Introduction
Triple-negative breast cancer (TNBC) accounts for
15–20% of all breast cancers in the USA (1–3).
Treatment for TNBC [tumors that are estrogen receptor
(ER)-negative, progesterone receptor (PR)-negative and human
epidermal growth factor receptor 2 (HER2) non-amplified] continues
to be a challenge due to the fact that it is, by definition,
insensitive to the hormonal therapies and trastuzumab that have
been developed to treat other types of breast cancer. These tumors
appear to be exquisitely sensitive to chemotherapy with reported
complete pathological response in 21–31% of TNBC tumors in patients
treated with neoadjuvant chemotherapy (4,5).
Despite this, these tumors are considered aggressive and have
shorter intervals for locoregional recurrence, distant metastasis
and disease-free survival (1,6–8). Gene
expression profiling has resulted in the classification of breast
cancer into five molecular subtypes: Luminal A (ER+, PR+ and
Her2−), luminal B (ER+, PR+ and Her2+), basal-like (ER−, PR− and
Her2−; triple-negative) Her2-enriched (ER−/PR−/Her2+) and the
normal breast-like subtype. Recent studies have focused on whether
molecular subtype is indicative of prognosis and response to
treatment, but the data on directed-associated treatment is still
in its infancy (6–8). As a result, chemotherapy continues to
be the mainstay of treatment for TNBC breast cancers. However,
recently, there has been interest in determining whether radiation
therapy provides any additional benefit to patients with TNBC
tumors, regardless of initial surgical management.
There are currently no specialized guidelines for
the treatment of TNBC. In general, radiation therapy is indicated
for all patients with invasive carcinoma of the breast under the
following conditions: i) received breast-conserving therapy (BCT);
ii) underwent mastectomy with tumor >5 cm or with positive
margins; or iii) underwent mastectomy with positive axillary nodes.
Recently, however, there have been several studies that have aimed
to determine the outcomes of patients with TNBC tumors who received
radiation therapy, in comparison to those who did not. The results
of these studies appear to indicate that patients with TNBC tumors
who received radiation therapy had decreased risk of locoregional
recurrence and increased overall survival in comparison to those
that did not receive radiation therapy (9,10). As
a result, the present study was performed in order to determine
whether similar results were observed in our study population.
Materials and methods
Study design
Approval from the institutional review board of
Washington University School of Medicine (St. Louis, MO, USA) was
obtained prior to the initiation of this study. It was determined
that written consent from patients was not required given the
retrospective nature of the study. We retrospectively identified
493 patients from our prospectively maintained database with a
diagnosis of stage I–III TNBC who were treated between January 1,
2002 and December 31, 2009. Of these, 25 patients were diagnosed
with stage IV breast cancer at the time of diagnosis and
subsequently excluded from the analysis. As a result, 468 patients
were included in the total study population. Patients were
determined to have a TNBC based on immunohistochemical methods. A
designation of receptor negative status was conducted based on
having <1% stained cells. Fluorescence in situ
hybridization was used to confirm HER-2/neu status if
immunohistochemistry detected 2+ staining. Patients were
subsequently divided based on whether they underwent lumpectomy or
BCT versus simple mastectomy (SM) versus modified radical
mastectomy (MRM). Data collected included patient and tumor
characteristics; surgical, systemic and radiation treatment
received; and breast cancer-specific survival.
Statistical analysis
The primary outcome was overall survival (OS), which
was defined as time from the date of treatment initiation to the
date of mortality due to any cause. Survivors were censored at the
date of last contact. The distributions of patient and clinical
characteristics (including age, ethnicity, nodal status, tumor
grade and size, receipt of chemotherapy and type of surgery) by the
status of radiotherapy were compared using χ2 or
Fisher’s exact tests, as appropriate. Survival curves by
radiotherapy status were estimated using the Kaplan-Meier
product-limit method and compared by the log-rank test. Univariate
Cox proportional hazard models were fit to identify factors
significantly associated with OS. For those factors with P<0.15
in the univariate analyses, a multivariate Cox model was
constructed using a backward selection procedure to assess whether
the receipt of radiotherapy was an independent predictor of
survival. Two-way interaction terms between radiotherapy and other
factors in the multivariate Cox model were also assessed. All
analyses were two-sided and P<0.05 was considered to indicate a
statistically significant difference. Statistical analyses were
performed using SAS (SAS Institute, Cary, NC, USA).
