Introduction
Previously, platinum-based chemotherapy regimens
were not commonly prescribed for patients with metastatic breast
cancer, as other regimens were considered to exhibit improved
efficacy and toxicity profiles (1).
Interest in platinum-based therapies was renewed with the
observation that BRCA1 deficient cell lines have a higher
sensitivity to DNA crosslinking agents, such as cisplatin, compared
with other breast cancer cell lines (2). There also appears to be a significant
overlap in terms of the histological and molecular features between
BRCA1-deficient breast tumors and types of triple-negative breast
cancer (TNBC) (3). Due to these
similarities, it has been hypothesized that the DNA repair defects
that sensitize BRCA1-deficient breast cancer tumors to platinum may
also be present in TNBC, indicating that platinum-based
chemotherapies may be an effective treatment option for this subset
of breast cancer (4).
While the exact role of platinum-based
chemotherapies in TNBC is being explored (Triple-Negative Trial,
NCT00532727; http://www.clinicaltrials.gov), there appears to be
conflicting data from retrospective studies with regard to efficacy
in the neoadjuvant (5) and
metastatic settings (6).
Previously, in two prospective neoadjuvant studies, the use of
single agent cisplatin in patients with TNBC resulted in
pathological complete response rates of 22 (7) and 10% (8), respectively. In the metastatic
setting, a multicenter phase II trial tested cisplatin or
carboplatin first-line chemotherapy for patients with metastatic
TNBC. Although there was a response rate of 30%, the median
progression-free survival time was only 3 months (9). These results are not superior to
historical data that shows that chemotherapy for triple-negative
disease has a median response duration of 12, 9 and 4 weeks in
first-, second- and third-line settings, respectively (10). Given this, it does not appear that
platinum has any definite additional activity compared with that of
the more commonly used regimens.
As the role of platinum-based chemotherapy in the
treatment of TNBC is controversial, the present study reviewed
platinum-based chemotherapy in metastatic breast cancer at the
Ottawa Hospital Cancer Center (Ottawa, Canada). The main objective
was to assess whether platinum-based chemotherapy is more effective
than non-platinum-based chemotherapy in patients with metastatic
TNBC in terms of time to progression. Similarly, it was assessed
whether platinum-based chemotherapy is more effective than
non-platinum-based chemotherapy in metastatic non-TNBC.
Patients and methods
Patient characteristics
All patients with histologically confirmed
metastatic or locally recurrent breast cancer who received
platinum-based chemotherapy at the Ottawa Hospital Cancer Centre
(Ottawa, Canada) between January 2000 and September 2010 were
identified. Patient data were collected through a review of
electronic health records.
Patients were separated into two cohorts, TNBC and
non-TNBC. Patients were classified as TNBC based on their surgical
or biopsy results, which were defined as follows: i) Estrogen and
progesterone receptor levels <1% by immunohistochemistry (IHC);
and ii) human epidermal growth factor receptor 2 scored as 0, 1 or
2 on IHC and/or negative fluorescence in situ hybridization
testing (11). Eligible patients
were required to have received any single or combination drug
platinum-based chemotherapy regimen for incurable disease. Patients
with an incomplete receptor status were excluded, as well as those
who had not received platinum specifically for advanced disease or
those who had received chemotherapy for separate types of
concomitant cancer. The present study received Research Ethics
Board approval from the Ottowa Hospital Cancer Center.
The reason for discontinuation of every line of
chemotherapy (e.g. toxicity and disease progression) and the date
of disease progression were determined from the clinical notes. The
primary outcome was time to progression, defined from the start
date of one line of chemotherapy to the date of the last cycle
administered prior to documented disease progression, clinical
deterioration with no further chemotherapy or documented mortality.
Lines of chemotherapy with an unclear outcome due to loss to
follow-up were not considered in the analysis.
