Introduction
Prostate cancer is known clinically as a
heterogeneous disease, characterized by biological behavior that
ranges between indolent and aggressive states. Although the initial
diagnosis of prostate cancer is relatively straightforward, as it
is based on prostate-specific antigen (PSA) screening and
confirmatory biopsy, the accurate staging and detection of
recurrent and metastatic disease remains clinically challenging.
Post-therapeutic biochemical failure in prostate cancer represents
a diagnostic dilemma to urologists, oncologists and
radiologists.
Fluorine-18 fluorodeoxyglucose (FDG) positron
emission tomography (PET)-computed tomography (CT) has been widely
used for diagnosis, initial staging, restaging, monitoring of
therapeutic response and prognostication in various types of
cancer, however, its role in prostate cancer remains controversial.
The small number of previously published observations indicated
that unlike the majority of malignancies, prostate tumors are
characterized by slow glycolysis and low FDG-avidity on PET images
(1,2). Significant overlap has been identified
between FDG uptake in prostate cancer and benign prostate
hyperplasia. An additional confounding problem is that FDG is
normally excreted by the kidneys and intense activity in the
distended urinary bladder usually obscures the prostate and
interferes with the identification of pelvic lymph nodes (1–4).
Therefore, application of FDG PET-CT in prostate cancer is
generally discouraged.
The purpose of the present retrospective study was
to evaluate the diagnostic value of FDG PET-CT in prostate cancer,
with an emphasis on the detection of metastatic disease.
Patients and methods
Ethics
The present retrospective study was approved by the
Institutional Review board of the University of Medicine and
Dentistry of New Jersey (Newark, NJ, USA). The relevant cases were
identified and selected from a computerized database of patients
who underwent FDG PET-CT imaging at the Advanced Imaging Center,
University Hospital (Newark, NJ, USA) between January 2006 and
December 2011. The medical records were retrospectively reviewed
for pathological, therapeutic and radiological information.
Patients
In total, 25 relevant cases of patients with newly
diagnosed prostate cancer, referred for staging (nine cases), or
with a history of prostate cancer or recent PSA relapse, referred
for detection of metastatic disease (16 cases), were included. None
of the patients had known imaging or pathological evidence of
metastatic disease prior to FDG PET-CT, however, the PSA levels had
been recorded in all patients within two months prior to FDG PET-CT
imaging. In total, 12 patients with imaging that suggested
metastatic disease prior to FDG PET-CT were excluded from the
analysis. An additional 15 cases were excluded from the study for
the following reasons: i) No data were available at the time of FDG
PET-CT imaging, including Gleason score at diagnosis, detailed
therapeutic history or PSA levels prior to FDG PET-CT; ii) no
further confirmatory tests were available following a positive FDG
PET-CT; and iii) cases with concurrent prostate cancer and other
malignancies, for instance, an additional tumor other than prostate
cancer, such as lung or colon cancer, or lymphoma, were referred
for FDG PET-CT.
Combined FDG PET-CT
Combined FDG PET-CT was performed using a PET-CT
scanner (Discovery LS; GE Healthcare, Amersham, UK) and standard
techniques. The maximum standardized uptake value
(SUVmax) of lesions was recorded. The definition of a
positive scan was that the observations were consistent with that
of a malignant or metastatic disease. By contrast, a negative scan
indicated no apparent abnormalities and the observations were not
indicative of a malignancy. The interpretation criteria for the
positive FDG PET-CT imaging were as follows: i) Focal uptake with
an SUVmax of >3.0 in the prostatic fossa; ii) nodal
SUVmax of >3.0 regardless of its size; iii) sclerotic
or lytic osseous lesion with an SUVmax of >3.0; and
iv) other CT identified and FDG-avid lesions with an
SUVmax of >3.0. Non-FDG-avid lymph nodes and bone
lesions were interpreted as negative.
Verification of FDG PET-CT
observations
The nine patients for initial staging all underwent
prostate biopsy and were diagnosed with cancer prior to FDG PET-CT.
In addition, one patient in the restaging group underwent prostate
biopsy following a positive imaging observation in the prostatic
fossa. For metastatic lesions that were identified by FDG PET-CT,
confirmatory biopsies were performed in three cases (lymph node
dissection, lung lesion resection and bone biopsy). All other
patients underwent further verification imaging studies within the
following three months after positive or negative FDG PET-CT
studies, with the exception of one patient with negative FDG PET-CT
in the restaging group. For the initial staging and restaging
cases, regional diagnostic CT (predominantly abdomen and pelvis)
was performed if the FDG PET-CT indicated nodal metastasis.