Results
During the study period, between January 2002 and
December 2009, 468 patients with stage I–III TNBC were identified.
Of 468 patients, 249 (53%) underwent lumpectomy, 63 (14%) underwent
simple mastectomy and 156 (33%) underwent modified radical
mastectomy. The mean age of the study population was 54±13 years
old with a mean follow-up period of 51±21 months. The patient and
tumor characteristics of the study population are described in
Table I.
 | Table IPatient and tumor characteristics of
468 patients with triple-negative breast cancer treated between
2002 and 2009. |
Table I
Patient and tumor characteristics of
468 patients with triple-negative breast cancer treated between
2002 and 2009.
| Characteristic | n (%) |
|---|
| Age, years |
| <50 | 193 (41.2) |
| ≥50 | 275 (58.8) |
| Ethnicity |
| Caucasian | 287 (61.3) |
| African
American | 172 (36.8) |
| Other | 9 (1.9) |
| Clinical T stage |
| T1 | 166 (35.5) |
| T2 | 176 (37.6) |
| T3 | 37 (7.9) |
| T4 | 30 (6.4) |
| Unknown | 59 (12.6) |
| Histology |
| Invasive ductal | 386 (82.5) |
| Invasive
lobular | 9 (1.9) |
| Mixed/other | 73 (15.6) |
| Nuclear grade |
| 1 | 6 (1.3) |
| 2 | 55 (11.8) |
| 3 | 391 (83.6) |
| Unknown | 16 (3.4) |
| Node status |
| N0 | 295 (63.0) |
| N1 | 100 (21.4) |
| N2 | 12 (2.6) |
| N3 | 16 (3.4) |
| Unknown | 45 (9.6) |
| Stage |
| 1 | 149 (31.8) |
| 2a | 142 (30.3) |
| 2b | 54 (11.5) |
| 3 | 66 (14.1) |
| Unknown | 57 (12.2) |
Overall, 263 (56%) received adjuvant radiation
therapy, including 178/249 (71%) following lumpectomy, 13/63 (21%)
following SM and 72/156 (46%) following MRM (P<0.0001), as
listed in Table II. Of the 263
patients that received adjuvant radiation therapy, information
regarding their treatment regimen was only available for 152
patients (57.8%). For these patients, the mean initial radiation
dose was 5,137±938 cGy with a range of 2,000–10,240 cGy and median
of 5,000 cGy. Of these patients, 84 (55.3%) went on to receive an
additional boost of radiation with a mean of 1,292±629 cGy, median
of 1,000 cGy and range of 1,000–6,400 cGy. Factors predictive of
receipt of adjuvant radiation included type of surgical therapy
received (lumpectomy vs. SM and MRM), increasing tumor size and
positive nodal status (P<0.05 for each). The groups did not
differ with regard to age, ethnicity, tumor size or nuclear grade
(Table III).
| Table IILocoregional treatment of 468 patients
with triple-negative breast cancer. |
Table II
Locoregional treatment of 468 patients
with triple-negative breast cancer.
| Type of surgery | Received radiation, n
(%) | No radiation, n
(%) |
|---|
| Breast-conserving
therapy | 178 (71.5) | 71 (28.5) |
| Simple
mastectomy | 13 (20.6) | 50 (79.4) |
| Modified radical
mastectomy | 72 (46.2) | 84 (53.8) |
| Table IIICorrelation between patient and tumor
characteristics and receipt of radiation therapy in 468 patients
with triple-negative breast cancer. |
Table III
Correlation between patient and tumor
characteristics and receipt of radiation therapy in 468 patients
with triple-negative breast cancer.
