Introduction
Adenoma of the nipple (AN) is a rare benign
epithelial tumor of the nipple ducts. It generally occurs
unilaterally and arises at an average age of between 43–45 years,
predominantly in females and rarely in males and adolescents
(1–3). The lesion, also known as erosive
adenoma and florid papillomatosis, appears similar to a
hard-elastic nodule that deforms the nipple, causing swelling or
erosion with serous or hematic secretion. AN is often confused with
Paget’s disease (4) and the
differential diagnosis with breast carcinoma is often difficult
(5,6).
AN appears histologically as an extremely
heterogeneous tumor entity, particularly due to the following
various patterns of growth associated with it: i) ‘sclerosing
papillomatosis pattern’, often indistinguishable from sclerosing
papilloma; ii) ‘papillomatosis pattern’, florid papillary
hyperplasia of ductal epithelium; iii) ‘adenosis pattern’, evident
myoepithelial hyperplasia; and iv) ‘mixed proliferative pattern’,
combination of three patterns (metaplasia of ducts with cysts,
apocrine metaplasia and acanthosis of the epithelium) (7).
A larger series previously reported in the
literature referred to a group of 42 American patients and a
casuistry of 18 Chinese patients (8,9),
collected over several decades, which did not include Italian
patients. Only sporadic case reports have been previously described
(2,10).
The present study described a series of 13 cases of
AN with clinicopathological features, collected within a decade,
highlighting the incidence of this benign lesion in the population
of Southern Italy. In addition, the requirement of a careful
morphological analysis, associated with a relevant immunophenotypic
panel, for the recognition of this lesion and differential
diagnosis with other breast malignant neoplasms was
highlighted.
Materials and methods
Clinical information
Cases were selected from the pathological files of
the National Cancer Institute, Fondazione Pascale Hospital (Naples,
Italy) between January 2003 and April 2013. The World Health
Organization (WHO) criteria was strictly applied to establish the
diagnosis of AN. Clinical information was recovered from clinical
files and a total of 13 cases were identified. All patients signed
an informed consent form according to the institutional
regulations.
Immunophenotype analysis
The formalin-fixed, paraffin-embedded (FFPE) tissue
block specimens were sectioned (3-μm thick), deparaffinized and
rehydrated. Each section was stained with hematoxylin and eosin and
then used for immunostaining. Immunohistochemical analyses were
performed using an autostainer (BenchMark XT system; Ventana
Medical Systems, Inc., Tucson, AZ, USA) according to the
manufacturer’s instructions. The following anti-human primary
antibodies were used: p63 (Santa Cruz Biotechnology, Inc,. Santa
Cruz, CA, USA), caldesmon, calponin, α-smooth muscle actin, CD10,
cytokeratin (CK) 5/6 (DakoCytomation, Glostrup, Denmark) and CK8/18
(Novocastra, Newcastle, UK) (Table
I).
 | Table IAntibody panel for
immunohistochemistry analysis. |
Table I
Antibody panel for
immunohistochemistry analysis.
| Antibody | Source | Clone | Dilution |
|---|
| p63 | Rabbit
polyclonal | Sc-8343 | 1:200 |
| h-CALD1 | Mouse monoclonal | h-cd | 1:400 |
| Calponin | Mouse monoclonal | CALP | 1:600 |
| α-smooth muscle
actin | Mouse monoclonal | 1A4 | Prediluted |
| CD10 | Mouse monoclonal | 56C6 | 1:50 |
| CK5/6 | Mouse monoclonal | D5/16B4 | Prediluted |
| CK8/18 | Mouse monoclonal | 5D3-R-7-CE | Prediluted |
Stained sections were evaluated by two different
pathologists using uniform criteria. Discrepancies were resolved
through simultaneous evaluation and discussion of the results.
Single-marker expression was recorded as negative/positive and
high/low level, following consideration of the expression in
reactive surrounding tissue compared with tumoral cells and the
specific cut-off of each marker.