Regional diagnostic CT and/or whole-body bone scintigraphy were
performed if FDG PET-CT indicated bone metastasis and diagnostic CT
of the abdomen and pelvis was performed if FDG PET-CT was negative
for metastatic disease.
Statistical analysis
A paired t-test was used to perform the for
statistical analyses. P<0.05 was considered to indicate a
statistically significant difference.
Results
Patient characteristics
Table I summarizes
the characteristics of 25 eligible patients, including PSA level,
Gleason score, FDG PET-CT observations and confirmatory or
verification methods. The patients were divided into two groups,
initial staging and restaging.
 | Table IPatient characteristics and FDG PET-CT
observations. |
Table I
Patient characteristics and FDG PET-CT
observations.
| | | | | FDG PET-CT
observation | |
|---|
| | | | |
| |
|---|
| Patient no. | Age, years | Gleason score | Therapeutic
history | PSA on imaging,
ng/ml | Prostatic fossa | Lymph nodes | Bone (or other) | Confirmatory
test |
|---|
| 1 | 59 | 7 | Initial staging | 6.8 | − | + | + | BS and CT |
| 2 | 61 | 9 | Initial staging | 14 | − | + | − | CT and PLND |
| 3 | 52 | 6 | Initial staging | 49 | + | − | − | CT and BS |
| 4 | 50 | 7 | Initial staging | 6.1 | − | − | − | CT and BS |
| 5 | 73 | 8 | Initial staging | 680 | + | + | + | CT and BS |
| 6 | 69 | 6 | Initial staging | 9.6 | − | − | − | CT |
| 7 | 53 | 8 | Initial staging | 511 | − | + | + | BS and CT |
| 8 | 59 | 7 | Initial staging | 369 | − | − | + | BS and CT |
| 9 | 71 | 9 | Initial staging | 980 | + | + | + | BS and CT |
| 10 | 64 | 6 | Prostatectomy | 3.1 | − | − | + | BS and CT |
| 11 | 63 | 6 | Prostatectomy | 22.5 | − | + | − | CT |
| 12 | 55 | 8 | Prostatectomy | 10.7 | − | + | − | CT |
| 13 | 70 | 7 | Prostatectomy | 67 | − | − | + | BS and CT |
| 14 | 72 | 6 | Prostatectomy | 15.4 | − | − | + (lung) | Lung Bx |
| 15 | 64 | 6 | Prostatectomy | 3.8 | − | − | − | CT and repeat
PET |
| 16 | 68 | 7 | Prostatectomy | 14 | − | − | + | Bx |
| 17 | 72 | 7 | Prostatectomy | 8.4 | − | − | + | CT |
| 18 | 67 | 8 | Hormone | 11.5 | − | − | + | BS and CT |
| 19 | 60 | 9 | Brachytherapy | 15.7 | − | − | + | BS and CT |
| 20 | 70 | 8 | Brachytherapy | 5.5 | − | − | − | CT |
| 21 | 72 | 7 | Brachytherapy | 7.8 | + | − | − | Bx |
| 22 | 77 | 7 | Brachytherapy | 4.8 | − | − | − | None |
| 23 | 64 | 7 | Hormone + XRT | 41 | − | + | − | CT |
| 24 | 62 | 7 | Hormone + XRT | 680 | − | + | + | BS and CT |
| 25 | 57 | 8 | Orchiectomy +
XRT | 671 | + | + | + | BS and CT |
FDG PET-CT for initial staging of
prostate cancer
Nine patients were in the initial staging group,
with a mean age of 61±9 years (range, 50–73 years) and a mean PSA
level of 291±363 ng/ml (range, 6.1–980 ng/ml). All patients had
been newly diagnosed with prostate cancer by prostatic biopsy. FDG
PET-CT demonstrated abnormal uptake of the prostate in only three
cases and no abnormal prostate uptake was observed in the remaining
six cases, including two cases with PSA levels of 511 and 369
ng/ml. However, FDG PET-CT successfully detected metastatic lesions
in the lymph nodes and/or bones of six cases.