| Characteristic | Radiation, n (%) | No radiation, n
(%) | P-value |
|---|
| Age, years |
| <50 | 83 (40.5) | 110 (41.8) | NS |
| ≥50 | 122 (59.5) | 153 (58.2) | |
| Ethnicity |
| Caucasian | 125 (61.0) | 162 (61.6) | NS |
| African
American | 77 (37.6) | 95 (36.1) | |
| Other | 3 (1.5) | 6 (2.3) | |
| Clinical T stage |
| T1 | 72 (35.1) | 94 (35.7) | NS |
| T2 | 75 (36.6) | 101 (38.4) | |
| T3 | 14 (6.8) | 23 (8.8) | |
| T4 | 11 (5.4) | 19 (7.2) | |
| Unknown | 33 (16.1) | 26 (9.9) | |
| Nuclear grade |
| 1 | 2 (1.0) | 4 (1.5) | NS |
| 2 | 22 (10.7) | 33 (12.6) | |
| 3 | 170 (82.9) | 291 (84.0) | |
| Unknown | 11 (5.4) | 5 (1.9) | |
| Node status |
| N0 | 141 (68.8) | 154 (58.6) | 0.0047 |
| N1 | 37 (18.1) | 63 (24.0) | |
| N2 | 0 (0) | 12 (4.6) | |
| N3 | 7 (3.4) | 9 (3.4) | |
| Unknown | 20 (9.8) | 25 (9.5) | |
| Chemotherapy |
| Adjuvant | 106 (51.7) | 128 (48.7) | <0.0001 |
| Neoadjuvant | 45 (22.0) | 106 (40.3) | |
| Unknown | 54 (26.3) | 22 (11.0) | |
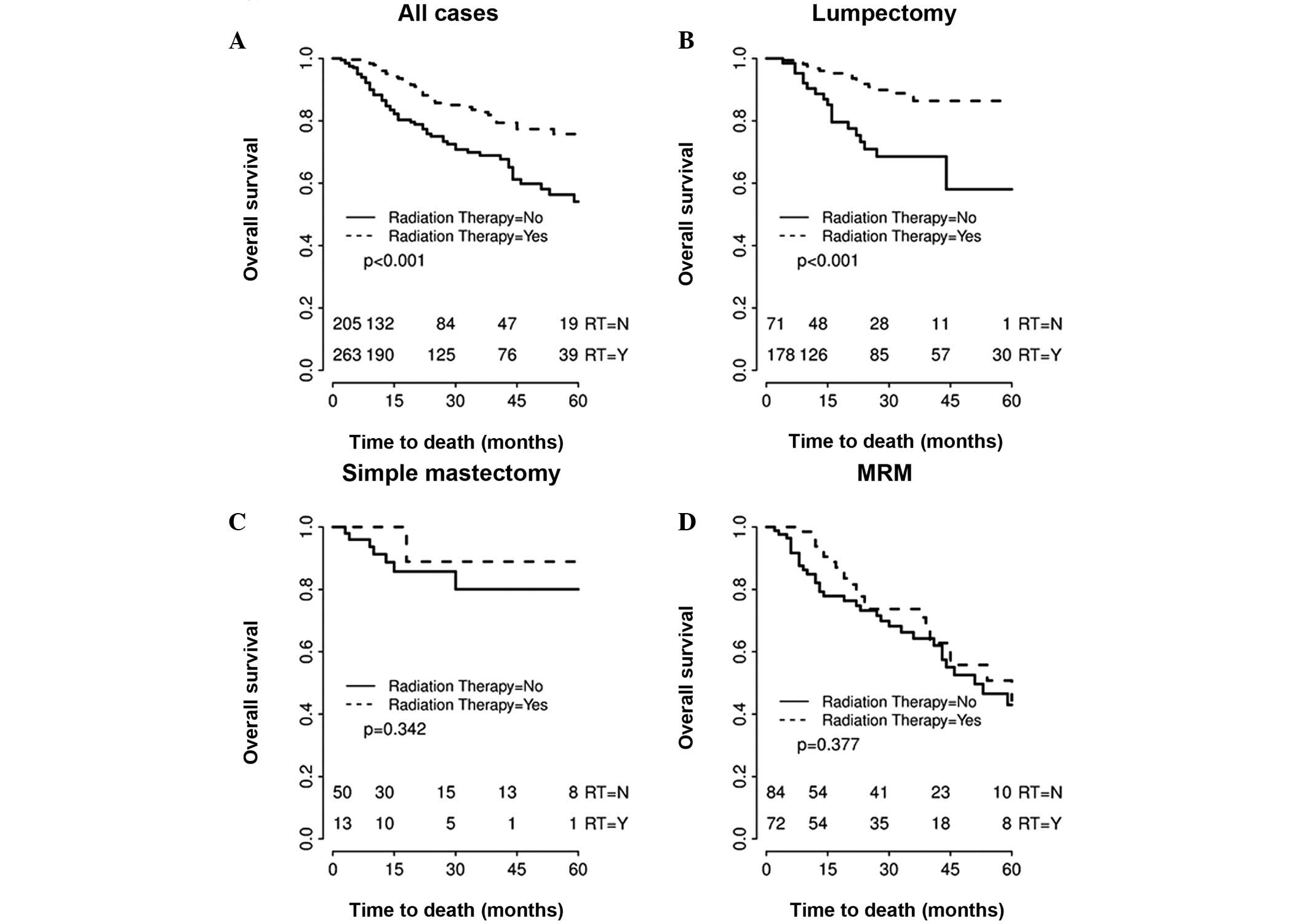
In the total cohort, univariate analysis
demonstrated that TNBC patients who underwent radiation therapy had
significantly improved overall survival (HR, 0.462; 95% CI,
0.311–0.69; P=0.0001) compared with those who did not receive
adjuvant radiation therapy. The overall four-year survival for
patients who received adjuvant radiation therapy was 77.34 versus
59.8% in patients who did not receive adjuvant radiation therapy.
