Introduction
There are two divergent treatment pathways for the
comprehensive treatment of brain metastases and primary
glioneuronal tumors. The two tumor types must be considered in the
context of the overall clinical status of the patient, for example
the patient’s age and neurological function. In the case of
metastatic tumors, the systemic disease burden, number of cerebral
lesions and their location must also be taken into account. With
glial tumors, radiological findings may provide specific
information indicating the tumor grade, but definitive diagnosis
and classification by the World Health Organization criteria
requires, at a minimum, tissue biopsy for histopathological
examination (1). Only after
pathological confirmation may an appropriate plan of treatment be
formulated based on classification criteria (2).
Certain primary brain tumors have shown responses to
chemotherapeutic agents, for example temozolomide, that are highly
dependent on the methylation status of tumor-associated genes,
including O6-methylguanine-DNA methyltransferase
(3,4). The role of cytoreductive surgery in
the management of a number of gliomas remains the subject of
debate, however, surgery is often recommended for management of
tumor-related mass effects (5,6).
Fractionated radiotherapy remains the mainstay of radiation-based
treatment, due to the infiltrative nature of glioneuronal tumors.
By contrast, metastatic tumors are often treated using a multimodal
approach that includes surgery, stereotactic radiosurgery and
radiotherapy, with a much smaller role for chemotherapy (7,8). The
role of radiosurgery in the management of metastatic tumors has
increased exponentially in the past 15 years, in response to
experience and success with this mode of treatment. Microsurgery is
usually reserved for surgically accessible symptomatic lesions
causing clinically significant mass effects. The use of
microsurgery alone leads to unacceptably high local failure rates
and radiotherapy is often necessary in conjunction with surgery for
treating metastatic tumors. Considering the markedly different
treatment options for these diseases, a clear differential
diagnosis is necessary to provide the appropriate clinical care.
This study was deemed to be non-human research by the Institutional
Review Board of Penn State Hershey Medical Center (Hershey, USA).
Standard procedural consent was obtained from the patient for the
blood draw and lumbar puncture.
Case report
A 36-year-old Caucasian female identified a lump in
the upper outer quadrant of the left breast and axilla in February
2011. An ultrasound-guided left breast and lymph node biopsy in
March revealed the presence of an estrogen receptor-positive and
progesterone- and human epidermal growth factor receptor 2-negative
poorly differentiated invasive ductal carcinoma. Additional
immunohistochemical study results were consistent with a basal-like
phenotype and the patient was found to have an IVS12+2del21
mutation in the breast cancer 1 (BRCA1) gene. Dose-dense adriamycin
and cytoxan, followed by dose-dense paclitaxel (the two regimens
every 2 weeks), were administered between April and August 2011.