FDG PET-CT for patients with
post-therapeutic biochemical recurrence
In total, 16 patients were included in the restaging
group with a mean age of 66±6 years (range, 55–72 years) and a mean
PSA level of 99±225 ng/ml (range, 3.1–680 ng/ml). Eight patients
had undergone radical prostatectomy and eight had received
prostate-preserving treatments, such as brachytherapy, hormonal
therapy or hormone combined with radiation therapy. FDG PET-CT only
detected two recurrences within the prostate and recurrence in one
patient was confirmed by prostatic biopsy. By contrast, FDG PET-CT
identified metastatic diseases in 12 patients, which were confirmed
by biopsy, diagnostic CT and/or bone scintigraphy in the subsequent
three months. Of these 12 patients, six exhibited bone lesions,
three exhibited nodal lesions, two exhibited bone and nodal
diseases, and one exhibited lung metastasis. FDG PET-CT failed to
detect an abnormality in three patients, of which two were found to
exhibit enlarged pelvic nodes on the follow-up CT one month later;
one patient (patient 22) did not undergo further imaging.
Role of FDG PET-CT in prostate
cancer
In nine newly diagnosed prostate cancer patients,
the sensitivity of FDG PET-CT in identifying untreated primary
lesions was only 33% (3/9). However, FDG PET-CT detected metastatic
disease in six of the nine patients who underwent initial staging.
Out of 16 patients with previous treatments and recent PSA relapse,
FDG PET-CT successfully identified metastatic diseases in 12 and
tumor recurrence within the prostatic fossa of two patients, one of
which exhibited prostate cancer recurrence and metastasis. The
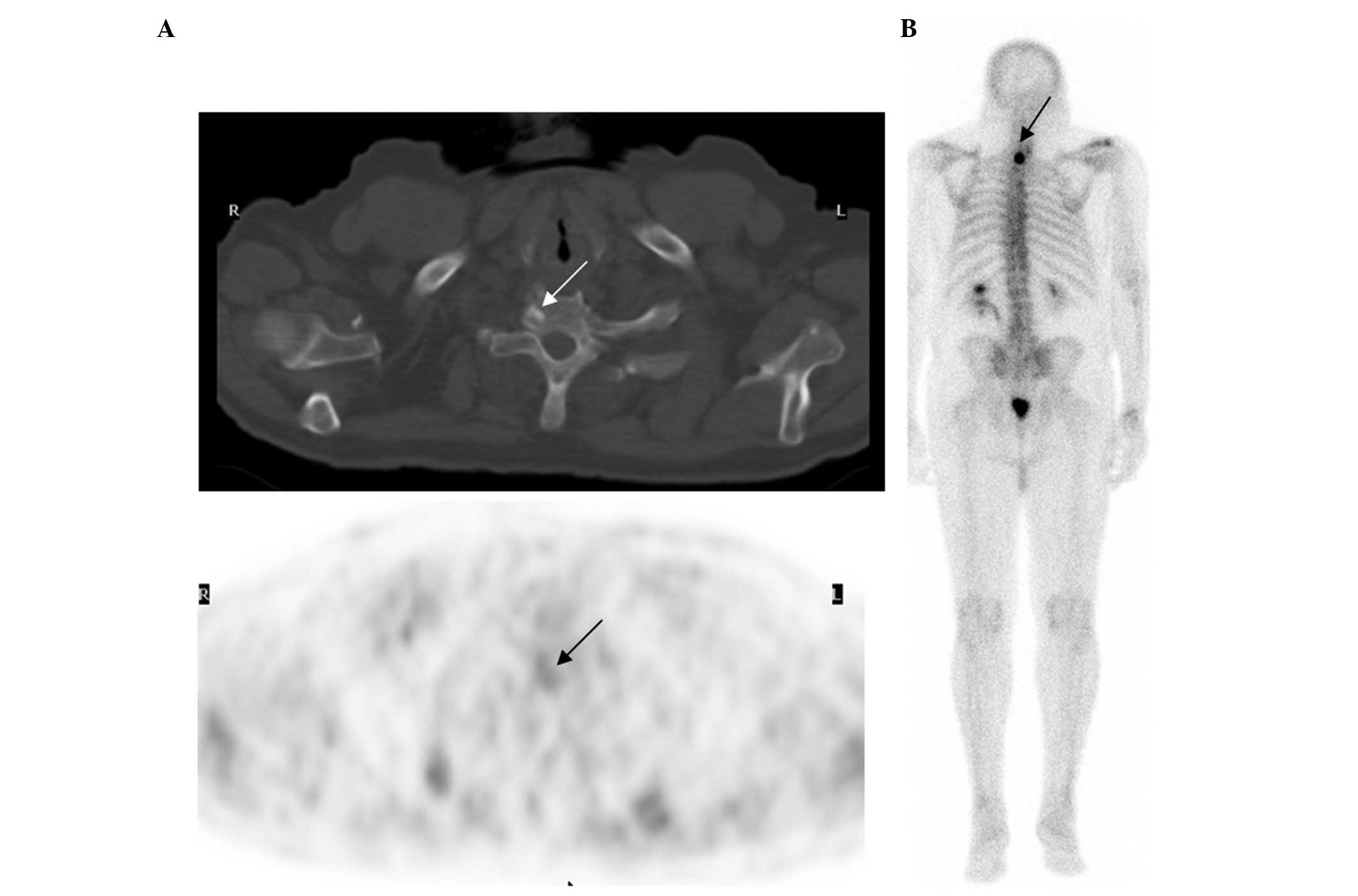
positive rate of FDG PET-CT was 81% (13/16). Fig. 1 shows an example of the role of FDG
PET-CT in the detection of metastatic disease in prostate cancer.
