Introduction
Lung cancer is the leading cause of
cancer-associated mortality worldwide, and non-small cell lung
cancer (NSCLC) accounts for >80% of all cases. In total, <20%
of NSCLC patients are effectively cured of the disease due to the
lack of effective early diagnostic methods, the high frequency of
recurrence following curative surgery and the fact that >70% of
patients are in the advanced stages of the disease at the time of
diagnosis (1–3).
The presence of circulating free DNA in the plasma
of patients with malignant neoplasms has been a well-established
concept for >30 years. Studies have been undertaken to analyze
the plasma circulating free DNA concentrations, together with the
genetic and epigenetic alterations of the tumor DNA of patients who
suffer from numerous types of cancer, including colon, breast,
prostate and germ cell tumors (4–6). It
has been previously demonstrated that patients suffering from
malignant diseases have increased amounts of cell-free nucleic
acids in their circulation; this circulating cell-free DNA is
elevated in cancer patients and decreases in response to effective
treatment (3,4,7).
As tumor tissues contain high copy numbers of
mitochondrial DNA (mtDNA), the detection of plasma mtDNA may act as
a sensitive tool for the identification of changes in disease
status during cancer treatment. The present study investigated
whether plasma mtDNA concentrations in lung cancer patients with
adenocarcinoma were altered during treatment with erlotinib, an
epidermal growth factor receptor-tyrosine kinase inhibitor
(EGFR-TKI), and whether this change has the potential to be used as
a predictor of treatment response.
Materials and methods
Patients
The present study procedure was approved by the
Taipei Veterans General Hospital Institutional Review Board (VGHIRB
no. 98–11–05). Patients with adenocarcinoma of the lung who were to
receive erlotinib treatment were enrolled in the study once
informed consent had been obtained. Blood samples were collected
immediately prior to the administration of the first dose of
erlotinib, on days 15 and 29 following the initiation of erlotinib
treatment and also when the disease had progressed.
Quantification of plasma free circulating
mtDNA
Plasma was collected in EDTA tubes and centrifuged
at 405 × g for 5 min. Each plasma sample (20 μl) was mixed with 20
μl of a preparation buffer that contained 2.5% Tween-20, 50 mM Tris
and 1 mM EDTA. This mixture was digested with 16 μg proteinase K
(Qiagen, Valencia, CA, USA) at 50°C for 40 min and diluted with 160
μl Tris-EDTA buffer after 5 min of heat deactivation at 95°C.
Following centrifugation at 10,625 × g for 10 min, 1 μl of
supernatant containing 0.1 μl of an equivalent quantity of the
plasma was used as a template for quantitative PCR (qPCR) without
purification. The copy number of mtDNA was measured by qPCR
(TaqMan) performed on a LightCycler 1.2 using a LightCycler
FastStart DNA Master Plus HybProbe kit (Roche Diagnostics,
Mannheim, Germany). The primers and probe were obtained from
PreVision Medical Corporation (New Taipei City, Taiwan, China) and
selected to amplify 194-bp fragments in the mtDNA conserved region.
The primer sequence used was AATTTCGTGCCAGCCACCGC and the probe
sequence used was CTACGAAAGTGGCTTTAACA. Reactions were performed in
a total volume in 20 μl, consisting of 4 μl 5× Master Mix
(PreVision Medical Corporation), 0.8 μM probe and 0.4 μM of each
primer. Thermocycling was performed in 20-μl glass capillary tubes.
Following a 10 min activation step at 95°C, the reactions were
subjected to 45 cycles of 95° for 15 sec, 60°C for 30 sec and 72°C
for 5 sec. The absolute equivalent amount of the mtDNA copy number
in each sample was determined by a standard curve with serial
dilutions of the cloned plasmid.