Results
Clinicopathological features
All AN patients were admitted to the National Cancer
Institute, Fondazione Pascale Hospital following a physical
examination revealing a well-defined erosive tumor, often
serousanguineous, of the breast nipple. Mammography and
ultrasonography revealed no mass lesions and calcifications in the
two breasts. In total, three cases appeared clinically as Paget’s
disease. A total excision of the nipple and areola with an
underlying portion of breast tissue was obtained. All
clinicopathological parameters of patients are included in Table II.
| Table IIClinicopathological features of
patients. |
Table II
Clinicopathological features of
patients.
| Patient | Age, years | Tumor size, cm | Growth pattern | Myoepithelial
markers | CK8/18a |
|---|
|
|---|
| p63 | CALD1 | CALP1 | M-actin | CD10 | CK5/6 |
|---|
| 1 | 38 | 0.9×1.2 | Papillomatosis
pattern | + | +/− | + | + | + | + | + |
| 2 | 20 | 0.8×1.1 | Papillomatosis
pattern | + | + | + | + | + | + | + |
| 3 | 40 | 1.6×1.3 | Papillomatosis
pattern | + | +/− | + | + | + | + | + |
| 4 | 31 | 0.7×1.5 | papillomatosis
pattern | + | +/− | − | + | + | + | + |
| 5 | 51 | 1.2×1.3 | Mixed prolif.
pattern | + | +/− | − | + | + | + | + |
| 6 | 42 | 0.7×1.1 | Papillomatosis
pattern | + | − | + | + | + | + | + |
| 7 | 37 | 1.3×0.9 | Papillomatosis
pattern | + | +/− | + | + | + | + | + |
| 8 | 37 | 0.5×1.2 | Papillomatosis
pattern | + | +/− | + | + | + | + | + |
| 9 | 31 | 1.3×1.5 | Papillomatosis
pattern | + | + | +/− | + | + | + | + |
| 10 | 44 | 0.8×1.2 | Papillomatosis
pattern | + | +/− | + | + | + | + | + |
| 11 | 44 | 1.1×1.3 | Papillomatosis
pattern | + | + | +/− | + | + | + | + |
| 12 | 42 | 0.8×1.3 | Mixed prolif.
pattern | + | + | +/− | + | + | + | + |
| 13 | 42 | 1.2×1.2 | Adenosis pattern | + | + | − | + | + | + | + |
In summary, all patients were female, with an age
range of 20–51 years and an average age of 38 years. The medium
size of the lesions was between 0.8 and 1.5 cm.
Histopathological observations
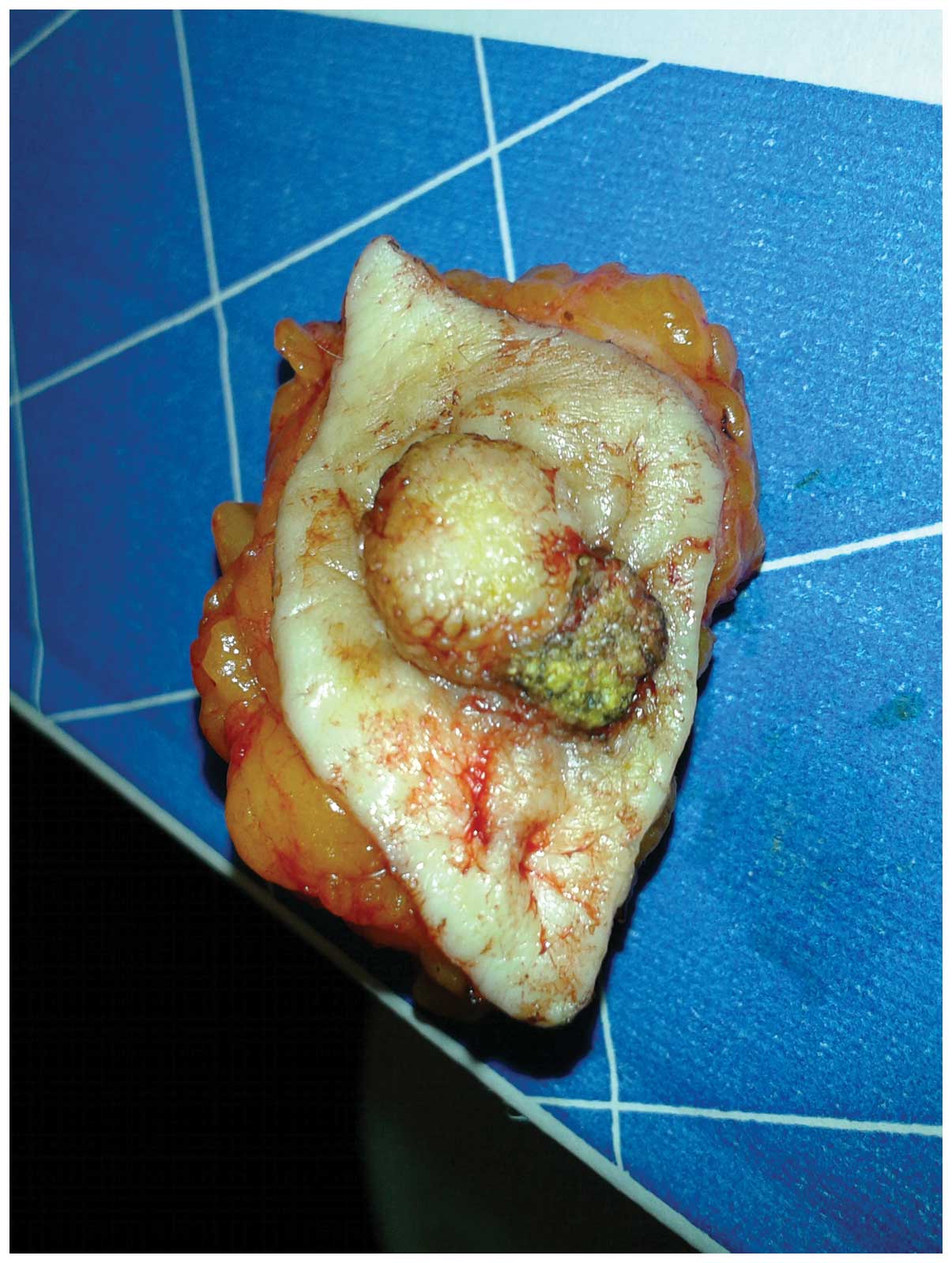
Macroscopically, all lesions presented in the
retroareolar region, with no encapsulated nodules and infiltrative
margins (Fig. 1). The presence of