Five years following radical prostatectomy, a 70-year-old male
(patient 13) exhibited a PSA relapse of 67 ng/ml. The first bone
scintigraphy and pelvic CT were obtained for the initial workups
one month prior to FDG PET-CT and the two were negative. FDG PET-CT
demonstrated a small sclerotic density with mild uptake
(SUVmax, 3.5) that indicated metastasis in the
right-side of the T1 vertebral body. Repeat bone scintigraphy that
was conducted one month later confirmed the FDG PET-CT-identified
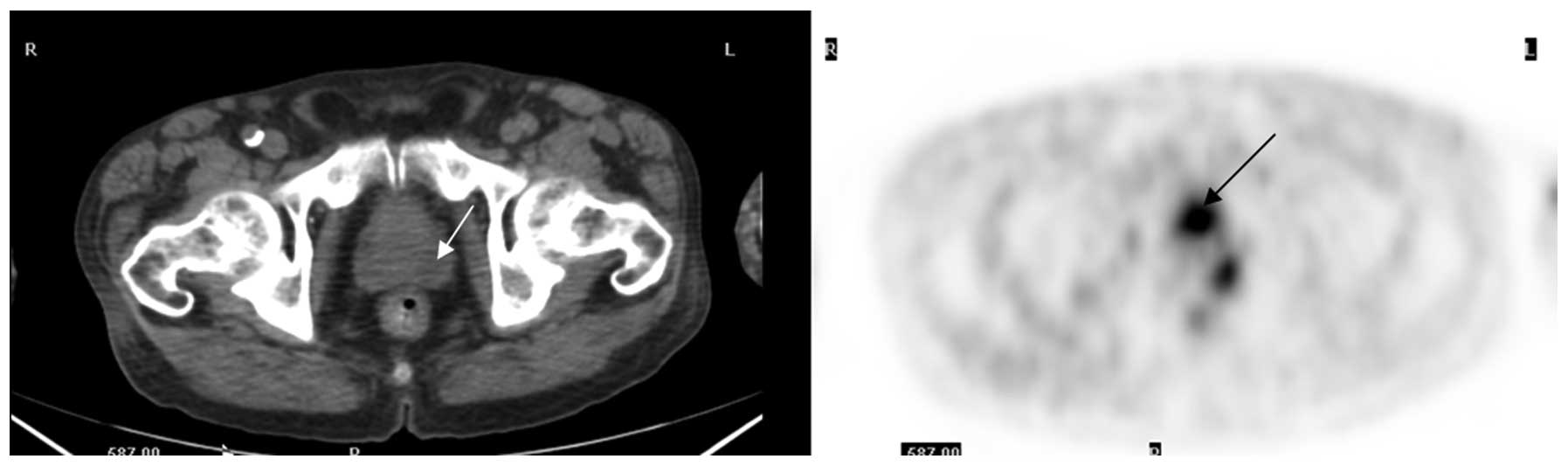
lesion. Fig. 2 shows transaxial FDG
PET-CT images obtained from a 72-year-old male post external beam
radiotherapy for prostate cancer (patient 21). The patient’s series
PSA levels were unremarkable until two years later when the PSA
level was 7.8 ng/ml. FDG PET-CT demonstrated an FDG-avid lesion in
the left-side of the prostate, which was confirmed as recurrent
adenocarcinoma via a transrectal biopsy.
