Introduction
Primary central nervous system lymphoma (PCNSL) is a
rare disease, accounting for 6% of all intracranial tumors and 1–2%
of all lymphomas (1,2). Unlike other brain tumors, PCNSL does
not warrant radical surgery as the lesions are highly infiltrative
(3). PCNSL is a chemosensitive and
radiosensitive tumor, thus a stereotaxic biopsy is frequently
performed. Early and accurate diagnosis of PCNSL is essential for
treatment and prognosis (4).
The temporal disappearance of PCNSL as a result of
steroid therapy is well known. Histologically, destructive and
demyelinating pseudotumoral characteristics, termed sentinel
lesions, are observed following steroid therapy for PCNSL (5). It is difficult to distinguish the
sentinel lesions of PCNSL from demyelinating diseases following
steroid therapy (5) and few studies
have reported the spontaneous radiographic and histological
remission of PCNSL (5–8). The current study presents a rare case
of PCNSL with preceding pseudotumoral demyelination in an
immunocompetent adult that had not received any previous steroid
treatment; the pitfalls of PCNSL diagnosis are also discussed. The
study was conducted under the auspices of the University of
Occupational and Environmental Health Institutional Review Board
(IRB; Kitakyushu, Japan) who provided approval for the use of human
tissues. The IRB waived the requirement for obtaining informed
consent.
Case report
A 70-year-old male with no previous medical concerns
experienced memory and gait disturbances and consulted to the
University Hospital of Occupational Environmental Health
(Kitakyushu, Japan). Neurological examination revealed mild right
hemiparesis and dysarthria. The patient’s mini-mental state
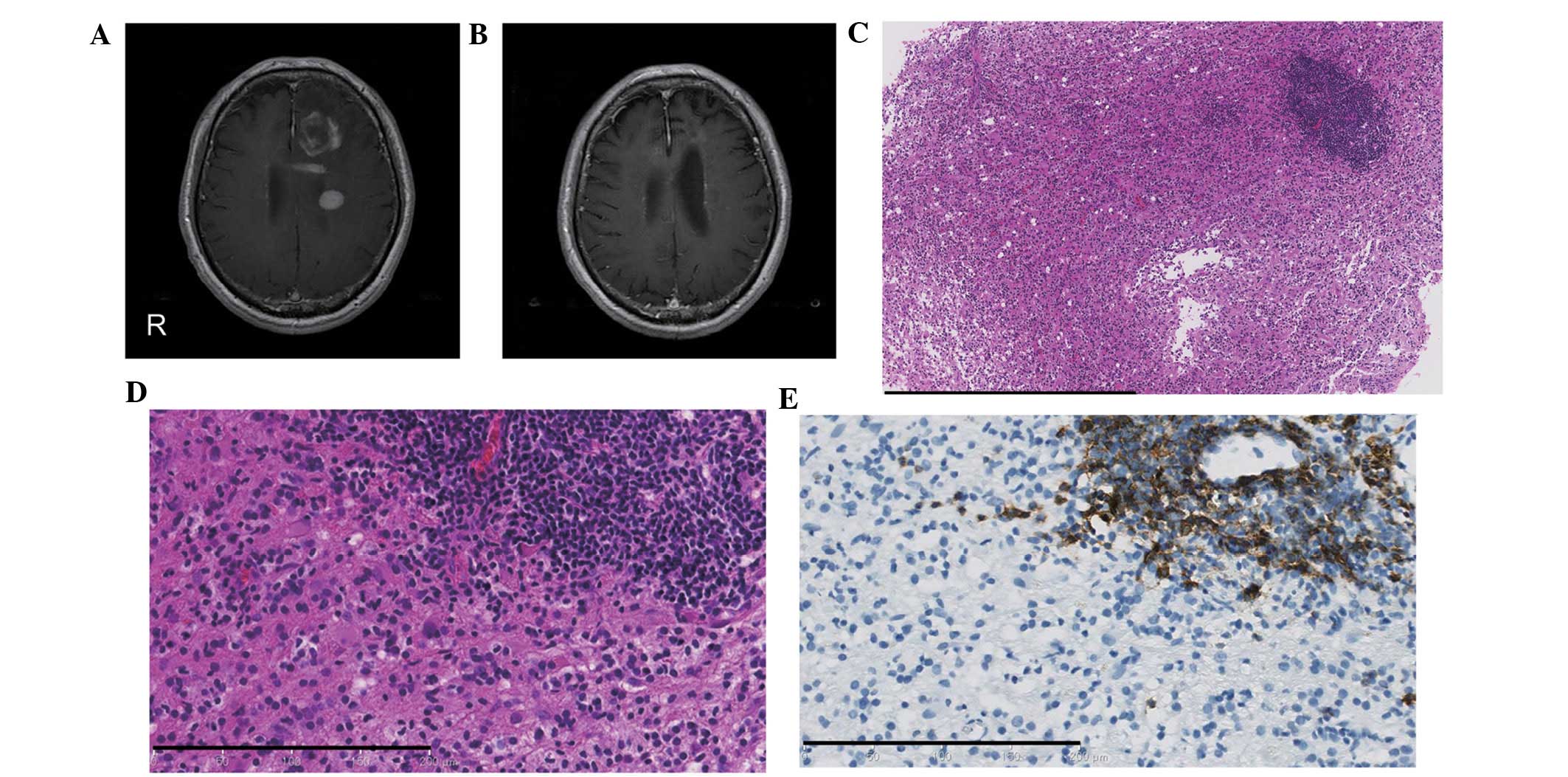
examination (MMSE) score was 7/30. Magnetic resonance imaging (MRI)
showed multiple enhanced lesions with perifocal brain edema in the
left cerebral hemisphere (Fig. 1A).