adenomatous proliferation in the stroma of medium and small caliber
ducts, coated by a double layer of cells (epithelial and
myoepithelial) was detected in all samples. Only one of the 13
cases appeared with ductal carcinoma in situ (DCIS)
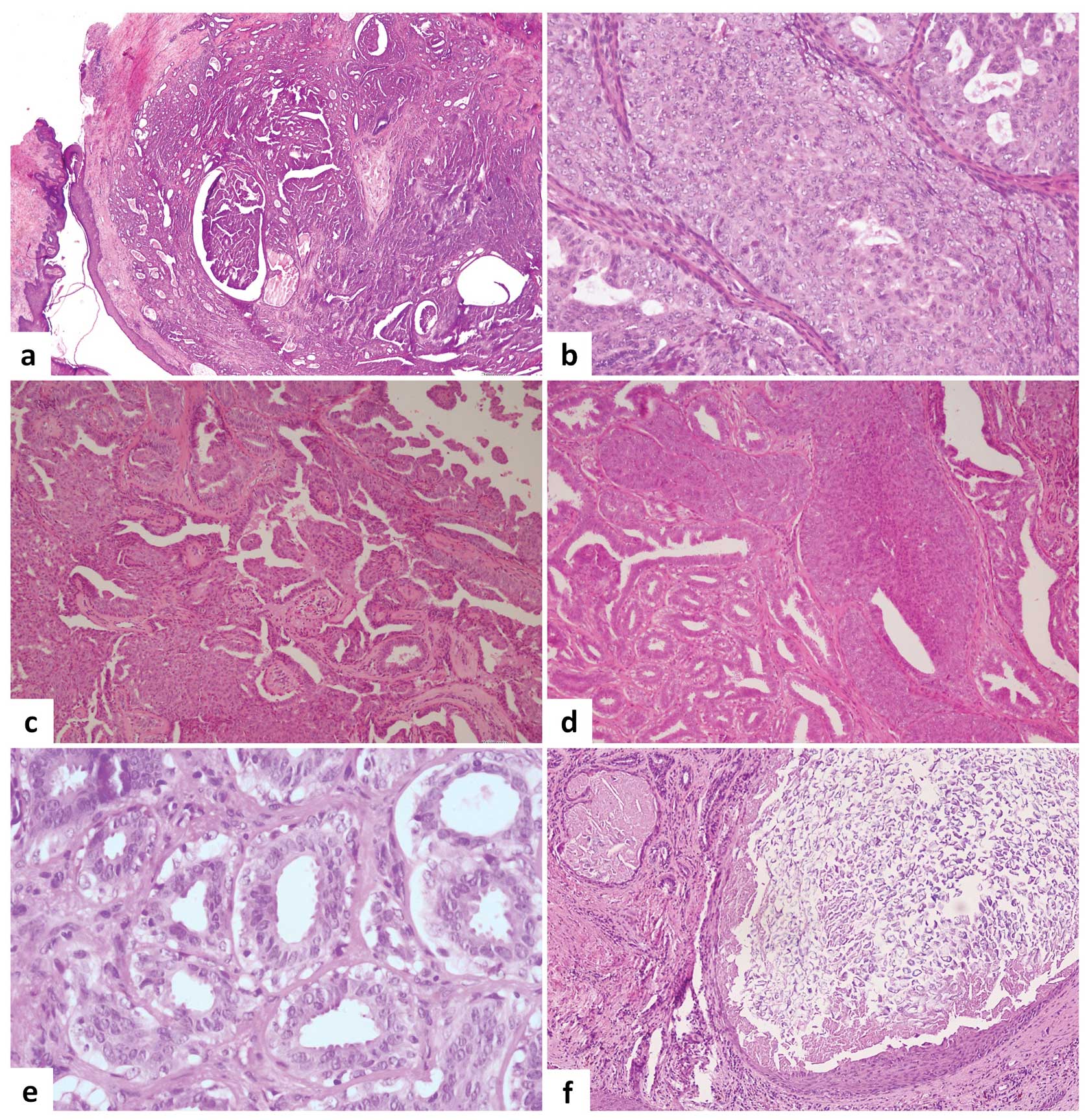
following the intraoperative examination. The histological features
of the 13 lesions were extremely variegated even when the prevalent
growth pattern was the papillomatosis pattern with a florid
papillary hyperplasia of ductal epithelium. In the majority of
cases, the following features were observed: i) presence of
fibrosis with distortion of the ducts that may simulate images of
pseudo invasion; ii) epithelial hyperplasia with a partial or total
obliteration of the lumen; iii) epithelial hyperplasia with
intraductal papillary projections; iv) presence of intraductal
necrosis; v) presence of cellular monomorphism and/or polymorphism;
vi) cellular atypia; and vii) mitosis in 50% of cases. One case
showed an adenosis pattern with myoepitelial hyperplasia and two
cases showed a mixed proliferative pattern (Fig. 2).