Statistical analysis
Descriptive statistics were used to summarize the
characteristics of the patients with TNBC and non-TNBC. For each
study cohort (TNBC and non-TNBC), Kaplan-Meier curves were
constructed comparing the cumulative incidence of disease
progression for patients exposed to platinum-based chemotherapy
versus non-platinum-based chemotherapy. Differences between curves
were assessed by calculating log-rank test P-values. P<0.05 was
considered to indicate a statistically significant difference. In
addition, crude incidence rates of disease progression were
calculated for platinum-based chemotherapy and non-platinum-based
chemotherapy, together with 95% confidence intervals (CIs) based on
the Poisson distribution. Cox proportional hazards models were used
to estimate crude and adjusted hazard ratios (HRs) and 95% CIs of
disease progression associated with the use of platinum-based
chemotherapy versus non-platinum-based chemotherapy for each line
of chemotherapy. Under this scheme, various models were constructed
for each line of chemotherapy and thus, it was possible for
patients to contribute data to more than one line of chemotherapy.
The models were adjusted for age, prior adjuvant and neoadjuvant
chemotherapy, previous use of platinum (in models of second- and
third-line chemotherapy), tumor grade, initial stage, site and
extent of first distant relapse and presence of brain metastasis.
Results were analyzed using SAS version 9.2 (SAS Institute Inc.,
Cary, NC, USA).
Results
Patient population
A total of 173 patients with metastatic or locally
recurrent breast cancer received platinum-based chemotherapy. In
total, 14 patients were excluded due to incomplete receptor status
results, leaving 58 patients in the TNBC cohort and 101 patients in
the non-TNBC cohort. Of these, 50 patients in each cohort received
platinum-based chemotherapy in the first, second or third line. Due
to the anticipated shorter survival of the TNBC cohort, comparisons
for this study were restricted to the first three lines of
therapy.
Baseline patient characteristics for each group are
shown in Table I. Prior adjuvant
chemotherapy was received by 55 and 66% of TNBC and non-TNBC
patients, respectively, and the rates of prior neoadjuvant
chemotherapy were 36 and 31%, respectively. At the onset of
metastatic disease, 59% of the patients with TNBC exhibited
visceral metastasis, including 14% with initial brain metastasis,
compared with 53% of non-TNBC patients who exhibited visceral
metastasis, including 5% with initial brain metastasis. By the end
of study period, 87% of the entire cohort had succumbed to their