Whole-spine MRI, whole-body computed tomography and gascintigraphy
showed no abnormalities. In addition, no other abnormal
hyperintensity or suspected chronic lesions were detected on MRI.
Blood examination, including assessments for determining the levels
of soluble interleukin-2 receptor (IL-2R; 388 U/ml) and
anti-aquaporin-4, indicated no abnormalities. The serological
examination for infectious and collagen diseases was unremarkable.
Cerebrospinal fluid (CSF) examination yielded normal results; the
CSF showed normal oligoclonal immunoglobulin G bands (OCB) and no
myelin basic protein, IL-2R or malignant cells. The patient
underwent stereotaxic biopsy after one week. Histological
examination of the brain biopsy sample from the left frontal lobe
lesion showed myelin destruction with relative sparing of axons,
several T lymphocytes and foamy macrophages (Fig. 1C and D). Perivascular aggregation of
B-cells was only observed in a small area (Fig. 1E). The patient had no previous
symptoms, no chronic lesions on MRI and negative OCB; thus, the
condition was diagnosed as multiple sclerosis. The patient
gradually improved with pulse corticosteroid therapy. Multiple
brain lesions were absent from the MRI scans obtained two months
following the biopsy (Fig. 1B) and
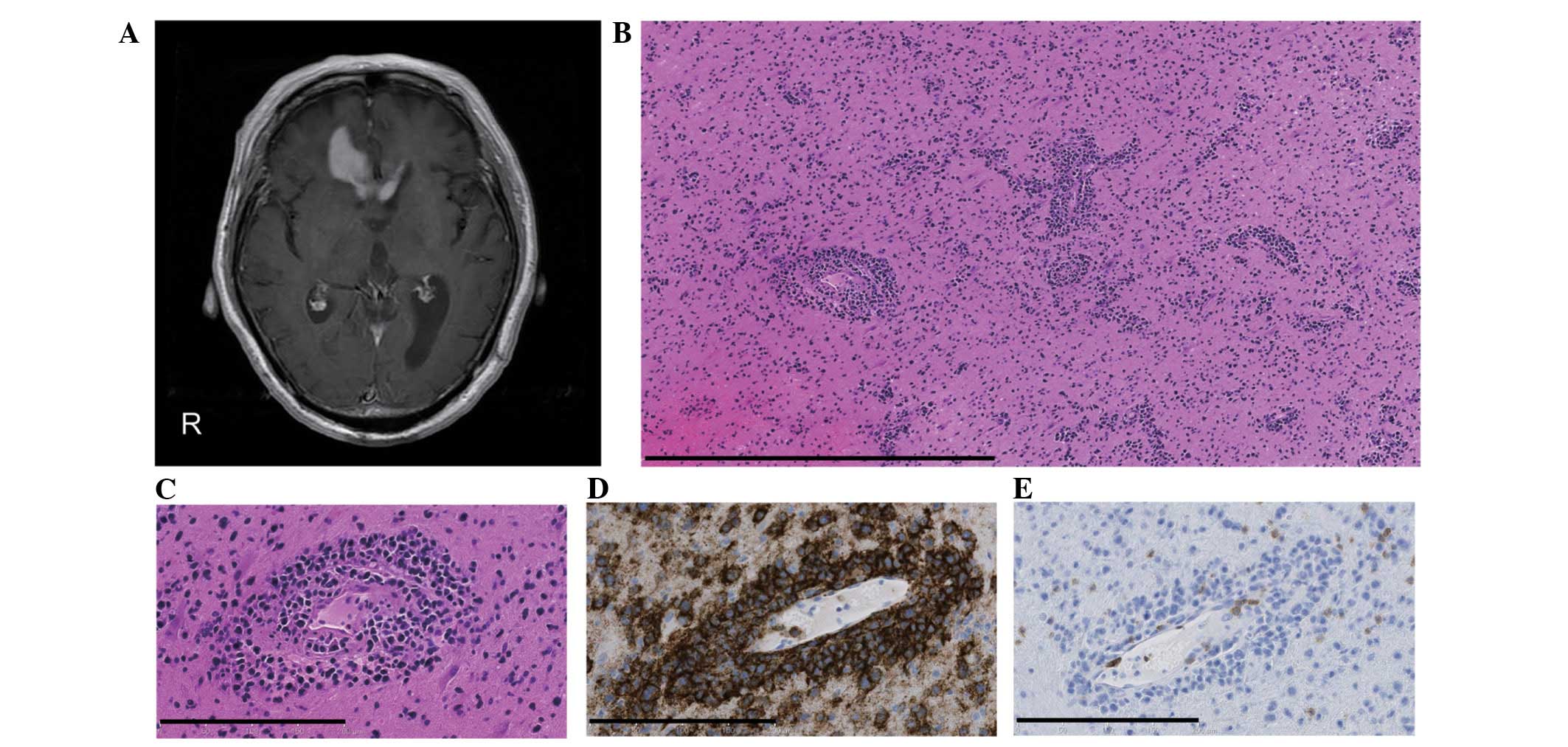
the MMSE score had increased to 17/30. However, three months after
the biopsy, the patient’s condition deteriorated again. MRI
revealed a homogeneous enhanced lesion in the right frontal lobe
with severe perifocal brain edema (Fig.
2A). Blood examination showed an elevated level of IL-2R (911.0
U/ml). The patient received a brain biopsy with craniotomy.
Histological examination of the biopsied lesion revealed diffuse
infiltrating B-cells with perivascular aggregation (Fig. 2B–E); therefore the condition was
diagnosed as diffuse large B-cell type PCNSL. Following whole brain
radiation therapy (45 Gy) and steroid therapy the patient initially
showed minimal regression, however, a slow progressive
deterioration in neurological and general function subsequently
developed. The patient succumbed eight months after the initial
diagnosis.
Discussion
This study presents an unusual case of PCNSL with
preceding demyelinating pseudotumoral characteristics in a patient
that had not received any previous steroid treatment. Initially,
the demyelinating lesions disappeared following steroid therapy and
the patient recovered. However, three months after the primary