Following completion of chemotherapy, the patient underwent
mastectomy of the left breast, axillary lymph node dissection and
prophylactic right mastectomy in September 2011. A complete
pathological response was observed.
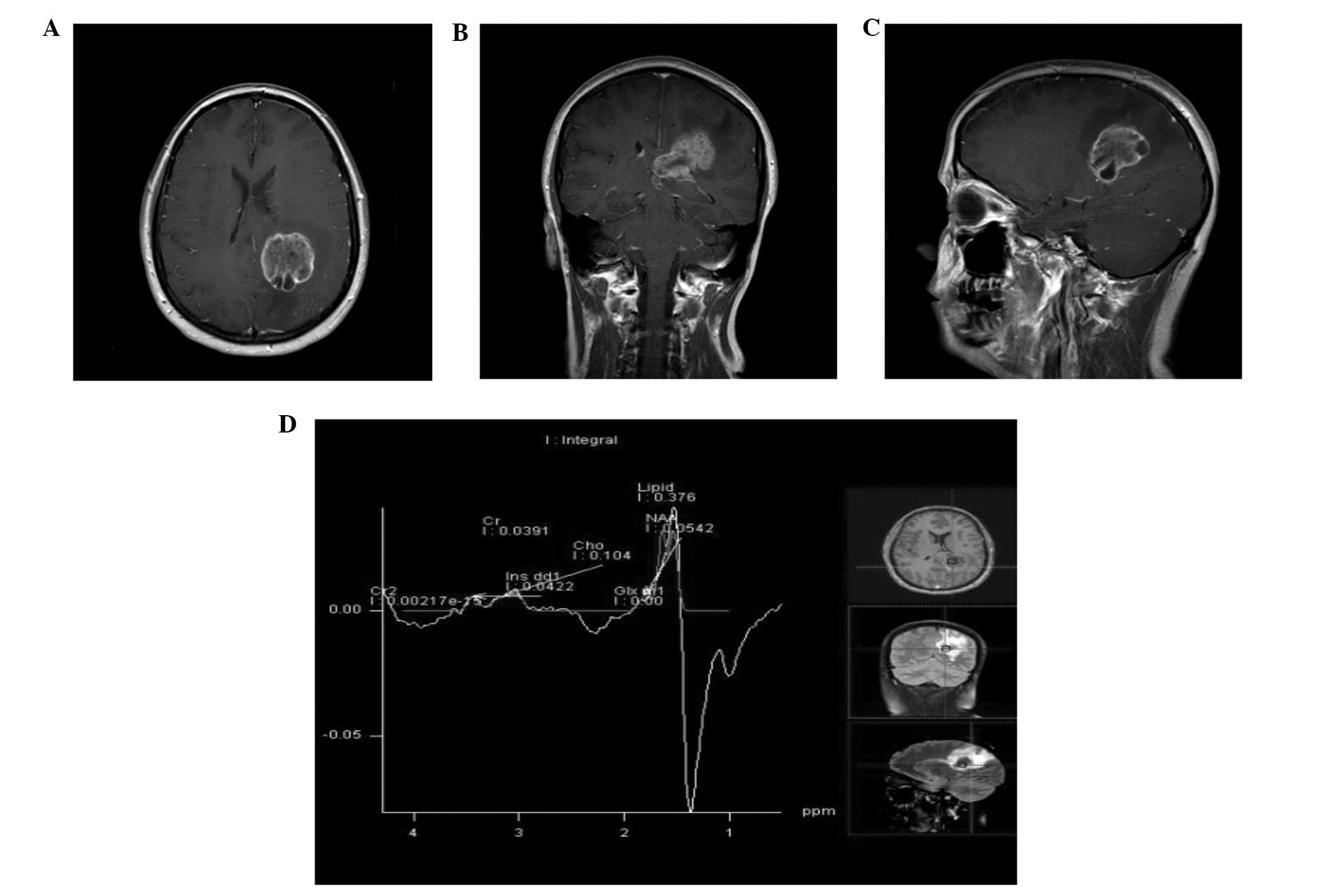
Postoperatively, chest wall radiation and a
bilateral oophorectomy were performed. In early April 2012, the
patient began to experience increasingly severe occipital and neck
pain, followed by increasingly prominent impairment of balance and
gait. Gadolinium-enhanced magnetic resonance imaging of the brain
revealed a large (4.4×3.2×4.2 cm) peripherally enhancing and
centrally necrotic mass centered in the left parietal lobe,
extending across the corpus callosum into the right hemisphere
(Fig. 1). A positive emission
tomography-computed tomography scan demonstrated no evidence of
disease outside the nervous system. Based on the lesion’s
radiographic appearance, the neuroradiologist hypothesized that it
may represent a solitary metastasis or a malignant primary
glioma.
The brain is a relatively common site of metastasis
for breast cancer and patients with a BRCA1-mutant form may be more
likely to develop brain metastases than non-carriers (9). By applying a well-validated nomogram,
designed to predict the likelihood of subsequent brain metastases
in patients with metastatic breast cancer (10), the current case report estimated the
risk of brain metastases in the patient to be ~14%. The patient was
referred to radiation oncology and neurosurgery. Given the vastly
different treatment algorithms for metastatic breast cancer and
malignant gliomas, confirmation of the nature of the mass was
requested. Magnetic resonance spectroscopy was performed, but was
unable to definitively resolve this ambiguity.
In an attempt to shed light on this diagnostic
dilemma, the patient’s blood and cerebrospinal fluid (CSF) were
tested for the presence of circulating tumor cells (CTCs) with the
CellSearch system (Janssen Diagnostics LLC, South Raritan, NJ,
USA), using standard and adapted instructions reported previously
(11). This technique requires
expression of the epithelial cell adhesion molecule (EpCAM) for
detection, which is not expressed by glial cells. Therefore, tumor
cells of glial origin are not detected by this method. However,
breast tumor cells are readily detectable, as previously
demonstrated (11). CTCs were not
detected in the peripheral blood of the patient but 6,703
EpCAM-positive tumor cells in 9 ml CSF were detected. This strongly
suggests that the tumor was of epithelial rather than glial
origin.
The patient underwent two lumbar punctures and
pathology confirmed the presence of malignant cells by cytological
examination. Next, the patient received fractionated external beam
radiation to the lesion, placement of a right frontal ventricular
access device and intrathecal chemotherapy. The initial agents used
were liposomal cytarabine, topotecan, methotrexate and etoposide.
Under conditions where a clear diagnosis was not made, the patient
may have undergone two very different treatment algorithms,
particularly with regards to chemotherapy and radiation.
Discussion
The biology of CTCs remains an active area of study.