diseases or were receiving no further anticancer treatment. In
addition, 5% of patients were lost to follow-up.
 | Table IBaseline characteristics of TNBC and
non-TNBC cohorts. |
Table I
Baseline characteristics of TNBC and
non-TNBC cohorts.
| Characteristics | TNBC | Non-TNBC |
|---|
| Cohort size, n | 58 | 101 |
| Age at diagnosis,
years (SD) | 48.9 (11.2) | 50.3 (9.8) |
| Time between
diagnosis and 1st treatment, weeks (SD) | 9.7 (21.4) | 28.5 (59.4) |
| Extent of first
distant relapse, n (%)a |
| Single-site | 39 (67.2) | 61 (60.4) |
| Multi-site | 19 (32.8) | 40 (39.6) |
| Type of first distant
relapse, n (%)a |
| Non-visceral | 24 (41.4) | 47 (46.5) |
| Visceral | 34 (58.6) | 54 (53.5) |
| Adjuvant therapy, n
(%)a |
| No | 18 (31.0) | 26 (25.7) |
| Yes | 32 (55.2) | 67 (66.3) |
| Unknown | 8 (13.8) | 8 (7.9) |
| Neoadjuvant therapy,
n (%)a |
| No | 36 (62.1) | 68 (67.3) |
| Yes | 21 (36.2) | 32 (31.7) |
| Unknown | 1 (1.7) | 1 (1.0) |
| Disease metastatic to
the brain, n (%)a |
| At diagnosis | 8 (13.8) | 5 (4.9) |
| Following
diagnosis | 35 (60.3) | 66 (65.4) |
| Unknown | 15 (25.9) | 30 (29.7) |
| Metastatic at
diagnosis, n (%)a |
| No | 54 (93.1) | 83 (82.2) |
| Yes | 4 (6.9) | 18 (17.8) |
| Median overall
survival from diagnosis of metastatic disease, weeks | 60 | 144 |
| Patient status, n
(%) |
| Alive on
treatment | 4 (6.9) | 6 (5.9) |
| Succumbed, unrelated
to malignancy | 1 (1.7) | 1 (1.0) |
|
Succumbed/palliative | 49 (84.5) | 90 (89.1) |
| Lost to
follow-up | 4 (6.9) | 4 (4.0) |
Table II shows the
types of platinum-based regimens used. The combinations of
vinorelbine or gemcitabine with cisplatin or carboplatin were the
most frequent platinum-based regimens used (>70%). On average,
TNBC patients received 2.8 lines of chemotherapy in the metastatic
setting (range, 1–5) versus 3.9 lines for non-TNBC patients (range,
1–6). TNBC patients received platinum in the first, second or third
lines in 27, 36.5 and 17.6% of cases, respectively, compared with
12.4, 21.2 and 20.9% of cases, respectively, for the non-TNBC
cohort.
| Table IIPlatinum-based regimens received. |
Table II
Platinum-based regimens received.
| Platinum
regimens | Patients, n (%) |
|---|
|
Cisplatin-vinorelbine | 47 (26.4) |
|
Carboplatin-vinorelbine | 34 (19.1) |
|
Cisplatin-gemcitabine | 15 (8.4) |
|
Carboplatin-gemcitabine | 34 (19.1) |
|
Cisplatin-etoposide | 30 (16.9) |
| Other | 18 (10.1) |
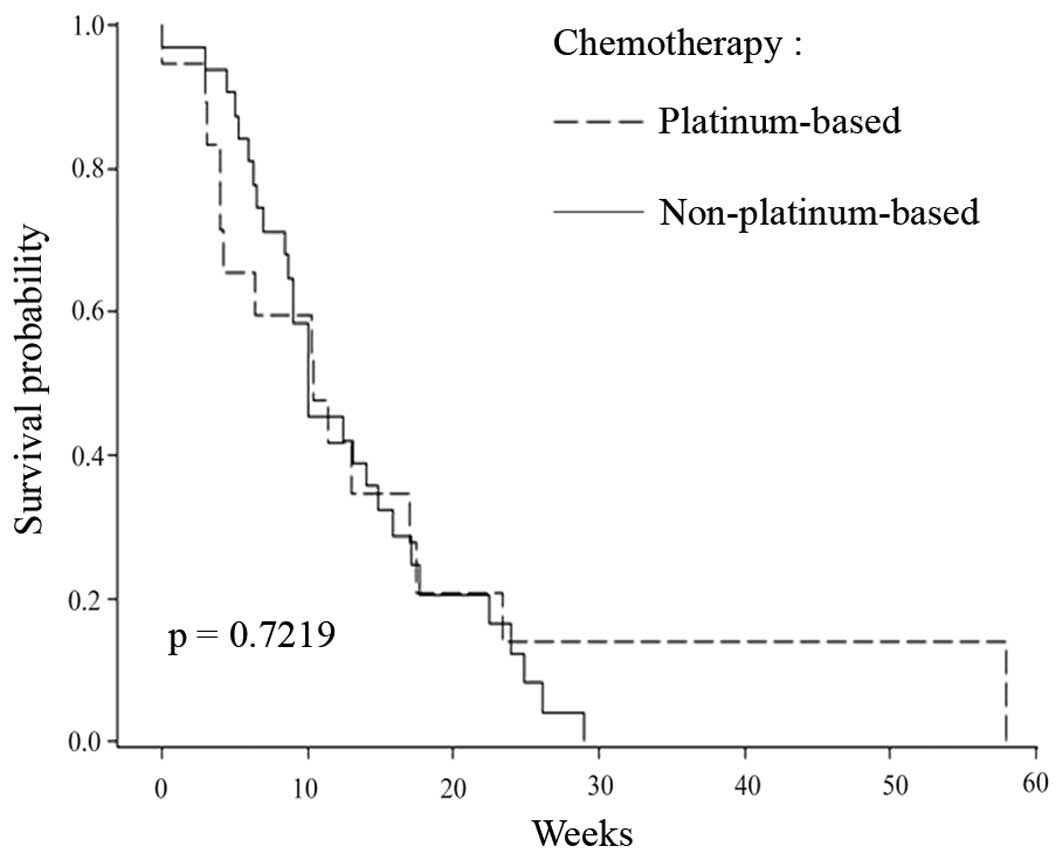
Disease progression
With respect to the cumulative incidence of disease
progression, no statistically significant differences were observed