EGFR mutation analysis
EGFR mutation analysis was performed
utilizing nucleotide sequence analysis. The VarientSEQr™
Resequencing Primer Set (Applied Biosystems, Foster City, CA, USA)
was selected for mutational analysis of the tyrosine kinase domain,
located at exons 18–21 of the EGFR gene. Genomic DNA was
extracted from paraffin blocks, exons 18–21 were amplified and
uncloned PCR fragments were sequenced and analyzed in the sense and
antisense directions for the presence of heterozygous mutations.
All the sequence variations were confirmed by multiple, independent
PCR amplifications and repeated sequencing reactions. EGFR
activating mutations were defined as those with exon 19 deletions
or exon 21 L858R.
Efficacy evaluation
A chest computed tomography scan (including the
liver and adrenal glands) was performed within three weeks prior to
the initiation of erlotinib treatment, at one and three months
following the initiation of erlotinib treatment and then every
three months thereafter. Treatment response evaluation was
performed according to the Response Evaluation Criteria in Solid
Tumors (RECIST) group criteria version 1.1 (8). Progression-free survival (PFS) was
calculated from the date of starting erlotinib treatment to the
earliest sign of disease progression, as determined by means of the
RECIST criteria, or mortality from any cause. If disease
progression had not occurred at the time of the last follow-up
visit, PFS was considered to have been censored at that time.
Statistical analysis
Survival curves were drawn using the Kaplan-Meier
method. The log-rank test was used for comparisons of data. The
plasma mtDNA levels in the patients who received erlotinib
treatment were compared using the independent samples t-test,
