Introduction
Neuroendocrine tumors, which cause syndrome of
inappropriate secretion of antidiuretic hormone (SIADH), are
potentially detectable in small-cell carcinoma (SmCC) of the lung.
Up to 10% of patients with pulmonary neuroendocrine SmCC (1) and 4% of extra-pulmonary neuroendocrine
SmCC patients (2) develop SIADH. Ma
and Lei reviewed all cases (45 in total) of neuroendocrine SmCC in
the nasal cavity or paranasal sinus pathologically diagnosed over
the last 40 years. Only two of the 45 cases were reported to be
complicated with SIADH (3).
Combined SmCC, which consists of SmCC and another
histological type of carcinoma, accounts for only 5% of all SmCCs
in the lungs (4). The combination
of SmCC and adenocarcinoma is not unusual; several clinical reports
exist (5–7). However, the combination of SmCC and
squamous cell carcinoma (SqCC) has not been reported previously.
This report presents the first known case of combined SmCC and SqCC
accompanied by SIADH as a paraneoplastic syndrome. Written informed
consent was obtained from the patient.
Case report
An 80-year-old Japanese female presented with a
four-week history of right nasal discharge, nasal obstruction and
left neck swelling. The patient was a non-smoker with a history
including left traumatic blindness, chronic renal disorder
(estimated glomerular filtration rate on admission, 30.3 ml/min),
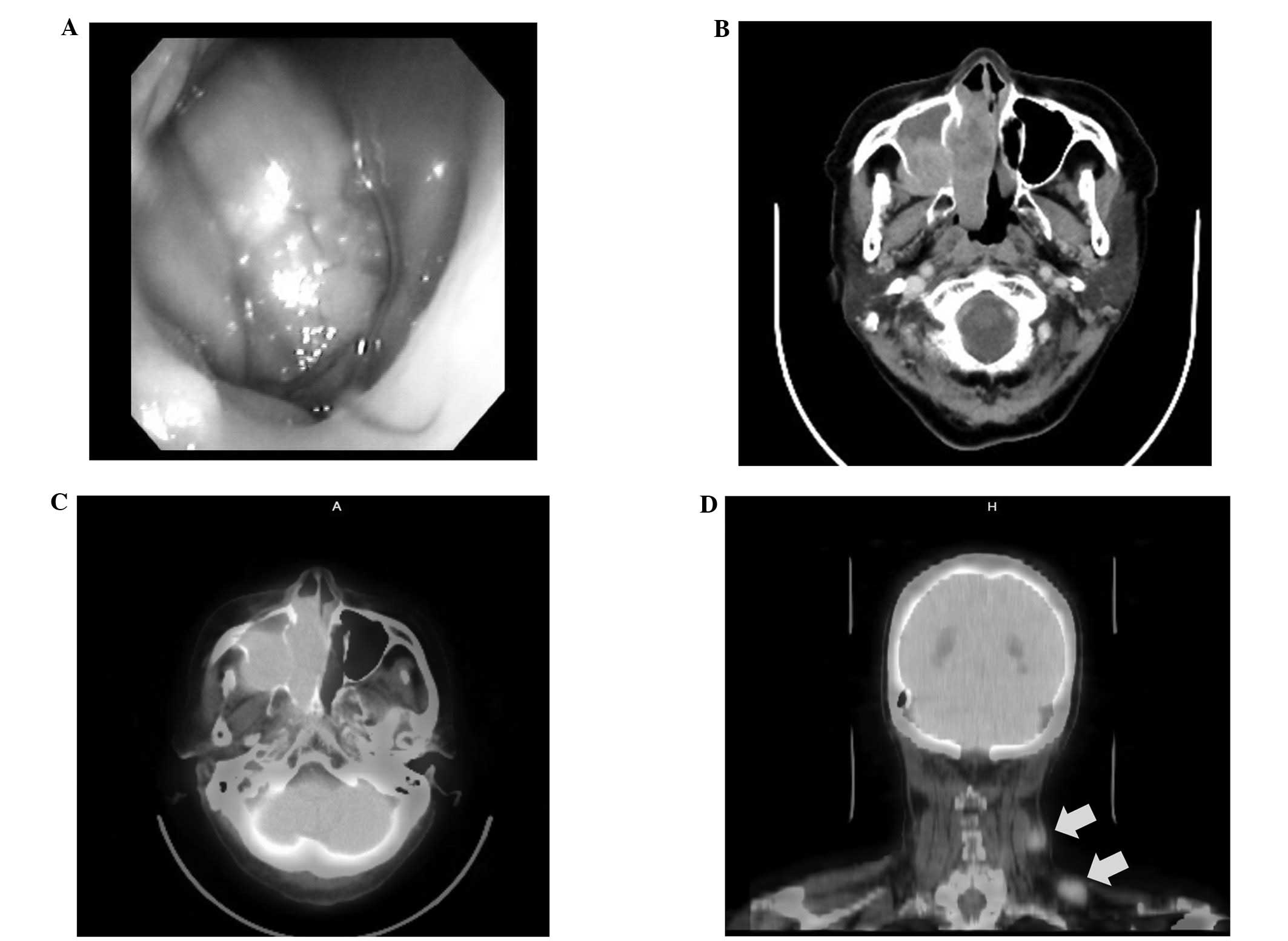
hypertension and diabetes mellitus. Physical examination