The early stages of cancer spread may be due to micro-metastases
seeding the blood and circulating until the appropriate ‘soil’ is
found (12). Previous clinical
studies have demonstrated the prognostic value of CTCs in several
metastatic solid tumors, including breast cancer, as well as
their use in monitoring tumor response to therapy (13,14).
The CellSearch system is a fully automated system that relies on
immunomagnetic enrichment with EpCAM-labeled iron oxide
nanoparticles. Subsequent identification criteria include nuclear
DNA and expression of cytokeratin and cluster of differentiation
45. The final step involves analysis of the cells by trained
personnel to ensure that only cells with the appropriate
cytomorphological characteristics are counted.
The CellSearch system was designed to use blood as
the biological matrix, although a modification of the system
utilizing CSF was previously reported (11). This adapted protocol permits tumor
cells to be accurately and sensitively counted in the CSF of
patients with breast cancer metastases in the central nervous
system, without detecting glial cells. Previous studies have
indicated that the number of tumor cells correlates with the
magnitude of disease (11). The
current case study demonstrates the use of a ‘liquid biopsy’
protocol to enumerate cells in the patient’s CSF to provide
diagnostic information, in addition to the magnitude of metastatic
disease burden. Thus, this case report has extended the clinical
utility of the liquid biopsy technique.
In conclusion, the ability of the CellSearch system
to detect cells of epithelial origin was utilized in order to
resolve a diagnostic dilemma involving a patient with a brain
lesion without systemic disease but with prior poorly
differentiated invasive ductal carcinoma that completely resolved
following surgery and treatment. Distinguishing the origins of
brain lesions is particularly complex when the patient has had a
prior systemic disease that responded completely to therapy, which
increases the probability of the lesion representing a metastatic,
rather than a primary tumor. The impact of utilizing this technique
to distinguish the tumor origin, as was the case for this
situation, is particularly high when different diagnoses lead to
considerably different treatment options.
Acknowledgements
This study was supported by startup funds to Dr
Wafik El-Deiry from the Penn State Hershey Cancer Institute. Dr
El-Deiry is an American Cancer Society Research Professor.
References
|
1
|
Louis D, Ohgaki H, Wiestler O, et al: The
2007 WHO classification of tumours of the central nervous system.
Acta Neuropathol. 114:97–109. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ohgaki H and Kleihues P: Genetic pathways
to primary and secondary glioblastoma. Am J Pathol. 170:1445–1453.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Martinez R and Esteller M: The DNA
methylome of glioblastoma multiforme. Neurobiol Dis. 39:40–46.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Weller M, Stupp R, Reifenberger G, et al:
MGMT promoter methylation in malignant gliomas: ready for
personalized medicine? Nat Rev Neurol. 6:39–51. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ammirati M, Vick N, Liao YL, Ciric I and
Mikhael M: Effect of the extent of surgical resection on survival
and quality of life in patients with supratentorial glioblastomas
and anaplastic astrocytomas. Neurosurgery. 21:201–206. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kelly PJ and Hunt C: The limited value of
cytoreductive surgery in elderly patients with malignant gliomas.
Neurosurgery. 34:62–67. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bindal RK, Sawaya R, Leavens ME and Lee
JJ: Surgical treatment of multiple brain metastases. J Neurosurg.
79:210–216. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Brown PD, Brown CA, Pollock BE, Gorman DA
and Foote RL: Stereotactic radiosurgery for patients with
‘radioresistant’ brain metastases. Neurosurgery. 51:656–667.
2002.
|
|
9
|
Albiges L, André F, Balleyguier C,
Gomez-Abuin G, Chompret A and Delaloge S: Spectrum of breast cancer
metastasis in BRCA1 mutation carriers: highly increased incidence
of brain metastases. Ann Oncol. 16:1846–1847. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Graesslin O, Abdulkarim BS, Coutant C, et
al: Nomogram to predict subsequent brain metastasis in patients
with metastatic breast cancer. J Clin Oncol. 28:2032–2037. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Patel AS, Allen JE, Dicker DT, et al:
Identification and enumeration of circulating tumor cells in the
cerebrospinal fluid of breast cancer patients with central nervous
system metastases. Oncotarget. 2:752–760. 2011.PubMed/NCBI
|
|
12
|
Fidler IJ: The pathogenesis of cancer
metastasis: the ‘seed and soil’ hypothesis revisited. Nat Rev
Cancer. 3:453–458. 2003.
|
|
13
|
Allen JE and El-Deiry WS: Circulating
tumor cells and colorectal cancer. Curr Colorectal Cancer Rep.
6:212–220. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cristofanilli M, Hayes DF, Budd GT, et al:
Circulating tumor cells: A novel prognostic factor for newly
diagnosed metastatic breast cancer. J Clin Oncol. 23:1420–1430.
2005. View Article : Google Scholar : PubMed/NCBI
|