non-parametric Mann-Whitney test and the Wilcoxon test for
different conditions. P<0.05 was considered to indicate a
statistically significant difference. All statistical analyses were
performed using SPSS software (SPSS, Inc., Chicago, IL, USA).
Results
Patient characteristics and treatment
response
Plasma was prospectively collected from 53 patients,
including 20 males and 33 females, with a mean age of 64 years and
a range of 30–88 years. The performance status was 0 in four
patients, 1 in 36 patients, 2 in nine patients and 3 in four
patients. Of these 53 patients, the most common response to
erlotinib treatment was a partial response (PR) in 26 patients
(49.1%), followed by stable disease (SD) in 13 patients (24.5%) and
progressive disease (PD) in 14 patients (26.4%). Of the 30 patients
who had tumor tissue samples available for EGFR mutation
analysis, 16 patients had EGFR activating mutations and 14
patients were EGFR wild-type.
Plasma mtDNA concentration correlates
with erlotinib treatment response
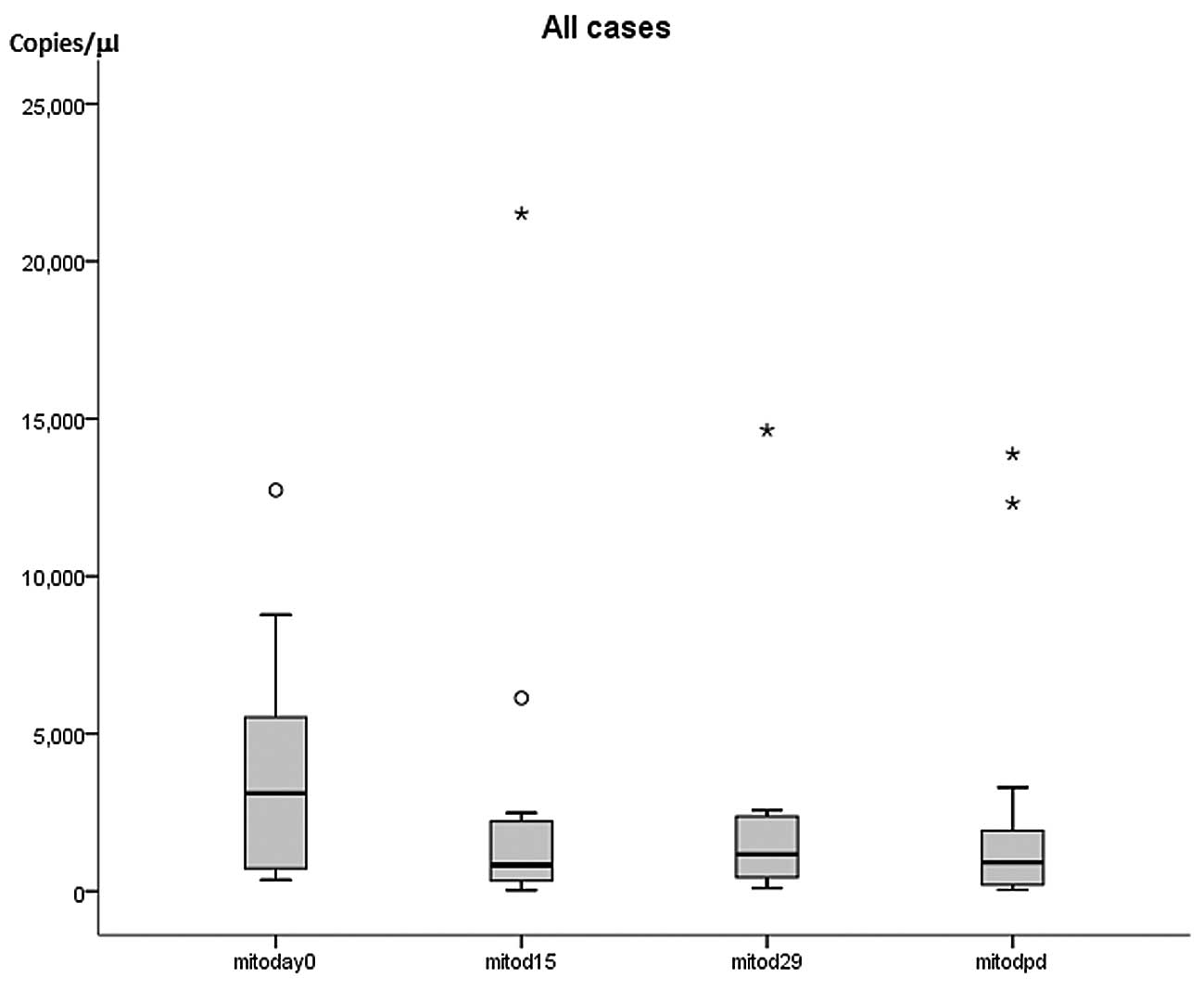
In the patients with a PR to erlotinib treatment,
the mean plasma mtDNA concentration was 2,907±757 copies/μl (mean ±
standard error of the mean) on day 0 (n=26), 3,109±986 copies/μl on
day 15 (n=23), 2,077±473 copies/μl on day 29 (n=24) and 808±446
copies/μl with disease progression (n=7). In the patients with PD
following erlotinib treatment, the mean plasma mtDNA concentration
was 3,776±1,014 copies/μl on day 0 (n=14), 1,567±387 copies/μl on
day 15 (n=13), 3,159±1,667 copies/μl on day 29 (n=8) and
6,387±2,189 copies/μl with disease progression (n=9) (Table I; Fig.
1).
 | Table IPlasma free mtDNA levels in 53
erlotinib-treated patients. |
Table I
Plasma free mtDNA levels in 53
erlotinib-treated patients.