Immunohistochemical observations
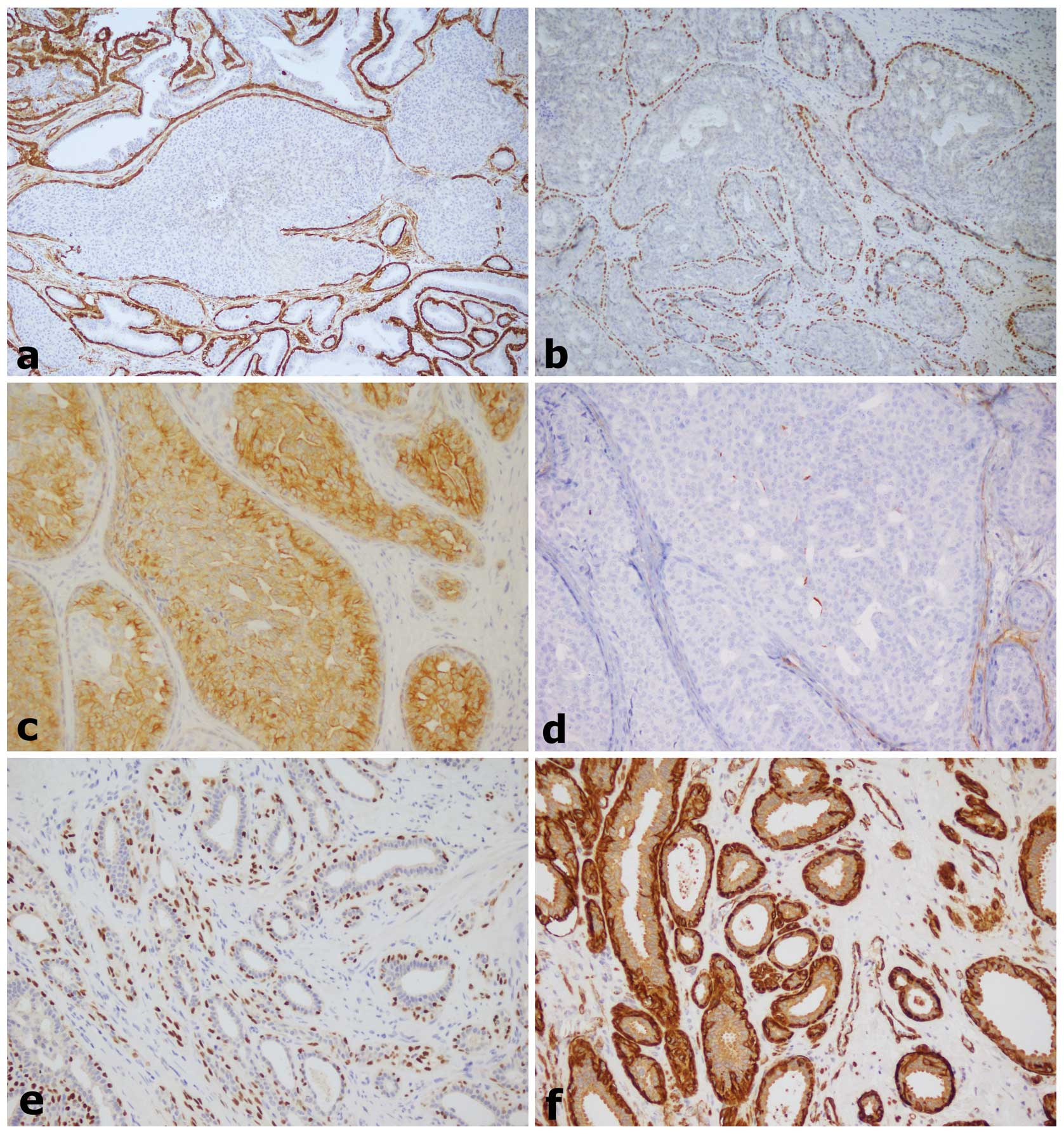
Immunohistochemical studies were performed on all AN
specimens. For epithelial cells of the inner layer of ducts, CK8/18
antibodies were used, while myoepithelial cells of the outer layer
were highlighted using antibodies against p63, caldesmon, calponin,
α-smooth muscle actin, CK5/6 and CD10.
The details of positivity/negativity for several
markers is included in Table II
and shown in Fig. 3.
Discussion
AN is a rare benign tumor of the breast, which
originates from the nipple areola complex generally between the
fourth or fifth decade of life. This lesion is almost always
unilateral and is often accompanied by a serous/hematic secretion
in the nipple. In the WHO classification, AN is defined as ‘a
compact proliferation of small tubules lined by epithelial and
myoepithelial cells, with or without proliferation of the
epithelial component, around the collecting ducts of the nipple’
(11).
However, there is considerable confusion concerning
the terms used to define this lesion, due to the diversity of
histological pattern with which it occurs. It has been defined as
erosive adenomatosis of the nipple, papillary AN, florid
adenomatosis, florid papillomatosis of the nipple, subareolar duct
papillomatosis and superficial papillary adenomatosis of the nipple
(2,8,12).