Smaller tumor size (T1/T2), negative nodal status, receipt of
systemic chemotherapy and receipt of adjuvant radiation therapy
were all significantly associated with improved overall survival
(P<0.05 for each). However, when comparing survival by surgical
type, receipt of adjuvant radiation therapy significantly improved
survival in the lumpectomy group (HR, 0.30; 95% CI, 0.16–0.58;
P=0.001), but was not significantly associated with improved
survival in the SM group (HR, 0.38; 95% CI, 0.05–3.04; P=0.34) or
in the MRM group (HR, 0.77; 95% CI, 0.46–1.34; P=0.38). Fig. 1 illustrates the survival curves for
all TNBC study patients, as well as the survival curves for
patients treated by surgical intervention. Overall four-year
survival for patients treated by surgical intervention was 78.9,
81.78 and 54.26% for lumpectomy, SM and MRM groups,
respectively.
Discussion
The majority of studies have shown that TNBC is a
particularly aggressive form of breast cancer. These tumors tend to
present in younger patients, at a larger size (>2 cm), with
positive lymph nodes and with a higher mitotic index and grade
(3,8). Patients with TNBC demonstrate poorer
overall breast cancer-specific survival and shorter time to
recurrence, including locoregional recurrence and distant
metastasis (3,8,11,12).
In addition, studies have also documented that the incidence of
locoregional recurrence in TNBC patients peaks during years 1–4,
but then sharply declines (8).