Correlation between PSA levels and
positive FDG PET-CT studies
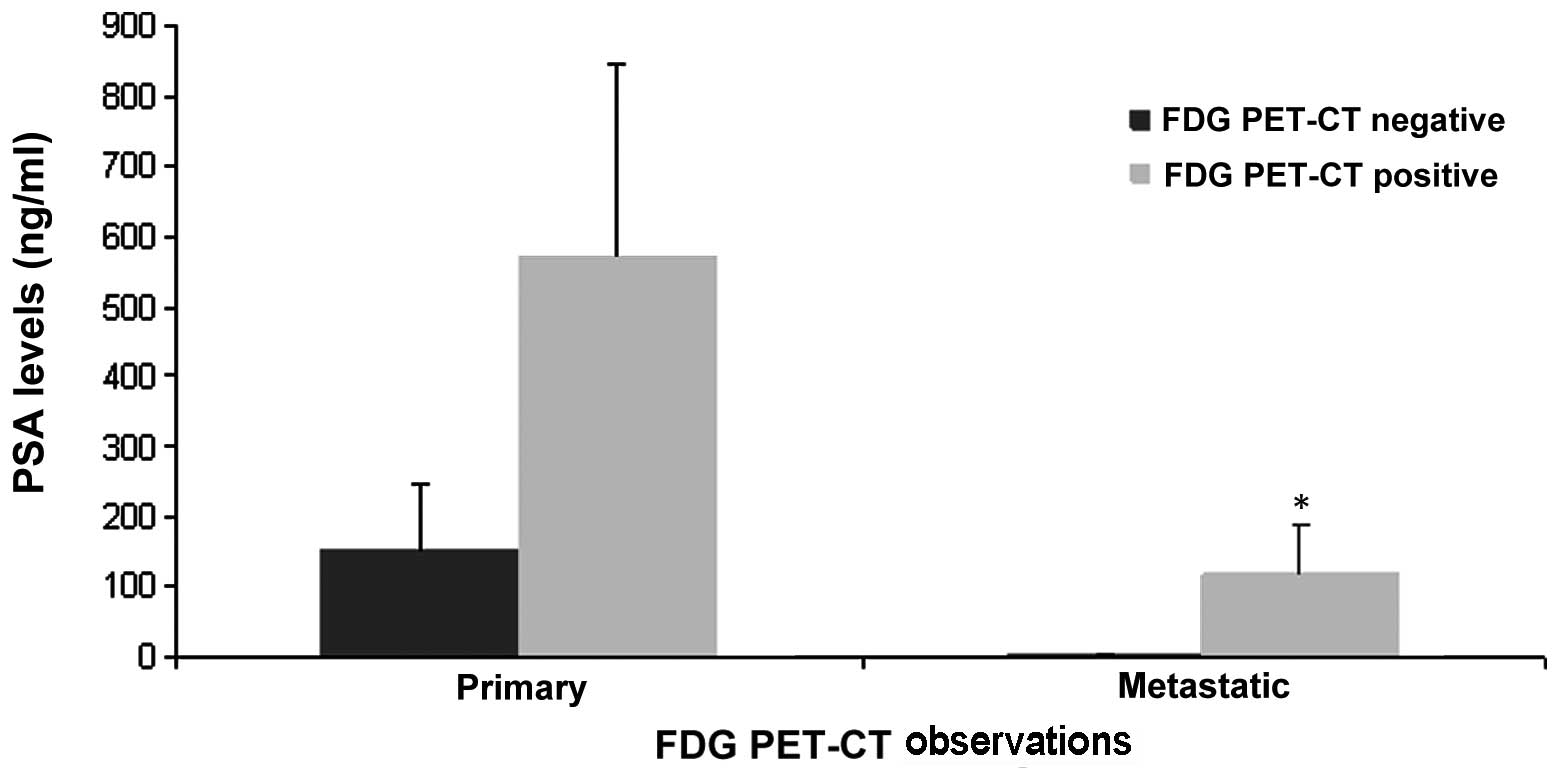
Fig. 3 represents
the mean PSA levels in all subgroups of the patients. For primary
prostate tumors in the initial staging group, the mean PSA levels
were 153±92 ng/ml in the FDG PET-CT-negative cases and 570±274
ng/ml in the FDG PET-CT-positive cases. Statistical analysis
identified no significant difference in the initial serum PSA
levels between patients with positive and negative FDG PET-CT for
primary prostate lesions. The reason for this insignificant
difference may be due to the wide variation in the range of PSA
levels and the small case number. However, no abnormal uptake was
identified in the prostate of the two patients with PSA levels of
369 and 511 ng/ml.
The mean PSA levels in the restaging (metastatic)
group were 4.7±0.49 ng/ml in patients with negative FDG PET-CT
scans (three cases) and 120±68 ng/ml in patients with positive FDG
PET-CT scans (13 cases). The difference in the PSA levels was
identified to be statistically significant (P<0.05) between the
two subgroups of the restaging patients.