between the use of platinum-based chemotherapy and
non-platinum-based regimens as first-line chemotherapy in patients
with TNBC (Fig. 1). By contrast, in
the non-TNBC cohort, patients who received platinum exhibited a
poorer time to progression when administered in the first-line
setting (Fig. 2).
In the two cohorts, the main reason for the
discontinuation of chemotherapy was disease progression and a
higher proportion of patients discontinued chemotherapy due to
toxicity in the TNBC cohort compared with the non-TNBC cohort
(17.1, vs. 8.9%). The median overall survival time from the time of
the diagnosis of metastatic disease was 60 weeks for the TNBC
cohort and 144 weeks for the non-TNBC cohort.
Table III presents
the results comparing platinum-based chemotherapy with
non-platinum-based regimens in the first-, second- and third-line
settings in patients with TNBC. Overall, the use of platinum-based
chemotherapy was not found to correlate with an improved time to
progression, with the adjusted HRs close to unity in the first- and
second-line settings. The adjusted HR for the third-line setting
was numerically elevated and did not reach statistical
significance, although the point estimate was likely unstable due
to the few patients in this group.
| Table IIICrude and adjusted HRs for time to
progression associated with platinum-based regimens compared with
standard chemotherapies for TNBC patients. |
Table III
Crude and adjusted HRs for time to
progression associated with platinum-based regimens compared with
standard chemotherapies for TNBC patients.
| Treatment | Cases, n | Person-time
(weeks) | Rate of progression
(per 1,000/week) | Crude HR | Adjusted HR (95%
CI)a |
|---|
| First line |
| Standard
chemotherapies | 29 | 387 | 75.0 | 1.00 | 1.00 (reference) |
| Platinum-based
chemotherapy | 15 | 241 | 62.2 | 0.89 | 0.97 (0.40–2.35) |
| Second line |
| Standard
chemotherapies | 18 | 416 | 43.3 | 1.00 | 1.00 (reference) |
| Platinum-based
chemotherapy | 22 | 599 | 36.7 | 0.81 | 0.91 (0.42–2.01) |
| Third line |
| Standard
chemotherapies | 18 | 279 | 64.4 | 1.00 | 1.00 (reference) |
| Platinum-based
chemotherapy | 13 | 143 | 90.7 | 1.30 | 2.83
(0.73–11.03) |
For patients with non-TNBC, the use of
platinum-based chemotherapy regimens in the first-line setting was
associated with a >2-fold increased risk in disease progression
(HR, 2.57; 95% CI, 1.11–5.99). In the second- and third-line
settings, the use of platinum-based chemotherapy regimens was not
found to correlate with disease progression (HR, 1.08; 95% CI,
0.53–2.18 and HR, 1.91; 95% CI, 1.00–3.63, respectively).