demonstrated an easy-bleeding tumor in the right nasal cavity
(Fig. 1A) and swelling of the left
medial and inferior cervical lymph nodes (diameter, 3 and 2 cm,
respectively).
Computed tomography scanning revealed a huge lesion
occupying the nasal cavity and paranasal sinus that had destroyed
the posterior and medial walls of the maxillary antrum (Fig. 1B). There was direct extension into
the right ethmoidal air cells, but no extension to the floor of the
orbit, skull base or hard palate. Fluorodeoxyglucose-positron
emission tomography (FDG-PET) showed high accumulation in the
primary tumor, with a maximum standardized uptake value
(SUVmax) of 9.63 (Fig.
1C). The SUVmax of FDG-PET in the left medial and
inferior cervical LNs was also high (6.90 and 4.62, respectively;
Fig. 1D), although there was no
definitive lesion in the right cervical LNs or distant
metastasis.
The tumor in the right nasal cavity was biopsied
using forceps, but the pathological examination resulted in
necrotic tissue with suppurative granulation. It is unclear whether
the biopsy revealed the presence of necrotic tissue or whether the
biopsy procedure itself caused the necrotic tissue. An incisional
biopsy of the left cervical lymphadenopathy and the right maxillary
antral lesion was therefore carried out via the canine fossa.
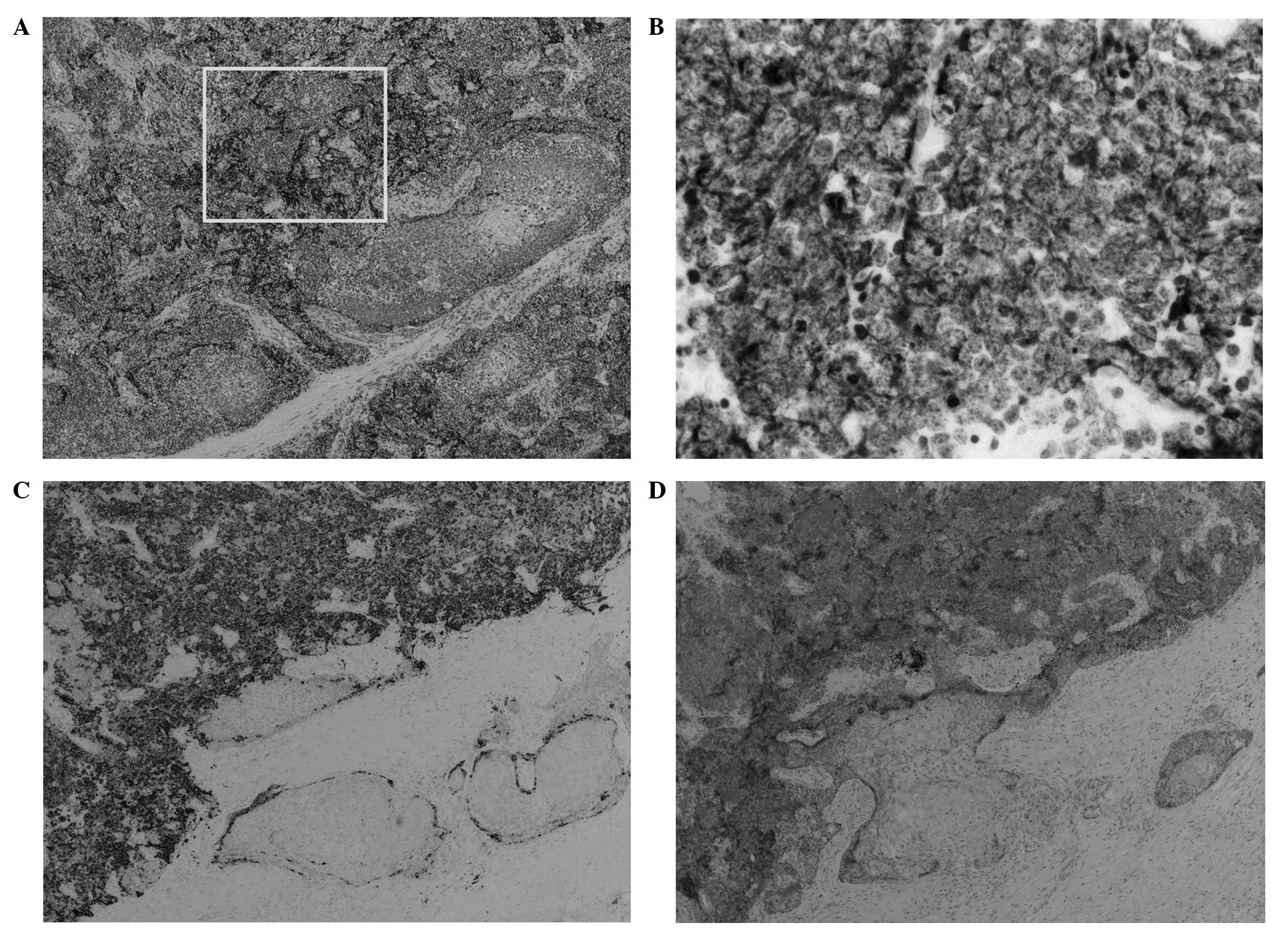
Pathological examination revealed a highly malignant anaplastic
tumor. Under hematoxylin-eosin stain, two components could be
