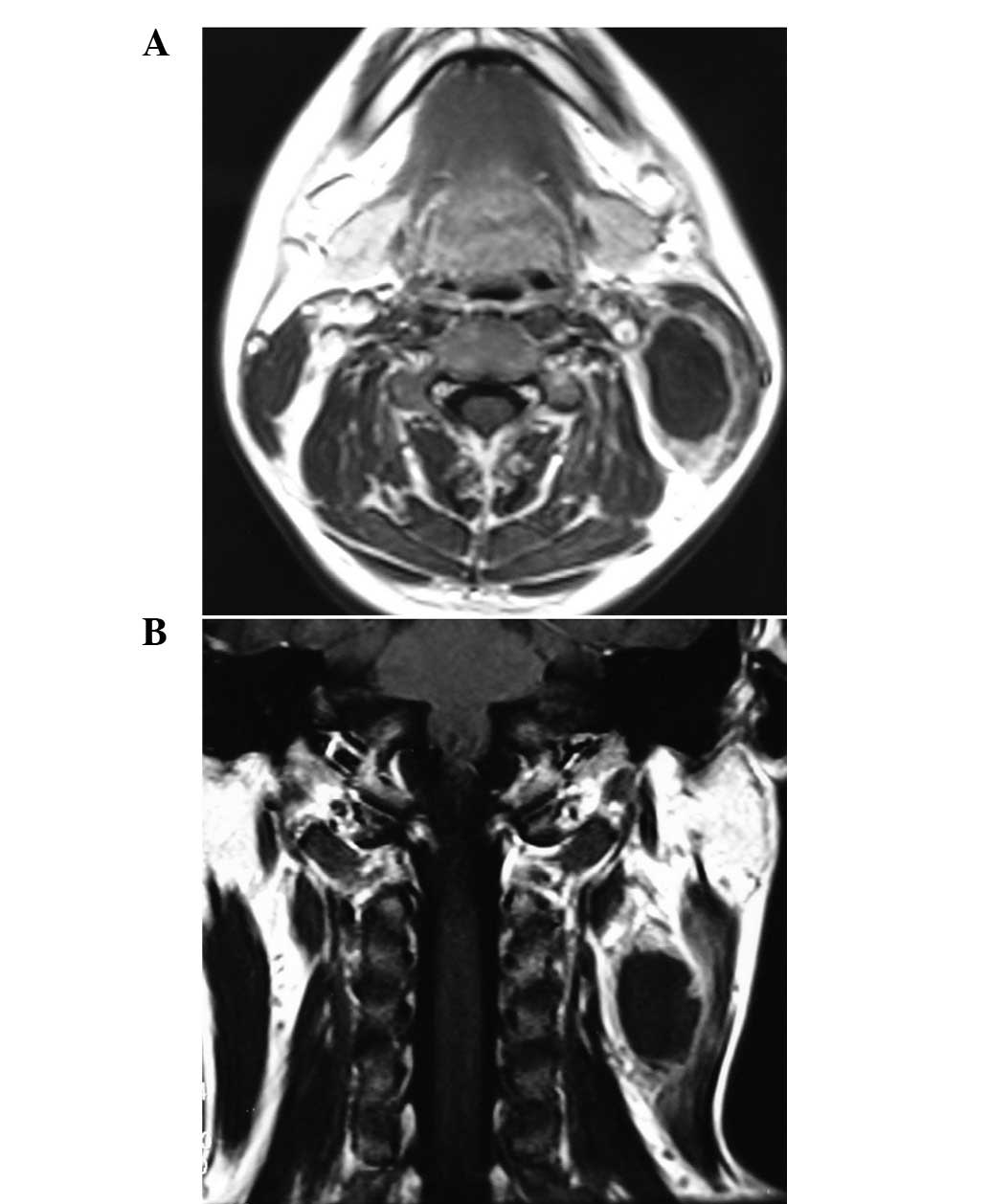
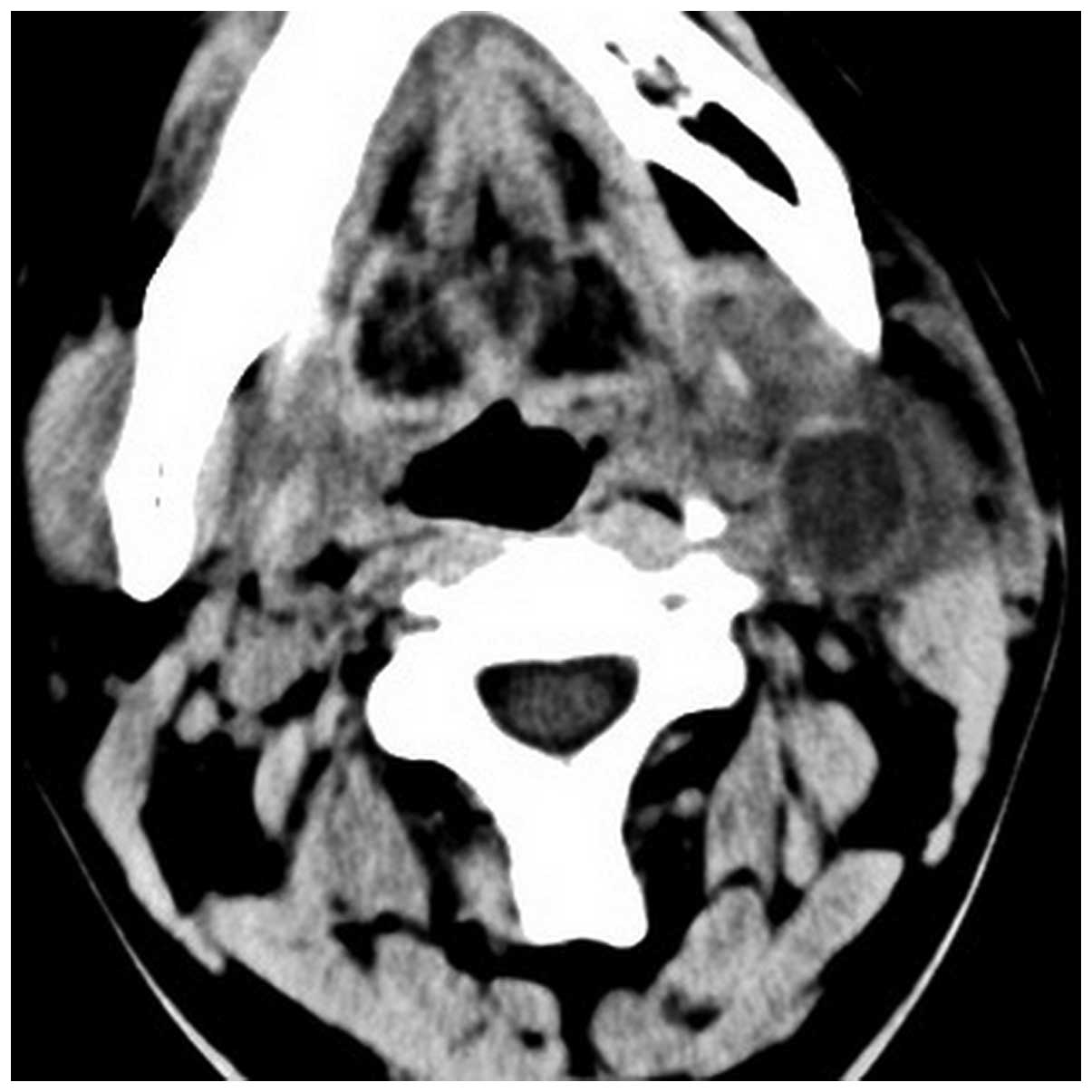
Furthermore, thickened cystic walls were observed on
CT (n=7) and MRI (n=6). Pathologically, there were 10 cases of
infection and 3 cases of carcinomatous transformation. In 4
patients, uniformly-thickened cystic walls with significant
enhancement were observed (Fig. 3).