Discussion
Despite the aggressive phenotype, there remains no
standard chemotherapy regimen (12)
for females with metastatic TNBC. This is important from two
standpoints; firstly, the ‘best’ chemotherapy must be provided
upfront for all patients regardless of their specific phenotype. An
ongoing UK randomized, phase III Triple-Negative Breast Cancer
Trial (TNT; NCT00532727) comparing single agent carboplatin with
docetaxel for metastatic TNBC is likely to provide further
information concerning the optimal treatment options for these
patients. Secondly, in the absence of a ‘standard chemotherapy
backbone’ it is difficult to know which chemotherapy regimens to
add additional agents to in this patient population. For example,
studies with poly (ADP-ribose) polymerase (13), epidermal growth factor receptor
(14) and vascular endothelial
growth factor (15,16) inhibitors have all used various
chemotherapy backbones.
In the TNBC cohort of the present study, no observed
benefit was identified in time to progression with the use of
platinum-based chemotherapy compared with non-platinum-based
regimens. Platinum-based chemotherapy was discontinued
significantly more often due to toxicity and this must be factored
in when considering their use. The current study was unable to
determine whether platinum-based chemotherapy had an impact on
survival in TNBC as every patient received a platinum-based
chemotherapy at specific times. In addition, overall treatment for
patients within the population was extremely heterogeneous,
confounding any potential survival evaluation.
In the present study, patients with non-TNBC who
received platinum-based regimens exhibited a shorter time to
progression compared with those who received non-platinum-based
regimens, particularly in the first-line setting. No previous
randomized controlled trials have compared platinum-based
chemotherapy with non-platinum-based chemotherapy in advanced
breast cancer. Previously, in two small trials, single-agent
cisplatin showed response rates of 47 and 54%, respectively, as a
first-line treatment for advanced breast cancer (17,18).
In phase II trials of combinations of carboplatin and taxanes as a
first-line treatment for advanced breast cancer, response rates of
53–68% have been achieved (19).
The results of the current study indicate that platinum-based
chemotherapy may be inferior to non-platinum-based chemotherapy in
non-TNBC.
The current study had limitations; firstly, as with
any observational study, residual confounding may have been
present. Considering that the population was a subset of patients
observed at the cancer center who had received platinum-based
therapy, there is the potential for a selection bias, which may
affect the validity of the results. Secondly, the overall sample
size was small and thus, the study was likely underpowered for the
second- and third-line analyses, where the predicted benefits of
chemotherapy greatly diminished. In addition, considering that
chemotherapy is less effective in later lines of treatment compared
with earlier lines, small differences between platinum- and
non-platinum-based regimens may not have been detected in analysis.
Finally, time to progression was not based on the Response
Evaluation Criteria In Solid Tumors criteria and hence, a more
pragmatic time to progression calculation was required.
Despite study limitations, the results of the
current study indicate that platinum-based chemotherapy is not the
‘magic bullet’ for TNBC and that it appears to offer no significant
advantage compared with more standard non-platinum-based regimens.
In addition, platinum-based chemotherapy appears to correlate with
a higher rate of discontinuation due to toxicity compared with
other regimens. By contrast, platinum-based chemotherapy may be
less effective compared with non-platinum-based regimens in
patients with non-TNBC, although this may not be ascertained with
any certainty from the current study. The prospective, randomized
TNT is likely to aid the clarification of the role of
platinum-based regimens in TNBC. The results of the current study
are not consistent with the optimism for the widespread adoption of
platinum-based chemotherapy in clinical practice.