observed in the lesions: SqCC and small cells containing
chromatin-rich nuclei with scanty cytoplasm undergoing apoptosis
and mitosis (Fig. 2A). To
characterise the cells, an immunohistochemical examination was
performed. On evaluation of specimens from the right maxillary
sinus, small cells were positive for the epithelial marker
cytokeratin CAM5.2 (Fig. 2B), and
small cells situated on the peripheral lesion were positive for
cluster of differentiation (CD)56 and synaptophysin, neuroendocrine
markers (Figs. 2C and D). Malignant
lymphoma and malignant melanoma were excluded as CD3, CD20 and
human melanoma black 45 stains were negative (data not shown).
These findings supported a diagnosis of primary combined
neuroendocrine SmCC associated with SqCC of the right maxillary
sinus. Staining of the left cervical lymph node produced similar
results. Finally, the patient was staged as T4aN2cM0 according to
the staging system established by UICC in 2009 (8). Serum levels of neuron-specific enolase
(NSE) and pro-gastrin-releasing peptide (pro-GRP), tumor markers of
small-cell carcinoma, were also elevated [NSE, 25.8 ng/ml, (normal
range, 0–12 ng/ml); pro-GRP, 152.0 pg/ml (normal range, <80.0
pg/ml)].
Following the incisional biopsy, the patient was
diagnosed with SIADH on the grounds of low sodium (124 mEq/l) with
low plasma osmolarity (271 mOsm/l), high plasma ADH levels (26.2
pg/ml; reference range, 0.3–3.5 pg/ml), high urine sodium (39
mEq/l) and high urine osmolarity (301 mOsm/l)without dehydration.