Discussion
FDG is a non-physiological compound with a chemical
structure extremely similar to that of naturally occurring glucose.
Similarly to glucose, FDG enters the cells through membrane glucose
transporter proteins, which are commonly overexpressed in cancer
cells (5). FDG is actively
transported into the cell through the membrane glucose transporters
and converted into FDG-6-phosphate by hexokinase. Since
FDG-6-phosphate is not a substrate for the enzyme responsible for
the next step in glycolysis, it is then trapped and accumulates in
the cell in proportion to its glucose metabolic activity. Malignant
cells exhibit increased FDG accumulation due to increased membrane
transporters, increased intracellular hexokinase and low levels of
glucose-6-phosphatase (5,6).
A limited number of previous studies demonstrated a
low sensitivity of FDG PET-CT in the detection of primary prostate
cancer, indicating that FDG PET-CT may not be useful in the
diagnosis or staging of clinically organ-confined disease (7). Previously, Oyama et al
(8) reported a 64% sensitivity of
FDG PET-CT in detecting primary prostate cancer; however, the
subjects in the study exhibited high serum PSA levels (mean PSA
level, 251 ng/ml), as well as advanced stage and aggressive cancer.
Liu et al (9) previously
reported that FDG PET-CT only exhibited 4% sensitivity in detecting
prostate cancer among 24 patients, with a mean serum PSA level of
13.6 ng/ml. In addition, Minamimoto et al (10) reported a 51.9% sensitivity of FDG
PET-CT in 50 subjects with increasing PSA levels that were
suspected of having prostate cancer. The results showed that FDG
PET-CT was appropriate for detecting peripheral zone prostate
cancer in patients that were considered to exhibit more than an
intermediate risk. The results of the current study showed only 33%
sensitivity of FDG PET-CT for identifying primary prostate lesions
in newly diagnosed patients, which is consistent with the
previously described observations. Although high PSA levels are
likely to increase the possibility of FDG-avidity of primary
tumors, no statistical difference was identified between the two
subgroups of patients in the current series due to the small case
number.
The low sensitivity of FDG PET-CT in identifying
prostate cancer is considered to be predominantly due to the slow
rate of glycolysis of tumor cells as a result of relatively slow
tumor growth. Previous laboratory studies have revealed that
glucose transporter mRNA and protein are only weakly expressed in
human prostate cancer tissues, which is considered to account for
its low FDG-avidity (11). A
previous in vitro study also indicated that glucose may not
be required for androgen-dependent prostate cancer cells since
LNCaP cells grow at controlled rates even in a medium containing
only 0.05 g/l glucose (12). In
addition, Liu et al (13)
reported that all benign and malignant prostate cells are
characterized by a dominant uptake of fatty acid compared with
glucose.
Information on lymph node status is important when
planning appropriate treatment for patients with newly diagnosed
prostate cancer. Although conventional imaging modalities, such as
CT and magnetic resonance imaging (MRI), are often used to detect
nodal disease, previous observations have indicated that FDG PET-CT
is more sensitive than anatomic imaging in the detection of nodal
metastasis. Heicappell et al (14) investigated the use of FDG PET in
determining pelvic lymph node metastases and found that FDG PET was
positive in four of the six patients with histologically confirmed
lymph node spread, which was a superior outcome compared with the
CT imaging. In the present study, FDG PET-CT identified five cases
with nodal disease in the nine patients that were newly diagnosed
with prostate cancer, including two cases with distant nodal
lesions in the mediastinum and neck. In addition, five patients
were found to exhibit osseous metastasis on FDG PET-CT. It is clear
that FDG PET-CT has an advantage, with regards to whole-body data
acquisition and ability to detect more distant or unexpected
lesions, compared with a regional diagnostic CT or MRI.