| Parameter | Partial response | Stable disease | Progressive
disease |
|---|
| Day 0 |
| No. of patients | 26 | 13 | 14 |
| mtDNA concentration,
copies/μl |
| Mean ± SEM | 2907±757 | 2601±874 | 3776±1,013 |
| Range | 154–17,510 | 228–10,644 | 63–12,733 |
| Day 15 |
| No. of patients | 23 | 11 | 13 |
| mtDNA concentration,
copies/μl |
| Mean ± SEM | 3109±986 | 774±221 | 1568±387 |
| Range | 26–21,511 | 60–2,395 | 54–4,925 |
| Day 29 |
| No. of patients | 24 | 11 | 8 |
| mtDNA concentration,
copies/μl |
| Mean ± SEM | 2077±473 | 2935±948 | 3159±1,667 |
| Range | 56–7,587 | 107–9,383 | 390–14,637 |
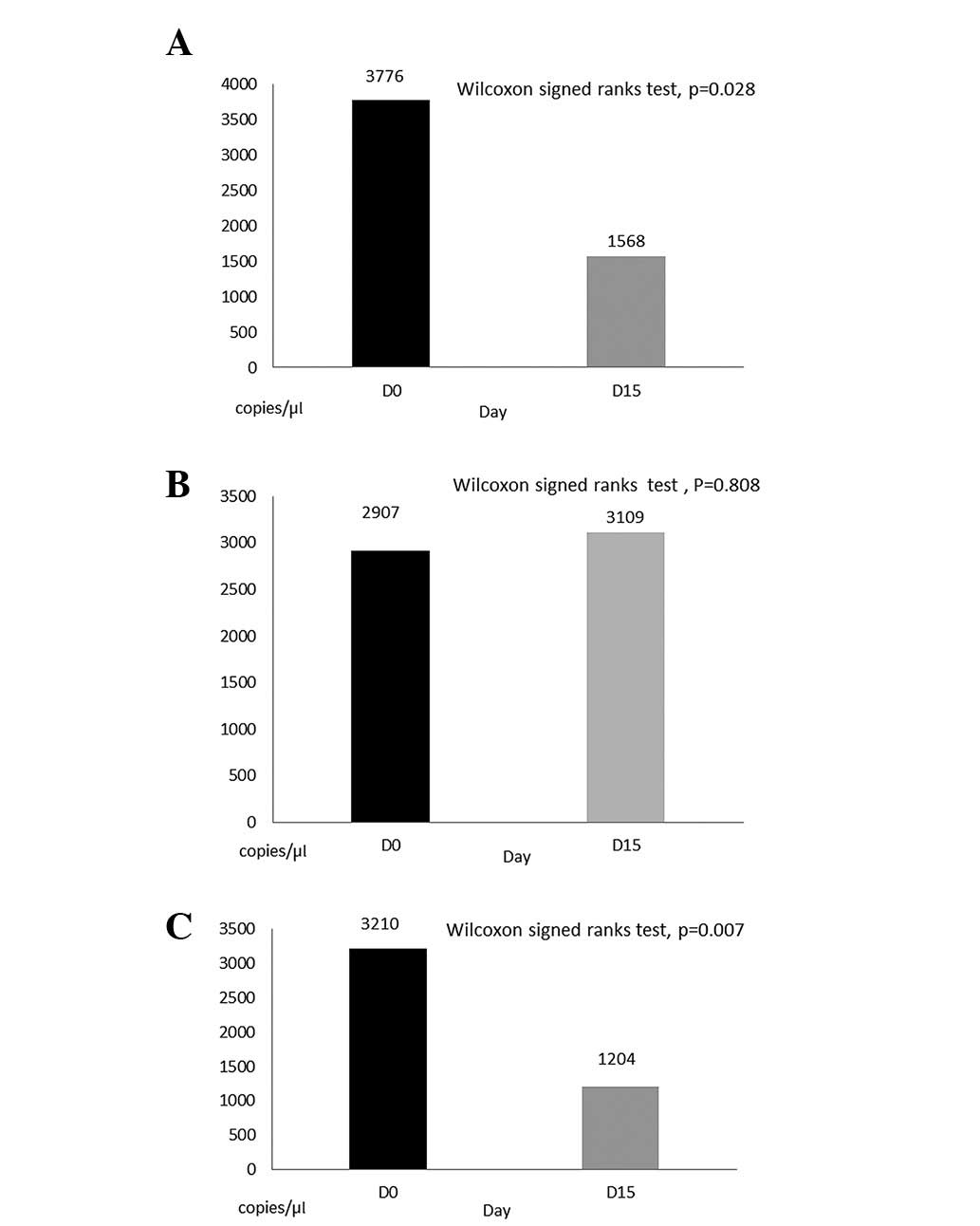
Sequential changes in plasma mtDNA concentration in
individual patients were significantly decreased on day 15 compared
with the levels observed on day 0 in the patients with PD following
erlotinib treatment (Wilcoxon signed-rank test, P=0.028; Fig. 2A) or with no response (SD + PD) to
erlotinib treatment (Wilcoxon signed-rank test, P=0.007; Fig. 2B). Plasma mtDNA concentrations in
patients with a PR to erlotinib treatment did not differ
significantly on day 15 compared with day 0 (Wilcoxon signed-rank
test, P=0.808; Fig. 2C), as the
levels of individual patients varied, with decreases, increases or
similar concentrations recorded. There was no statistically
significant difference in plasma mtDNA concentrations between days
0 and 29 or the day of disease progression in individual patients
with a response, SD, PD or no response to treatment. When the
patients were divided into a PR group and a non-PR group, the PR
group had significantly higher plasma mtDNA concentrations than the
non-PR group on day 15 and when the disease progressed (independent