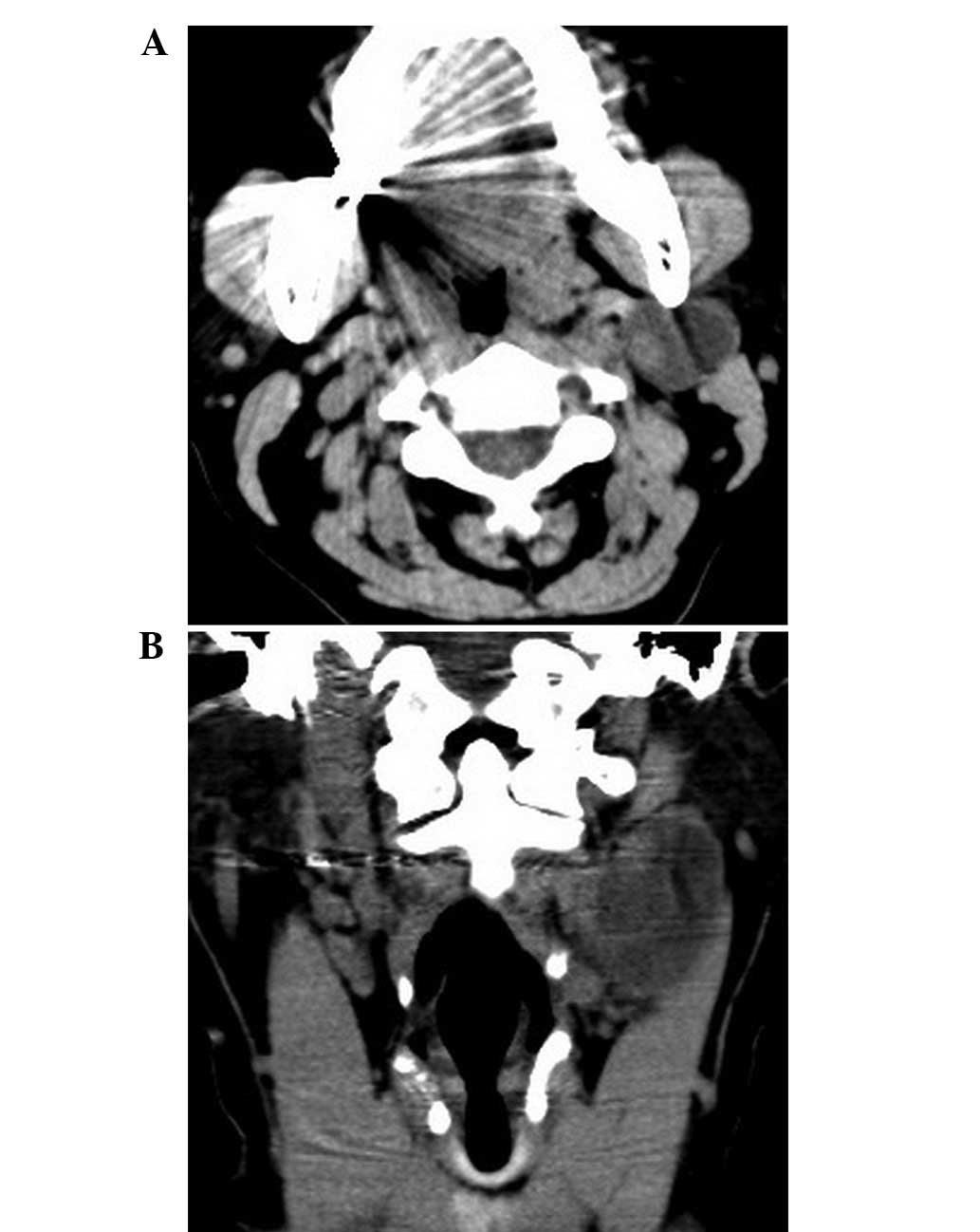
Intramural nodes were observed in 3 patients (infection, n=1;
malignant transformation, n=2; Figs.
3 and 4) and ill-defined
borders were present in 5 patients (infection, n=3; malignant
transformation, n=2; Fig. 5).
During the surgery, edema of adjacent structures was observed in 3
patients with infection and infiltration of adjacent structures
observed in 2 patients with malignant transformation. In one
patient, with a recurrent infection for 5 years, the lesion
appeared as a solid mass and a small cyst was identified in the
lesion. A heterogeneous signal intensity was observed on MRI
(Fig. 6). In an additional case
with malignant transformation, a lobulated cystic mass with
intratumoral septa was observed. The carotid artery sheath was
infiltrated and cervical metastasis of the lymph nodes was observed
in front of the ipsilateral trapezius.