Since the main feature common to these lesions is adenomatous
proliferation in the stroma (small and medium caliber duct
proliferation) (1,4), the definition of AN was preferred in
the current study.
Although AN are rare and benign entities, the main
issue with these lesions is the differential diagnosis with nipple
Paget’s disease (clinical and histological diagnosis), DCIS of
low-grade, tubular carcinoma, infiltrating syringomatous adenoma
and solitary central papilloma subareolar (histological diagnosis)
(7).
These lesions are characterized by the presence of
two cell populations, an internal layer of cuboidal epithelial
cells with an apocrine secretion and an external layer of
myoepithelial cells. The presence of a myoepithelial cell layer in
neoplastic ducts is considered to be the most important
histological observation for distinguishing adenoma from carcinoma.
For this reason, the correct immunophenotypic definition, through
the use of a panel of specific antibodies for the myoepithelial
cells, is always required for the differential diagnosis. Among the
frequently used myoepithelial markers are p63, h-caldesmon,
calponin 1, α-smooth muscle actin, CK5/6 and CD10 (13,14).
The positivity of at least two markers is sufficient for diagnosis.
The use of p63 has been largely discussed since it may be extremely
useful, particularly for the differential diagnosis with DCIS. In
this lesion, the expression of p63 is lost or may appear
discontinuous (15). The CK5/6, in
addition to myoepithelial cells, is also present within the
intraductal epithelial proliferation lesion. In the case of
differential diagnosis with atypical ductal hyperplasia and DCIS,
positivity for CK5/6 within the ducts is lost (14).
Cytological examination may be performed for
diagnosis, but the complete excision of the lesion and examination
of FFPE serial sections remains the gold standard for diagnosis.
Although the lesion is almost always unilateral, bilateral cases
(16,17) and association of AN with malignant
breast carcinoma (18–21) have been previously described. With
regard to the probability of a tumor developing from these lesions,
no reliable data has been identified in the previous literature
(22,23).
To date, few case studies have analyzed the numerous
individual case reports for AN. A previous case series of 15 cases
was described in 1985 by Brownstein et al (12). Subsequently, the largest case series
was presented in 1986 by Rosen and Caicco with 42 selected cases of
AN (8). Finally, a case series of
18 AN cases in the Chinese population was described (9). No previous studies have analyzed the
incidence of this lesion in Italy. Since 2002, only single case
reports have been presented (2,10).
In the present study, a case series of 13 patients
was selected from the National Cancer Institute of Fondazione
Pascale Hospital database. This was collected within ten years and
represented a female population from the Campania region of
Southern Italy. The range of ages of the patients recruited in the
study corresponds with that described in the previous literature
and the mean age was ~38 years. In addition, the growth pattern
frequently found was the papillomatosis pattern with a florid
papillary hyperplasia of ductal epithelium. All lesions presented
were unilateral and not associated with other malignant diseases of
the breast. In all analyzed cases, the definition of the
immunophenotypic profile was essential for the correct
diagnosis.
In conclusion, although AN may be diagnosed
preoperatively by cytological examination and core biopsy, complete
excision of the lesion and an adequate histological and
immunophenotypic analysis is recommended. This is necessary to
discriminate the pseudo invasive pattern that often characterizes
this lesion from breast cancer precursors and aggressive
carcinoma.
References
|
1
|
Fernandez-Flores A and Suarez-Peñaranda
JM: Immunophenotype of nipple adenoma in a male patient. Appl
Immunohistochem Mol Morphol. 19:190–194. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tuveri M, Calò PG, Mocci C and Nicolosi A:
Florid papillomatosis of the male nipple. Am J Surg. 200:e39–e40.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ishii N, Kusuhara M, Yasumoto S and
Hashimoto T: Adenoma of the nipple in a Japanese man. Clin Exp
Dermatol. 32:448–449. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Healy CE, Dijkstra B, Walsh M, Hill AD and
Murphy J: Nipple adenoma: a differential diagnosis for Paget’s
disease. Breast J. 9:325–326. 2003.
|
|
5
|
Aftab K and Idrees R: Nipple adenoma of
breast: a masquerader of malignancy. J Coll Physicians Surg Pak.