samples t-test, P=0.004 and P=0.003, respectively). Although the
patients with low plasma mtDNA levels had a marginally longer PFS,
there was no statistically significant difference in PFS between
the patients with high or low plasma mtDNA concentrations (P=0.367,
Fig. 3). There was no significant
correlation of the plasma mtDNA levels with tumor EGFR
wild-type or activating mutations (P=0.951).
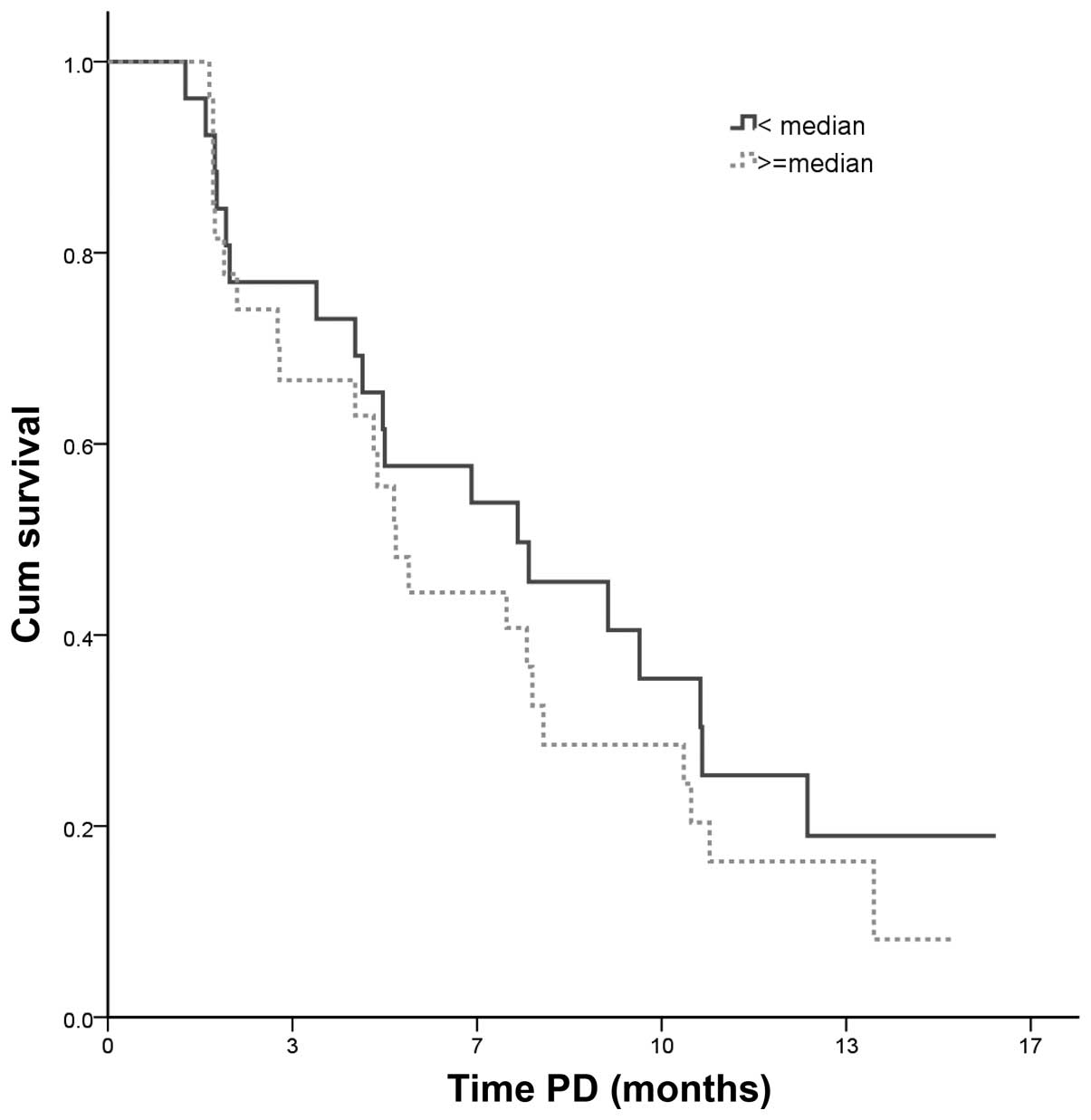 | Figure 3PFS following the initiation of
erlotinib treatment. Patients with a plasma free mitochondrial DNA
concentration lower than median value had a longer PFS time
compared with patients with plasma free mtDNA concentration that
was higher than the median value, however, this difference was not
statistically significant (low free mtDNA value: n=26, censor 7,
median 7.4 months; high free mtDNA value: n=27, censor 4, median
5.2 months; P=0.367). PFS, progression-free survival; mtDNA,
mitochondrial DNA; PD, progressive disease; Cum, cumulative. |
Discussion
A number of serum or plasma markers, including
cytokeratin fragment 21–1, carcinoembryonic antigen, carbohydrate
antigen 19–9 and squamous cell carcinoma antigen, have been
considered as potential aids in the screening or early detection of
lung cancer. The levels of these circulating markers have been
reported to be elevated in certain lung cancer patients (9–11).
However, not all cancer patients had elevated markers.
Circulating free DNA has been found in healthy
individuals, patients with non-malignant diseases and in those with
various malignancies, including lung cancer (2,3,12–19).
However, several studies have revealed that these circulating free