Discussion
Generally, the clinical symptoms and imaging
observations of BBCs are typical. The majority of BCCs occur
between the ages of 10 and 40 years, without gender predilection
(1,5). The Bailey classification divides
second BCCs into the following four types (3): i) I, the most superficial subtype,
which reaches as deep as the platysma surface and lies along the
anterior surface of the sternomastoid muscle; ii) II, the most
common subtype, identified along the surface of the sternomastoid
muscle and posterior to the submandibular gland; iii) III, extends
medially at the bifurcation of the internal and external carotid
arteries to the lateral pharyngeal wall; and iv) IV, arises in the
pharyngeal mucosal space. BCCs often appear as painless masses,
which may enlarge and become painful or tender if secondarily
infected (1,6,7).
The common imaging observations of BCCs have been
described in specific previous studies (1,4,6,8–12).
Typical BCCs appear as well-circumscribed, fluid-like masses with
uniformly thin walls. The cystic wall shows mild enhancement
following the injection of contrast materials. The atypical imaging
features are likely to be observed when the lesions are accompanied
with infection, hemorrhaging or carcinomatous transformation, which
makes diagnosis difficult (1,12).
Intracystic hemorrhaging is usually caused by
secondary infection or biopsy attempts. Hemorrhages appears
hyperdense on CT scan and shows different signals in the various
phases on MRI (11). In the present
study, two cases showed high signal intensity on T1WI and T2WI,
which must be distinguished from neck lipomas, which also exhibit
hyperintensity on T1WI and T2WI. Furthermore, fat-suppression
sequences highlight crucial information for determining the
diagnosis.
Solidification of cystic fluid is also caused by
infection. The cystic fluid becomes muddy due to a rich protein
content, which increases the density of BCCs on CT scan and reduces
T1 relaxation time (4,11). When the cyst fluid is gradually
absorbed, a jelly-like contents is observed which appears
hypointense on T2WI, similar to jugular venous aneurysm.
Contrast-enhanced MRI and MRA examination is used to differentiate
solidification of cystic fluid from jugular venous aneurysm.
The thickening of the cystic wall is often induced
by infections (7,13,14).
When the wall is markedly thickened following repeated infection,
the lesion is likely to appear as a solid mass with a small area of
cyst (9). In one case in the
present study, the cystic mass was filled with inflammatory tissue.
Under these conditions, it is difficult to differentiate BCCs from
other solid or cystic tumors in the neck based only on the
morphology, density or signal intensity.
BCCs with malignant transformation are rarely
observed and its etiology remains unconfirmed. Specific factors may
be associated with the malignant transformation of BCCs, including
infection, repeated surgery or biopsy and other carcinogenic
stimuli (15–17). It is difficult to identify
malignancies based on clinical symptoms, imaging observations or
even biopsy. The definitive diagnosis relies on pathological
examinations following surgical resection (17). In the early stages, only thickened
cyst walls with well-defined borders are observed, which are often
misinterpreted as infected BCCs, but are unresponsive to antibiotic
therapy. One case in the present study was initially considered to
be BCCs with infection, however, malignant transformation was
confirmed by pathology. The lesion is likely to infiltrate
surrounding structures and cause cervical lymphadenopathy
atelectasis and distant (lung, bone, liver) metastases in later
stages (15,18).
It is difficult to diagnose BCCs preoperatively when
the imaging observations are atypical. However, the classical
location of the lesion, for example near to the mandibular angle or
the anterior sternocleidomastoid muscle, may be indicative
(1,19). Signal alternations correlate with
the component of cystic contents and the thickened walls of BCCs
indicate inflammation or malignant transformation. Malignant
transformation must be considered when BCCs exhibit ill-defined
borders with adjacent infiltrating vessels, or cause
lymphadenopathy atelectasis. Furthermore, it is important to
analyze the relative past history of the patient.
Acknowledgments
This study was supported by The National Natural
Science Foundation of China (81171393 and 31271066) and a Project
Funded by the Priority Academic Program Development of Jiangsu
Higher Education Institutions (PAPD).