After water restriction to <1,000 ml/day, the sodium imbalance
and osmotic status improved. To confirm the neuroendocrine
characteristics of this tumor, immunohistochemistry using the
rabbit polyclonal anti-human ADH antibody (diluted 1:400; Abcam
Inc., Cambridge, UK) was performed; however, the tumor was negative
for ADH immunostaining (data not shown). Two weeks after the
biopsy, the patient complained of progressive loss of vision in the
right eye, induced by tumor extension to the right orbit. Curative
treatments, including surgery, irradiation and/or chemotherapy,
were not prescribed due to high performance status (grade 3) and
severe complicated diseases. Instead, palliative treatments were
administered. The patient succumbed to cachexia five months after
diagnosis.
Discussion
Carcinoma of the nasal cavity and paranasal sinus is
relatively rare, reported to comprise only 3% of all malignant head
and neck diseases (9). Among such
sinonasal cancers, SmCC is rarer still, and only 45 cases have been
reported (3,5). In addition, there have been no reports
of the combination of SmCC and SqCC in the nasal cavity and
paranasal sinus.
Combined SmCC is a histological group of carcinomas
in which SmCC and non-SmCC, including SqCC or adenocarcinoma, are
mixed. In contrast to head and neck cancers, the neuroendocrine
type of combined SmCC has been frequently reported in SmCC of the
lung. To the best of our knowledge, 17 cases of combined SmCC with
SqCC in the larynx (10) and four
cases of combined SmCC with adenocarcinoma in the sinonasal tract
have been reported (5–7). This is the first report to describe
combined SmCC with SqCC in the sinonasal tract.
According to the 2005 WHO pathological
classification of tumors of the head and neck (11), neuroendocrine tumors are extremely
rare in the sinonasal tract. The neuroendocrine type of SmCC was
not described in the chapter on the sinonasal tract, but rather
classified under the larynx. The pathology in this case was similar
to combined SmCC of the larynx. An important differential diagnosis
is olfactory neuroblastoma. SmCC is characterized by the marked
appearance of crushed nuclei, which is different to olfactory
neuroblastoma. In addition, olfactory neuroblastoma does not
coexist with SqCC. Thus, a diagnosis of olfactory neuroblastoma was
rejected in favor of combined SmCC.
Hyponatremia due to SIADH is a well known
paraneoplastic syndrome and occurs in a variety of malignancies,
particularly small-cell lung cancer (11–15%) (1,12) and
head and neck cancer (3%) (12,13).
Indeed, several reports have demonstrated that the incidence of
SIADH in patients with SqCC of the head and neck is markedly higher
than previously recognized (13,14).
Four mechanisms exist for the overproduction of ADH, namely: i)
Ectopic ADH secretion; ii) increased hypothalamic production of
ADH-like substances in neurological disorders; iii) administration
of drugs, including chemotherapeutic agents; and iv) administration
of exogenous ADH. In this case, ADH production from either SmCC or
SqCC was not detected by immunohistochemistry, and this patient
exhibited neither intracranial invasion nor brain metastasis, and
had not received any chemotherapeutic agents. However, serum ADH
was elevated (10 times higher than normal) and the clinical data
were compatible with a diagnosis of SIADH. These findings imply
that the mechanism of SIADH in this patient is unclear, and various
factors, including other mechanisms, may be responsible for this
pathophysiological state.
Notably, several reports have described that SIADH
correlates with clinical factors, including prognosis and the
development of metastases. Hansen et al demonstrated that,
in lung SmCC, hyponatremia is an independent marker of worsening
prognosis, in addition to advanced staging, high performance status
(≥3), male gender and age >70 years (15). Furthermore, the inability to achieve
a normal level of plasma sodium following treatment is also a poor
survival indicator. Similarly, in SmCC of the head and neck region,
the prognosis of patients with SIADH appears to be poor (16). By contrast, List et al
revealed that the development of SIADH does not correlate with the
clinical stage or distribution of metastatic sites of SmCC
(1); thus, the relationship between
the presence of SIADH and clinical outcome remains controversial.
In the present case report, although the patient recovered
immediately from SIADH-induced hyponatremia with water restriction
therapy, the tumors progressed rapidly and invaded the right orbit
and skull base, and the patient succumbed to the disease five
months later. Further data collection from such cases is required
to elucidate the pathophysiology of malignancies associated with
SIADH.