DNA concentrations are notably higher in individuals with various
malignancies than in healthy controls (2,16,20).
As a result, numerous mechanisms have been hypothesized to explain
the release of circulating free DNA into the circulation by
tumor-host or tumor-virus interactions (16,17).
The detection of plasma circulating tumor DNA in
lung cancer patients may be a potential marker for screening,
diagnosis, prognosis, monitoring of treatment response and the
early detection of disease progression. The best examples are
circulating EGFR mutation markers, which may be used to
gauge response, monitor progression and possibly detect newly
acquired mutations (21,22). Circulating mtDNA is a type of
circulating free DNA, the study of which has been limited in
comparison. The present study attempted to identify whether this
circulating marker may be used as a predictor in EGFR-TKI treatment
for patients with pulmonary adenocarcinoma.
The detection of specific mitochondrial mutations in
a patient’s plasma would be a useful measurement to investigate
novel diagnostic tools for lung cancer. However, the specific
mitochondrial mutations that occur in lung cancer have rarely been
studied, nor have they been reported in plasma samples, although
mutations in the mitochondrial genome have been documented for a
number of other types of cancer (23,24).
Despite this, the detection of free mtDNA in plasma is as simple to
perform as the detection of plasma free DNA in cancer patients.
In previous studies, lung cancer patients who had
received chemotherapy were reported to have significantly increased
plasma free DNA concentrations at the time of disease progression
(20,25,26).