References
|
1
|
Clemons M, Leahy M, Valle J, et al: Review
of recent trials of chemotherapy for advanced breast cancer:
studies excluding taxanes. Eur J Cancer. 33:2171–2182. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tassone P, Tagliaferri P, Perricelli A, et
al: BRCA1 expression modulates chemosensitivity of BRCA1-defective
HCC1937 human breast cancer cells. Br J Cancer. 88:1285–1291. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Foulkes WD, Smith IE and Reis-Filho JS:
Triple-negative breast cancer. N Engl J Med. 363:1938–1948. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Santana-Davila R and Perez EA: Treatment
options for patients with triple-negative breast cancer. J Hematol
Oncol. 3:422010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Byrski T, Gronwald J, Huzarski T, et al:
Pathologic complete response rates in young women with
BRCA1-positive breast cancers after neoadjuvant chemotherapy. J
Clin Oncol. 28:375–379. 2010. View Article : Google Scholar
|
|
6
|
Staudacher L, Cottu PH, Dieras V, et al:
Platinum-based chemotherapy in metastatic triple-negative breast
cancer: the Institut Curie experience. Ann Oncol. 22:848–856. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Silver DP, Richardson AL, Eklund AC, et
al: Efficacy of neoadjuvant Cisplatin in triple-negative breast
cancer. J Clin Oncol. 28:1145–1153. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Baselga J, Gomez P, Awada A, et al: The
addition of cetuximab to cisplatin increases overall response rate
(ORR) and progression free survival (PFS) in metastatic
triple-negative breast cancer (TNBC): Results of a randomized phase
II study (Bali-1). In: Abstract Book of the 35th ESMO congress;
2010 Oct 8–12; Milan, Italy. Annals of Oncology. 21. pp.
viii1–viii96
|
|
9
|
Isakoff SJ: Triple-negative breast cancer:
role of specific chemotherapy agents. Cancer J. 16:53–61. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kassam F, Enright K, Dent R, et al:
Survival outcomes for patients with metastatic triple-negative
breast cancer: implications for clinical practice and trial design.
Clin Breast Cancer. 9:29–33. 2009. View Article : Google Scholar
|
|
11
|
Hammond ME, Hayes DF, Dowsett M, et al:
American Society of Clinical Oncology/College Of American
Pathologists guideline recommendations for immunohistochemical
testing of estrogen and progesterone receptors in breast cancer. J
Clin Oncol. 28:2784–2795. 2010. View Article : Google Scholar
|
|
12
|
Dent R, Trudeau M, Pritchard KI, et al:
Triple-negative breast cancer: clinical features and patterns of
recurrence. Clin Cancer Res. 13:4429–4434. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
O’Shaughnessy J, Osborne C, Pippen JE, et
al: Iniparib plus chemotherapy in metastatic triple-negative breast
cancer. N Engl J Med. 364:205–214. 2011.PubMed/NCBI
|
|
14
|
Carey LA, Rugo HS, Marcom PK, et al: TBCRC
001: EGFR inhibition with cetuximab added to carboplatin in
metastatic triple-negative (basal-like) breast cancer. J Clin
Oncol. 26(Suppl 15): 10092008.
|
|
15
|
Miller K, Wang M, Gralow J, et al:
Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic
breast cancer. N Engl J Med. 357:2666–2676. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Robert NJ, Dieras V, Glaspy J, et al:
RIBBON-1: randomized, double-blind, placebo-controlled, phase III
trial of chemotherapy with or without bevacizumab for first-line
treatment of human epidermal growth factor receptor 2-negative,
locally recurrent or metastatic breast cancer. J Clin Oncol.
29:1252–1260. 2011. View Article : Google Scholar
|
|
17
|
Sledge GW Jr, Loehrer PJ Sr, Roth BJ and
Einhorn LH: Cisplatin as first-line therapy for metastatic breast
cancer. J Clin Oncol. 6:1811–1814. 1988.PubMed/NCBI
|
|
18
|
Kolarić K and Roth A: Phase II clinical
trial of cis-dichlorodiammine platinum (cis-DDP) for
antitumorigenic activity in previously untreated patients with
metastatic breast cancer. Cancer Chemother Pharmacol. 11:108–112.
1983.
|
|
19
|
Perez EA: Carboplatin in combination
therapy for metastatic breast cancer. Oncologist. 9:518–527. 2004.
View Article : Google Scholar : PubMed/NCBI
|