In conclusion, this report presents the first known
case of combined SmCC and SqCC in the sinonasal tract accompanied
by SIADH. The presence of SIADH may have marked implications for
the treatment and prognosis of this disease. More studies are
required to establish the exact cause and appropriate
treatments.
References
|
1
|
List AF, Hainsworth JD, Davis BW, Hande
KR, Greco FA and Johnson DH: The syndrome of inappropriate
secretion of antidiuretic hormone (SIADH) in small-cell lung
cancer. J Clin Oncol. 4:1191–1198. 1986.PubMed/NCBI
|
|
2
|
Ibrahim NB, Briggs JC and Corbishley CM:
Extrapulmonary oat cell carcinoma. Cancer. 54:1645–1661. 1984.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ma AT and Lei KI: Small cell
neuroendocrine carcinoma of the ethmoid sinuses presenting with
generalized seizure and syndrome of inappropriate antidiuretic
hormone secretion: a case report and review of literature. Am J
Otolaryngol. 30:54–57. 2009. View Article : Google Scholar
|
|
4
|
Babakoohi S, Fu P, Yang M, Linden PA and
Dowlati A: Combined SCLC clinical and pathologic characteristics.
Clin Lung Cancer. 14:113–119. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jain R, Gramigna V, Sanchez-Marull R and
Perez-Ordoñez B: Composite intestinal-type adenocarcinoma and small
cell carcinoma of sinonasal tract. J Clin Pathol. 62:634–637. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Babin E, Rouleau V, Vedrine PO, et al:
Small cell neuroendocrine carcinoma of the nasal cavity and
paranasal sinuses. J Laryngol Otol. 120:289–297. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Silva EG, Butler JJ, Mackay B and Goepfert
H: Neuroblastomas and neuroendocrine carcinomas of the nasal
cavity: a proposed new classification. Cancer. 50:2388–2405. 1982.
View Article : Google Scholar
|
|
8
|
International Union Against Cancer (UICC).
TNM Classification of Malignant Tumours. 7th edition. Sobin LH,
Gospodarowicz MK and Wittekind C: Wiley-Blackwell; Oxford: pp.
46–50. 2009
|
|
9
|
Goel R, Ramalingam K, Ramani P and
Chandrasekar T: Sino nasal undifferentiated carcinoma: A rare
entity. J Nat Sci Biol Med. 3:101–104. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Aggarwal G, Jackson L and Sharma S:
Primary combined small cell carcinoma of larynx with lateralized
histologic components and corresponding side-specific neck nodal
metastasis: report of a unique case and review of literature. Int J
Clin Exp Pathol. 4:111–117. 2010.
|
|
11
|
Perez-Ordonez B: Neuroendocrine
carcinomas. World Health Organization Classification of Tumours.
Pathology and Genetics of Head and Neck Tumours. Barnes L, Eveson
J, Peichart P and Sidransky D: IARC Press; Lyon: pp. 26–27.
2005
|
|
12
|
Sørensen JB, Andersen MK and Hansen HH:
Syndrome of inappropriate secretion of antidiuretic hormone (SIADH)
in malignant disease. J Intern Med. 238:97–110. 1995.
|
|
13
|
Talmi YP, Hoffman HT and McCabe BF:
Syndrome of inappropriate secretion of arginine vasopressin in
patients with cancer of the head and neck. Ann Otol Rhinol
Laryngol. 101:946–949. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ferlito A, Rinaldo A and Devaney KO:
Syndrome of inappropriate antidiuretic hormone secretion associated
with head neck cancers: review of the literature. Ann Otol Rhinol
Laryngol. 106:878–883. 1997. View Article : Google Scholar
|
|
15
|
Hansen O, Sørensen P and Hansen KH: The
occurrence of hyponatremia in SCLC and the influence on prognosis:
a retrospective study of 453 patients treated in a single
institution in a 10-year period. Lung Cancer. 68:111–114. 2010.
|
|
16
|
Mineta H, Miura K, Takebasyashi S, et al:
Immunohistochemical analysis of small cell carcinoma of the head
and neck: a report of four patients and a review of sixteen
patients in the literature with ectopic hormone production. Ann
Otol Rhinol Laryngol. 110:76–82. 2001. View Article : Google Scholar
|