Abbreviations:
|
BCC
|
branchial cleft cyst
|
|
Gd-DTPA
|
gadolinium
|
|
MRI
|
magnetic resonance image
|
|
SE
|
spin echo
|
|
TR
|
repetition time
|
|
TE
|
echo time
|
|
FSE
|
fast spin echo
|
|
MRA
|
MR angiography
|
|
CT
|
computerized tomography
|
References
|
1
|
Koeller KK, Alamo L, Adair CF and
Smirniotopoulos JG: Congential cystic masses of the neck:
radiologic-pathologic correlation. Radiographics. 19:121–146; quiz
152–153. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ghosh SK, Kr T, Datta S and Banka A:
Parapharyngeal second branchial cyst: A case report. Indian J
Otolaryngol Head Neck Surg. 58:283–284. 2006.PubMed/NCBI
|
|
3
|
Bailey H: The clinical aspects of
branchial cysts. Br J Surg. 10:173–182. 1933. View Article : Google Scholar
|
|
4
|
Shin JH, Lee HK, Kim SY, et al:
Parapharyngeal second brachial cyst manifesting as cranial nerve
palsies: MR findings. AJNR Am J Neuroradiol. 22:510–512.
2001.PubMed/NCBI
|
|
5
|
Daoud FS: Branchial cyst: an often
forgotten diagnosis. Asian J Surg. 28:174–178. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ahuja AT, King AD and Metreweli C: Second
branchial cleft cysts: variability of sonographic appearances in
adult cases. AJNR Am J Neuroradiol. 21:315–319. 2000.
|
|
7
|
Lo Re V III, Brennan PJ, Wadlin J, et al:
Infected branchial cleft cyst due to Bordetella
bronchiseptica in an immunocompetent patient. J Clin Microbiol.
39:4210–4212. 2001.PubMed/NCBI
|
|
8
|
Faerber EN and Swartz JD: Imaging of neck
masses in infants and children. Crit Rev Diagn Imaging. 31:283–314.
1991.PubMed/NCBI
|
|
9
|
Sarioglu S, Unlu M, Adali Y, et al:
Branchial cleft cyst with xanthogranulomatous inflammation. Head
Neck Pathol. 6:146–149. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Saussez S, De Maesschalk T, Mahillon V, et
al: Second branchial cyst in the parapharyngealspace: a case
report. Auris Nasus Larynx. 36:376–379. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cerezal L, Morales C, Abascal F, et al:
Pharyngeal branchial cyst: magnetic resonance findings. Eur J
Radiol. 29:1–3. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Setoguchi T, Hasuo K, Shida Y, et al:
Second branchial cleft cyst with ‘cyst-within-cyst’ appearance.
Clin Imaging. 31:352–355. 2007.
|
|
13
|
Ingoldby CJ: Unusual presentations of
branchial cysts: a trap for the unwary. Ann R Coll Surg Engl.
67:175–176. 1985.PubMed/NCBI
|
|
14
|
Ibrahim M, Hammoud K, Maheshwari M and
Pandya A: Congenital cystic lesions of the head and neck.
Neuroimaging Clin N Am. 21:621–639. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bernstein A, Scardino PT, Tomaszewki MM
and Cohen MH: Carcinoma arising in a branchial cleft cyst. Cancer.
37:2417–2422. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cho JS, Shin SH, Kim HK, et al: Primary
papillary carcinoma originated from a branchial cleft cyst. J
Korean Surg Soc. 81(Suppl 1): S12–S16. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Girvigian MR, Rechdouni AK, Zeger GD, et
al: Squamous cell carcinoma arising in a second branchial cleft
cyst. Am J Clin Oncol. 27:96–100. 2004. View Article : Google Scholar
|
|
18
|
Hong KH, Moon WS and Chung GH:
Radiological appearance of primary branchial cleft cyst carcinoma.
J Laryngol Otol. 113:1031–1033. 1999.PubMed/NCBI
|
|
19
|
Joshi MJ, Provenzano MJ, Smith RJ, et al:
The rare third branchial cleft cyst. AJNR Am J Neuroradiol.
30:1804–1806. 2009. View Article : Google Scholar : PubMed/NCBI
|