Another study demonstrated that individuals with TNBC were more
likely to have locoregional failure, in comparison to distant
metastasis (11). As a result, the
impetus for identifying the optimal locoregional treatment strategy
for TNBC is of paramount importance. Yet, the connection between
locoregional control and survival has yet to be elucidated for this
sub-group of patients.
Currently, there are no specific guidelines for the
management of TNBC. Systemic chemotherapy continues to be the
mainstay of treatment, as the majority of TNBCs tend to be
exquisitely sensitive to chemotherapy. However, how this systemic
therapy specifically impacts locoregional control remains less
clear. Radiation therapy is indicated for the majority of patients
who undergo BCT and is also indicated for a sub-set of patients
following mastectomy if high-risk features for locoregional
recurrence exist, for example multiple positive lymph nodes, tumors
>5 cm, presence of lymphovascular invasion or positive surgical
margins. There are no tumor subtype-specific guidelines regarding
adjuvant radiation therapy. Given that adjuvant radiation therapy
is used for local control and TNBCs appear to have a higher
incidence of locoregional recurrence, there has been recent
interest in determining whether TNBC, a specific subtype of breast
cancer, is likely to benefit from radiation therapy regardless of
surgical intervention. Therefore, several retrospective studies
have analyzed the role of radiation therapy in TNBC, but their
findings are conflicting (11–14).
Dragun et al found that there was no
difference in progression-free and locoregional-free survival in
TNBC patients with or without radiation therapy during years 1–3.
However, the radiation group had a higher probability of
locoregional-free survival after three years (13). Abdulkarim et al found that
T1-2N0 TNBC patients treated with MRM without RT had a
significantly increased risk of locoregional recurrence in
comparison with those treated with BCT, but there was no difference
in overall survival (9). Wang et
al completed a randomized trial comparing adjuvant chemotherapy
versus adjuvant chemotherapy and radiation in stage I and II TNBCs
who underwent modified radical mastectomy. The authors found
improved recurrence-free and overall survival in patients who
received combined therapy in comparison to those who only received
chemotherapy (10). While the data
appears to be inconsistent with respect to whether radiation
decreases locoregional recurrence, there is even less clear
evidence of the effect of radiation therapy on survival.
The current study has several limitations. Firstly,
this is a retrospective study and, therefore, patients were not
randomized to receipt of radiation therapy. There are specific
guidelines regarding indications for adjuvant radiation therapy,
but it is clear that adherence to these guidelines may not always
occur and the reasons for this are unclear retrospectively. For
example, it is noteworthy that of the 249 patients who underwent
BCT, 71 patients (28.5%) did not receive any radiation therapy. It
would be interesting to know if there were clinicopathological
versus social factors that affected why these patients did not
receive radiation. Another weakness of the study is the lack of
consistency amongst the treatment regimens, including the radiation
therapy regimen and whether or not patients received chemotherapy.
The median radiation dose was 5,000 cGy and ~50% of those patients
received an additional median boost of 1,000 cGy. These are fairly
standard regimens, but the regimens did vary, reflecting the
heterogeneity of patients that receive some or all of their care at
our single institution. In future prospective studies, a more
standardized radiation therapy must be outlined.
Although the retrospective nature of this study is a
potential limitation, we propose that it represents one of the
largest analyses of the impact of adjuvant radiation therapy in
patients with TNBC, with the primary goal of determining the impact
of radiation therapy on overall survival, rather than on
locoregional recurrence. The study indicates that, while overall
survival of patients with TNBC improved with radiation therapy,
this improvement was attributed to those patients who underwent
BCT. There was no difference in the overall survival of patients
who underwent either form of mastectomy according to receipt of
radiation therapy. These observations corroborate those documented
by Kyndi et al in their study of high-risk patients who
underwent MRM (14). The authors
also found no survival benefit for post-mastectomy radiation in
patients with TNBC.
Radiation therapy is not innocuous, nor is it
without cost. Determining whether certain sub-groups of patients
with TNBC may be able to forego adjuvant radiation therapy is of
significant clinical interest.