20:472–474. 2010.PubMed/NCBI
|
|
6
|
Da Costa D, Taddese A, Cure ML, Gerson D,
Poppiti R Jr and Esserman LE: Common and unusual diseases of the
nipple-areolar complex. Radiographics. 27(Suppl 1): S65–S77.
2007.PubMed/NCBI
|
|
7
|
Rosen PP: Rosen’s breast pathology. 3rd
Edition. Lippincott Williams & Wilkins (Wolters Kluwer);
Philadelphia: 2009
|
|
8
|
Rosen PP and Caicco JA: Florid
papillomatosis of the nipple. A study of 51 patients, including
nine with mammary carcinoma. Am J Surg Pathol. 10:87–101.
1986.PubMed/NCBI
|
|
9
|
Yang GZ, Li J and Ding HY: Nipple adenoma:
report of 18 cases with review of literatures. Zhonghua Bing Li Xue
Za Zhi. 38:614–616. 2009.(In Chinese).
|
|
10
|
Interlandi A and Busacca G: Adenomas of
the nipple. Minerva Chir. 57:699–702. 2002.(In Italian).
|
|
11
|
Tavassoli FA and Devilee P: World Health
Organization Classification of Tumors. Pathology and Genetics of
Tumours of the Breast and Female Genital Organs. IARC Press; Lyon:
2003
|
|
12
|
Brownstein MH, Phelps RG and Magnin PH:
Papillary adenoma of the nipple: analysis of fifteen new cases. J
Am Acad Dermatol. 12:707–715. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Batistatou A, Stefanou D, Arkoumani E and
Agnantis NJ: The usefulness of p63 as a marker of breast
myoepithelial cells. In Vivo. 17:573–576. 2003.PubMed/NCBI
|
|
14
|
Dewar R, Fadare O, Gilmore H and Gown AM:
Best practices in diagnostic immunohistochemistry: myoepithelial
markers in breast pathology. Arch Pathol Lab Med. 135:422–429.
2011.PubMed/NCBI
|
|
15
|
Werling RW, Hwang H, Yaziji H and Gown AM:
Immunohistochemical distinction of invasive from non-invasive
breast lesions: a comparative study of p63 versus calponin and
smooth muscle myosin heavy chain. Am J Surg Pathol. 27:82–90. 2003.
View Article : Google Scholar
|
|
16
|
Bergdahl L, Bergman F, Rais O and Westling
P: Bilateral adenoma of nipple. Report of a case. Acta Chir Scand.
137:583–586. 1971.PubMed/NCBI
|
|
17
|
Citoler P, Broer KH and Zippel HH:
Bilateral adenoma of nipple. Geburtshilfe Frauenheilkd. 33:729–731.
1973.(In German).
|
|
18
|
Rao P and Shousha S: Male nipple adenoma
with DCIS followed 9 years later by invasive carcinoma. Breast J.
16:317–318. 2010.PubMed/NCBI
|
|
19
|
Jones MW and Tavassoli FA: Coexistence of
nipple duct adenoma and breast carcinoma: a clinicopathologic study
of five cases and review of the literature. Mod Pathol. 8:633–636.
1995.PubMed/NCBI
|
|
20
|
Hansen U and Rank F: Adenoma of the nipple
and concomitant breast cancer. Ugeskr Laeger. 147:1852–1853.
1985.(In Danish).
|
|
21
|
Bhagavan BS, Patchefsky A and Koss LG:
Florid subareolar duct papillomatosis (nipple adenoma) and mammary
carcinoma: report of three cases. Hum Pathol. 4:289–295. 1973.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ermilova VD and Seredin VP: Adenoma of the
nipple with malignant degeneration. Arkh Patol. 49:59–61. 1987.(In
Russian).
|
|
23
|
Gudjónsdóttir A, Hägerstrand I and Ostberg
G: Adenoma of the nipple with carcinomatous development. Acta
Pathol Microbiol Scand A. 79:676–680. 1971.PubMed/NCBI
|