In the present study, patients with a response to erlotinib
treatment had significantly higher plasma mtDNA concentrations than
the remaining patients (the no response group) on day 15 following
erlotinib treatment and when their disease progressed (P=0.004 and
P=0.003, respectively). The initial elevation of mtDNA on day 15
could be explained by the erlotinib-induced destruction of tumor
cells, which may have been accompanied by the release of mtDNA into
the circulation. Elevation of mtDNA in patients who progressed
following an initial response may be due to the increased
proliferation and turnover of these tumor cells. By contrast, mtDNA
levels were lower on day 15 in those patients resistant to
erlotinib treatment. This may be due to the lack of a tumoricidal
effect of erlotinib treatment on these tumor cells, or more likely
due to a reduced tumor cell turnover rate in the first two weeks of
erlotinib treatment in these patients.
The present study demonstrated that plasma mtDNA
levels did not correlate with PFS when pulmonary adenocarcinoma
patients received erlotinib treatment, and that there was also no
association with tumor EGFR mutation status. To the best of
our knowledge, these findings have not been reported in any
previous studies. According to these results, plasma mtDNA appeared
to be of weak clinical utility as a screening, diagnostic or
prognostic tool in lung cancer patients.
Acknowledgements
This study was supported by grants from the National
Science Council of the Republic of China (grant number,
NSC99–2314-B-075-035-MY3) and Taipei Veterans General Hospital
(grant number, VGH-100-C-015).
References
|
1
|
Wu CH, Fan WC, Chen YM, Chou KT, Shih JF,
Tsai CM, et al: Second-line therapy for elderly patients with
non-small cell lung cancer who failed previous chemotherapy is as
effective as for younger patients. J Thorac Oncol. 5:376–379. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Paci M, Maramotti S, Bellesia E, Formisano
D, Albertazzi L, Ricchetti T, et al: Circulating plasma DNA as
diagnostic biomarker in non-small cell lung cancer. Lung Cancer.
64:92–97. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pathak AK, Bhutani M, Kumar S, Mohan A and
Guleria R: Circulating cell-free DNA in plasma/serum of lung cancer
patients as a potential screening and prognostic tool. Clin Chem.
52:1833–1842. 2006.PubMed/NCBI
|
|
4
|
Cheng C, Omura-Minamisawa M, Kang Y, Hara
T, Koike I and Inoue T: Quantification of circulating cell-free DNA
in the plasma of cancer patients during radiation therapy. Cancer
Sci. 100:303–309. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mancini M, Anderson BO, Caldwell E,
Sedghinasab M, Paty PB and Hockenbery DM: Mitochondrial
proliferation and paradoxical membrane depolarization during
terminal differentiation and apoptosis in a human colon carcinoma
cell line. J Cell Biol. 138:449–469. 1997. View Article : Google Scholar
|
|
6
|
Ellinger J, Müller SC, Wernert N, von
Ruecker A and Bastian PJ: Mitochondrial DNA in serum of patients
with prostate cancer: a predictor of biochemical recurrence after
prostatectomy. BJU Int. 102:628–632. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang R, Shao F, Wu X and Ying K: Value of
quantitative analysis of circulating cell free DNA as a screening
tool for lung cancer: A meta-analysis. Lung Cancer. 69:225–231.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Eisenhauer EA, Therasse P, Bogaerts J, et
al: New response evaluation criteria in solid tumours: revised
RECIST guideline (version 1.1). Eur J Cancer. 45:228–247. 2009.