Acknowledgements
The authors thank the patients who participated in
this study and physicians, nurses and research coordinators at the
Washington University Breast Cancer Oncology Clinic for their care
of these patients. The authors also wish to acknowledge the support
of the Biostatistics Core, Siteman Comprehensive Cancer Center and
NCI Cancer Center Support (grant no. P30 CA091842).
References
|
1
|
Zaky SS, Lund M, May KA, et al: The
negative effect of triple-negative breast cancer on outcome after
breast-conserving therapy. Ann Surg Oncol. 18:2858–2865. 2011.
View Article : Google Scholar
|
|
2
|
Fornier M and Fumoleau P: The paradox of
triple negative breast cancer: novel approaches to treatment.
Breast J. 18:41–51. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Carey LA, Perou CM, Livasy CA, et al:
Race, breast cancer subtypes, and survival in the Carolina Breast
Cancer Study. JAMA. 295:2492–2502. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Houssami N, Macaskill P, von Minckwitz G,
Marinovich ML and Mamounas E: Meta-analysis of the association of
breast cancer subtype and pathologic complete response to
neoadjuvant chemotherapy. Eur J Cancer. 48:3342–3354. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Asaga S, Kinoshita T, Hojo T, Suzuki J,
Jimbo K and Tsuda H: Prognostic factors for triple-negative breast
cancer patients receiving preoperative systemic chemotherapy. Clin
Breast Cancer. 13:40–46. 2013. View Article : Google Scholar
|
|
6
|
Lowery AJ, Kell MR, Glynn RW, Kerin MJ and
Sweeney KJ: Locoregional recurrence after breast cancer surgery: a
systematicreview by receptor phenotype. Breast Cancer Res Treat.
133:831–841. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Billar JA, Dueck AC, Stucky CC, et al:
Triple-negative breast cancers: unique clinical presentations and
outcomes. Ann Surg Oncol. 17(Suppl 3): 384–390. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dent R, Trudeau M, Pritchard KI, et al:
Triple-negative breast cancer: clinical features and patterns of
recurrence. Clin Cancer Res. 13:4429–4434. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abdulkarim B, Cuartero J, Hanson J,
Deschênes J, Lesniak D and Sabri S: Increased risk of locoregional
recurrence for women with T1-2N0 triple-negative breast cancer
treated with modified radical mastectomy without adjuvant radiation
therapy compared with breast-conserving therapy. J Clin Oncol.
29:2852–2858. 2011. View Article : Google Scholar
|
|
10
|
Wang J, Shi M, Ling R, et al: Adjuvant
chemotherapy and radiotherapy in triple-negative breast carcinoma:
a prospective randomized controlled multi-center trial. Radiother
Oncol. 100:200–204. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Haffty BG, Yang Q, Reiss M, et al:
Locoregional relapse and distant metastasis in conservatively
managed triple negative early-stage breast cancer. J Clin Oncol.
24:5652–5657. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Panoff JE, Hurley J, Takita C, et al: Risk
of locoregional recurrence by receptor status in breast cancer
patients receiving modern systemic therapy and post-mastectomy
radiation. Breast Cancer Res Treat. 128:899–906. 2011. View Article : Google Scholar
|
|
13
|
Dragun AE, Pan J, Rai SN, Kruse B and Jain
DL: Locoregional recurrence in patients with triple-negative breast
cancer: preliminary results of a single institution study. Am J
Clin Oncol. 34:231–237. 2011. View Article : Google Scholar
|
|
14
|
Kyndi M, Sørensen FB, Knudsen H, et al;
Danish Breast Cancer Cooperative Group. Estrogen receptor,
progesterone receptor, HER-2, and response to postmastectomy
radiotherapy in high-risk breast cancer: the Danish Breast Cancer
Cooperative Group. J Clin Oncol. 26:1419–1426. 2008. View Article : Google Scholar
|