pathological diagnosis, the lesions recurred and were diagnosed as
typical PCNSL.
To the best of our knowledge, only six cases of
PCNSL with preceding demyelinating pseudotumoral changes and no
previous steroid treatment have been published in the literature to
date (Table I). The pathogenesis of
spontaneous demyelinating changes in PCNSL remains unclear. PCNSL
usually develops in the fifth and sixth decades of life, and the
male to female ratio for PCNSL is 2:5. A previous study reported
that non-Hodgkin’s lymphoma deteriorated during the postpartum
period (9). Sudden hormonal changes
during pregnancy and menopause may alter the immune system and
induce spontaneous regression of PCNSL. Another study reported the
case of a male patient with PCNSL who previously had seroconversion
of hepatitis B (Tables I and
II, case 2); treatment for
hepatitis B may have had affected the immunomodulating reaction to
PCNSL. However, there was no previous disease in the present
case.
 | Table ISummary of central nervous system
lymphoma immunocompetent patients from the literature and the
present study without pretreatment of steroids, chemotherapy or
radiotherapy. |
Table I
Summary of central nervous system
lymphoma immunocompetent patients from the literature and the
present study without pretreatment of steroids, chemotherapy or
radiotherapy.
| Case no. | First author
(year) | Age
(years)/gender | Primary symptoms | Diagnostic
modality | Primary site | Primary pathological
diagnosis (method) |
|---|
| 1 | Takekawa H
(2008) | 68/F | Hypertension | MRI | Bilateral occipital
lobe | None (biopsy) |
| 2 | Suzuki M (2009) | 57/M | General seizure | MRI FDG-PET | Left frontal
lobe | Ganglioglioma
(biopsy) |
| 3 | Alderson L
(1996) | 49/F | Ataxia, vertigo | CT, MRI | Pons extending to the
fourth ventricle | Inflammation
(biopsy) |
| 4 | Weingarten KL
(1983) | 69/F | Gait disturbance
strange behavior | CT | Bifrontal
parasagittal cortical lesions | None |
| 5 | | 69/F | Altered mental
status | CT | Right cerebral
peduncle extended to caudate nucleus | None |
| 6 | | 60/F | Confusion,
obtundation seizure | CT | Left parietal
parasagittal cortex | None |
| 7 | Present case | 70/M | Strange behavior,
dementia, right hemiparesis | CT, MRI | Multiple lesions
predominantly in the left frontal lobe | Multiple sclerosis
(biopsy) |
| Table IITreatment of central nervous system
lymphoma following primary pathological diagnosis. |
Table II
Treatment of central nervous system
lymphoma following primary pathological diagnosis.