View Article : Google Scholar
|
|
9
|
Vassilakopoulos T, Troupis T, Sotiropoulou
C, Zacharatos P, Katsaounou P, Parthenis D, et al: Diagnostic and
prognostic significance of squamous cell carcinoma antigen in
non-small cell lung cancer. Lung Cancer. 32:137–144. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Suemitsu R, Yoshino I, Tomiyasu M,
Fukuyama S, Okamoto T and Maehara Y: Serum tissue inhibitors of
metalloproteinase-1 and -2 in patients with non-small cell lung
cancer. Surg Today. 34:896–901. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kulpa J, Wójcik E, Reinfuss M and
Kolodziejski L: Carcinoembryonic antigen, squamous cell carcinoma
antigen, CYFRA 21–1, and neuron-specific enolase in squamous cell
lung cancer patients. Clin Chem. 48:1931–1937. 2002.
|
|
12
|
Sozzi G, Conte D, Mariani L, et al:
Analysis of circulating DNA in plasma at diagnosis and during
follow-up of lung cancer patients. Cancer Res. 61:4675–4678.
2001.PubMed/NCBI
|
|
13
|
Sozzi G, Conte D, Leon M, et al:
Quantification of free circulating DNA as a diagnostic marker in
lung cancer. J Clin Oncol. 21:3902–3908. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gai S, Fidler C, Lo YM, et al:
Quantitation of circulating DNA in the serum of breast cancer
patients by real-time PCR. Br J Cancer. 90:1211–1215. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Flamini E, Mercatali L, Nanni O, et al:
Free DNA and carcinoembryonic antigen serum levels: an important
combination for diagnosis of colorectal cancer. Clin Cancer Res.
12:6985–6988. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ziegler A, Zangemeister-Wittke U and
Stahel RA: Circulating DNA a new diagnostic gold mine? Cancer Treat
Rev. 28:255–271. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gormally E, Caboux E, Vineis P and Hainaut
P: Circulating free DNA in plasma or serum as biomarker of
carcinogenesis: practical aspects and biological significance.
Mutat Res. 635:105–117. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Laktionov PP, Tamkovich SN, Rykova EY,
Bryzgunova OE, Starikov AV, Kuznetsova NP, et al: Extracellular
circulating nucleic acids in human plasma in health and disease.
Nucleosides Nucleotides Nucleic Acids. 23:879–883. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Antonatos D, Patsilinakos S, Spanodimos S,
Korkonikitas P and Tsigas D: Cell-free DNA levels as a prognostic
marker in acute myocardial infarction. Ann NY Acad Sci.
1075:278–281. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pathak AK, Bhutani M, Kumar S, Mohan A and
Guleria R: Circulating free DNA in plasma/serum of lung cancer
patients as a potential screening and prognostic tool. Clin Chem.
52:1833–1842. 2006.PubMed/NCBI
|
|
21
|
Rosell R, Carcereny E, Gervais R, et al:
Erlotinib versus standard chemotherapy as first-line treatment for
European patients with advanced EGFR mutation positive
non-small-cell lung cancer (EURTAC): a multicentre, open-label,
randomised phase 3 trial. Lancet Oncol. 13:239–246. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Punnoose EA, Atwal S, Liu W, et al:
Evaluation of circulating tumor cells and circulating tumor DNA in
non-small cell lung cancer: association with clinical endpoints in
a phase II clinical trial of pertuzumab and erlotinib. Clin Cancer
Res. 18:2391–2401. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Penta JS, Johnson FM, Wachsman JT and
Copeland WC: Mitochondrial DNA in human malignancy. Mutat Res.
488:119–133. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Jerónimo C, Nomoto S, Caballero OL, Usadel
H, Henrique R, Varzim G, et al: Mitochondrial mutations in early
stage prostate cancer and bodily fluids. Oncogene. 20:5195–5198.
2001.PubMed/NCBI
|
|
25
|
Leon SA, Shapiro B, Sklaroff DM and Yaros
MJ: Free DNA in the serum of cancer patients and the effect of
therapy. Cancer Res. 37:646–650. 1977.PubMed/NCBI
|
|
26
|
Kumar S, Guleria R, Singh V, et al: Plasma
DNA level in predicting therapeutic efficacy in advanced nonsmall
cell lung cancer. Eur Respir J. 36:885–892. 2010. View Article : Google Scholar : PubMed/NCBI
|