Post-therapeutic biochemical failure in prostate
cancer represents a diagnostic dilemma and poses a great challenge
to urologists and oncologists. FDG PET-CT has shown a promising
role in the detection of local recurrence or metastatic disease. In
a previous study of 24 patients with rising PSA levels following
treatment for localized prostate cancer, CT and FDG PET-CT were
obtained prior to pelvic lymph node dissection (15). The CT was negative in all cases,
whereas FDG PET-CT detected 75% of histopathologically proven
metastases. The sensitivity, specificity, accuracy and positive and
negative predictive values of FDG PET-CT in detecting metastatic
pelvic lymph nodes were 75, 100, 83, 100 and 68%,
respectively. In an additional retrospective study of 91 patients
with PSA relapse following prostatectomy, and validation of tumor
presence by biopsy or clinical and imaging follow-up, FDG PET-CT
detected local or systemic disease in 31% of patients (16). In the current case series, FDG
PET-CT detected metastatic diseases and less frequently, recurrent
prostate lesions, in 81% (13/16) of patients, which significantly
contributed to the patient management. The majority of metastases
were identified in the lymph nodes and bone. The sites of osseous
metastases were randomly distributed, the most common being the
spine and pelvis. In addition, the majority of lymph node lesions
were located in the pelvis and lower abdomen, although nodal
lesions in a few cases were detected in the upper torso, such as
the mediastinum or neck. The results demonstrated a promising role
of FDG PET-CT in the detection of metastatic disease. Clearly, the
present results showed a higher positive rate of FDG PET-CT to
detect metastatic disease than that which was previously reported
(16). The reason of this
difference is likely to be secondary to the selection of the
patients; mean PSA levels were 99±225 ng/ml in the current study,
but only 11±10 ng/ml in the previously published cases (16).
The present study demonstrated that FDG PET-CT has a
much higher sensitivity for the detection of metastatic lesions
than for primary prostate cancer, which may result from the
progression of the energetic metabolism in metastatic lesions
compared with the primary lesion; increased cell proliferation and
accelerated glucose metabolism. A previous in vitro study
indicated that the level of expression of glucose transporter 1 was
higher in the poorly differentiated cell lines, DU-145 and PC-3,
than in the well-differentiated hormone-sensitive LNCaP cell line,
demonstrating that glucose metabolism increases with the
progression of malignancy (17).
While PSA levels are not definitely associated with
positive FDG PET-CT observations for primary prostate lesions, high
PSA levels in restaging may predict a positive FDG PET-CT scan for
metastatic and/or recurrent disease. In the restaging group, all
three patients with negative FDG PET-CT exhibited low PSA levels
(4.7±0.49 ng/ml), whereas the patients with positive scans
exhibited much higher PSA levels (mean, 120±68 ng/ml) with only
three cases with a PSA of <10 ng/ml.
In recent years, much effort has been made to
develop novel radiotracers for PET imaging of prostate cancer, such
as tracers that identify cell membrane turnover, protein synthesis,
DNA synthesis and testosterone metabolism within the prostate,
however, they each have certain limitations in clinical
applications (18–20). As the only readily available PET
tracer on the market worldwide, the role of FDG in PET imaging of
prostate cancer cannot be ignored purely based on the limited
number of previous negative observations. FDG PET-CT is useful for
the detection of metastatic disease in prostate cancer in certain
patient groups, such as those with high PSA levels.
The present study was retrospective and a major
limitation was referral bias. Since FDG PET-CT is not a routine or
standard imaging modality in prostate cancer, only patients with a
high pretest possibility of metastasis were referred for FDG PET-CT
by the urologist or oncologist, which may account for the high PSA
levels and high positive rate of metastatic disease in the patients
of the present study. In addition, following the exclusion of cases
without detailed historical information, particularly PSA levels
two months prior to FDG PET-CT imaging, the total case number was
small, which limited the statistical power of the data.
In conclusion, FDG PET-CT may impact the clinical
management of patients with prostate cancer, although this impact
may be lower than that for other cancers. Although FDG PET-CT has a
low sensitivity for identifying primary prostate lesions and is not
useful for the diagnosis of prostate cancer, it may aid in the
detection of metastatic disease in appropriately selected patients.
In patients with post-therapeutic PSA relapse, FDG PET-CT has a
clear role in the detection of metastatic lesions, particularly in
those with high PSA levels. Furthermore, FDG PET-CT has the
advantage of whole-body data acquisition and the ability to detect
more distant or unexpected lesions compared with a regional
diagnostic CT or MRI.
References
|
1
|
Ravizzini G, Turkbey B, Kurdziel K and
Choyke PL: New horizons in prostate cancer imaging. Eur J Radiol.