| Case no. | Treatment | Clinical course | Time before
progression | Secondary
pathological diagnosis (method) | Follow-up
prognosis |
|---|
| 1 | None | Remission of primary
lesion, but a later appearance of other multiple lesions | 4 months | DLBCL (biopsy) | No information |
| 2 | Steroid | Remission, but later
appearances of other multiple lesions | 24 months | DLBCL (biopsy) | No information |
| 3 | Steroid | Remission, but later
appearances of right frontal lesion | 11 months | DLBCL (biopsy) | No information |
| 4 | None | Remission of primary
lesions, but later the clinical condition progressively
deteriorated | No information | Poorly differentiated
malignant lymphoma (autopsy) | Succumbed 4 months
after initial presentation |
| 5 | None | Remission of primary
lesions, then a slow deterioration of the patient’s condition | No information | Malignant
undifferentiated lymphoma (autopsy) | Succumbed 3 months
after inital presentation |
| 6 | None | Remission of primary
lesions, patient was treated with steroids and radiotherapy
following biopsy | No progression | Malignant lymphoma
(autopsy) | Alive 4 years after
initial diagnosis |
| 7 | Steroid | Remission of primary
lesions, but later the clinical condition progressively
deteriorated | 3 months | DLBCL (biopsy) | Succumbed 8 months
after initial diagnosis |
Sentinel lesions with PCNSL is a rare occurrence and
the incidence rate is currently unknown; however, occurrence may be
more frequent than has previously been reported. Distinguishing
sentinel lesions with PCNSL from demyelinating diseases is
challenging, as demonstrated in the present case where there was no
previous medical history of corticosteroid therapy, no typical
clinical history (distribution of lesions in space and time) and no
other specific laboratory data, including MRI (10). Surgical specimens of lesions
obtained from stereotaxic biopsies may be inappropriate for an
accurate diagnosis. Furthermore, the biopsy target site affects the
pathological diagnosis.
In conclusion, the presence of sentinel lesions
indicates remission after corticosteroid treatment and is followed
by the diagnosis of typical PCNSL within the next three months to
two years. However, PCNSL and demyelinating diseases may respond
equally well to steroids (5,7). For a
biopsy specimen showing demyelinating lesions, clinicians are
required to conduct close clinical and radiological observations to
distinguish demyelinating diseases from sentinel lesions due to
PCNSL.
References
|
1
|
Watanabe M, Tanaka R, Takeda N,
Wakabayashi K and Takahashi H: Correlation of computed tomography
with the histopathology of primary malignant lymphoma of the brain.
Neuroradiology. 34:36–42. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Miller DC, Hochberg FH, Harris NL, et al:
Pathology with clinical correlations of primary central nervous
system non-Hodgkin’s lymphoma. The Massachusetts General Hospital
experience 1958–1989. Cancer. 74:1383–1397. 1994.PubMed/NCBI
|
|
3
|
Onda K, Wakabayashi K, Tanaka R and
Takahashi H: Intracranial malignant lymphomas: clinicopathological
study of 26 autopsy cases. Brain Tumor Pathol. 16:29–35. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dubuisson A, Kaschten B, Lenelle J, et al:
Primary central nervous system lymphoma report of 32 cases and
review of the literature. Clin Neurol Neurosurg. 107:55–63. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Alderson L, Fetell MR, Sisti M, et al:
Sentinel lesions of primary CNS lymphoma. J Neurol Neurosurg
Psychiatry. 60:102–105. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Takekawa H, Hozumi A, Hirata K and
Yamazaki K: A spontaneously vanishing primary cerebral lymphoma
‘ghost tumour’. J Neurol Neurosurg Psychiatry. 79:11592008.
|
|
7
|
Weingarten KL, Zimmerman RD and Leeds NE:
Spontaneous regression of intracerebral lymphoma. Radiology.
149:721–724. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Suzuki M, Uchiyama T, Takahashi H, et al:
A case report of primary central nervous system lymphoma preceded
by cerebral and cerebellar lesion diminishing spontaneously:
consideration of two brain biopsy at the onset and after two years.
Rinsho Shinkeigaku. 49:586–589. 2009.(In Japanese).
|
|
9
|
Ioachim HL: Non-Hodgkin’s lymphoma in
pregnancy. Three cases and review of the literature. Arch Pathol
Lab Med. 109:803–809. 1985.
|
|
10
|
Polman CH, Reingold SC, Banwell B, et al:
Diagnostic criteria for multiple sclerosis: 2010 revisions to the
McDonald criteria. Ann Neurol. 69:292–302. 2011. View Article : Google Scholar : PubMed/NCBI
|