70:212–226. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Powels T, Murray I, Brock C, Oliver T and
Avril N: Molecular positron emission tomography and PET/CT imaging
in urological malignancies. Eur Urol. 51:1520–1521. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lawrentschuk N, Davis ID, Bolton DM and
Scott AM: Positron emission tomography and molecular imaging of the
prostate: an update. BJU Int. 97:923–931. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Effert PJ, Bares R, Handt S, Wolff JM,
Büll U and Jakse G: Metabolic imaging of untreated prostate cancer
by positron emission tomography with 18fluorine-labeled
deoxyglucose. J Urol. 155:994–998. 1996. View Article : Google Scholar
|
|
5
|
Kapoor V, McCook BM and Torok FS: An
introduction to PET-CT imaging. Radiographics. 24:523–543. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu Y, Ghesani NV and Zuckier LS:
Physiology and pathophysiology of incidental findings detected on
FDG-PET scintigraphy. Semin Nucl Med. 40:294–315. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hofer C, Laubenbacher C, Block T, Breul J,
Hartung R and Schwaiger M: Fluorine-18-fluorodeoxyglucose positron
emission tomography is useless for the detection of local
recurrence after radical prostatectomy. Eur Urol. 36:31–35. 1999.
View Article : Google Scholar
|
|
8
|
Oyama N, Akino H, Suzuki Y, Kanamaru H,
Sadato N, Yonekura Y and Okada K: The increased accumulation of
[18F]-fluorodeoxyglucose in untreated prostate cancer. Jpn J Clin
Oncol. 29:623–629. 1999.
|
|
9
|
Liu IJ, Zafar MB, Lai YH, Segall GM and
Terris MK: Fluorodeoxyglucose positron emission tomography studies
in diagnosis and staging of clinically organ-confined prostate
cancer. Urology. 57:108–111. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Minamimoto R, Uemura H, Sano F, Terao H,
Nagashima Y, Yamanaka S, Shizukuishi K, Tateishi U, Kubota Y and
Inoue T: The potential of FDG-PET/CT for detecting prostate cancer
in patients with an elevated serum PSA level. Ann Nucl Med.
25:21–27. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Candler JD, Williams ED, Slavin JL, Best
JD and Rogers S: Expression and localization of GLUT1 and GLUT12 in
prostate carcinoma. Cancer. 97:2035–2042. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Singh G, Lakkis CL, Laucirica R and Epner
DE: Regulation of prostate cell division by glucose. J Cell
Physiol. 180:431–438. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liu Y, Zuckier LS and Ghesani NV: Dominant
uptake of fatty acid over glucose by prostate cells: a potential
new diagnostic and therapeutic approach. Anticancer Res.
30:369–374. 2010.PubMed/NCBI
|
|
14
|
Heicappell R, Müller-Mattheis V, Reinhardt
M, Vosberg H, Gerharz CD, Müller-Gärtner H and Ackermann R: Staging
of pelvic lymph nodes in neoplasms of the bladder and prostate by
positron emission tomography with 2-[(18)F]-2-deoxy-D-glucose. Eur
Urol. 36:582–587. 1999.
|
|
15
|
Chang CH, Wu HC, Tsai JJ, Shen YY,
Changlai SP and Kao A: Detecting metastatic pelvic lymph nodes by
18F-2-deoxyglucose positron emission tomography in patients with
prostate-specific antigen relapse after treatment for localized
prostate cancer. Urol Int. 70:311–315. 2003. View Article : Google Scholar
|
|
16
|
Schöder H, Herrmann K, Gönen M, Hricak H,
Eberhard S, Scardino P, Scher HI and Larson SM:
2-[18F]fluororo-2-deoxyglucose positron emission tomography for the
detection of disease in patients with prostatic-specific antigen
relapse after radical prostatectomy. Clin Cancer Res. 11:4761–4769.
2005.
|
|
17
|
Effert P, Beniers AJ, Tamimi Y, Hardt S
and Jakse G: Expression of glucose transporter 1 (Glut-1) in cell
lines and clinical specimens from human prostate adenocarcinoma.
Anticancer Res. 24:3057–3063. 2004.PubMed/NCBI
|
|
18
|
Shiiba M, Ishihara K, Kimura G, Kuwako T,
Yoshihara H, Sato H, Kondo Y, Tsuchiya S and Kumita S: Evaluation
of primary prostate cancer using 11C-methionine-PET/CT and
18F-FDG-PET/CT. Ann Nucl Med. 26:138–145. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jadvar H: Prostate cancer. Methods Mol
Biol. 727:265–290. 2011. View Article : Google Scholar
|
|
20
|
Bouchelouche K, Tagawa ST, Glodsmith SJ,
Turkbey B, Capala J and Choyke P: PET/CT imaging and
radioimmunotherapy of prostate cancer. Semin Nucl Med. 41:29–44.
2011. View Article : Google Scholar : PubMed/NCBI
|