Introduction
Pulmonary metastasis is a common occurrence in
patients with renal cancer and is usually treated with
immunotherapy and novel agents that target angiogenesis (1). Certain clinical studies have indicated
that the resection of pulmonary metastases (metastasectomy) may be
a treatment option (1–2). However, the role of surgery for
metastases originating from renal cancer has yet to be fully
determined. Pulmonary nodules that appear in patients who have
undergone nephrectomy for renal cancer are usually pulmonary
metastases. However, the occurrence of metachronous lung tumors and
certain benign diseases, particularly pulmonary hamartoma, are
uncommon (3). The patient provided
written informed consent.
Case report
A 55-year-old female was referred to the First
Affiliated Hospital, School of Medicine of Zhejiang University
(Hangzhou, China) due to the presence of multiple round pulmonary
nodules on a chest computed tomography (CT) scan, which was
performed during a postoperative follow-up evaluation for renal
cancer. The patient reported no history of cough, fever, chest
pain, dyspnea, hemoptysis, weight loss or tuberculosis. In
addition, no peripheral lymphadenopathy was detected and the
routine blood test results, including a hemogram and renal and
liver function tests, were within the normal ranges.
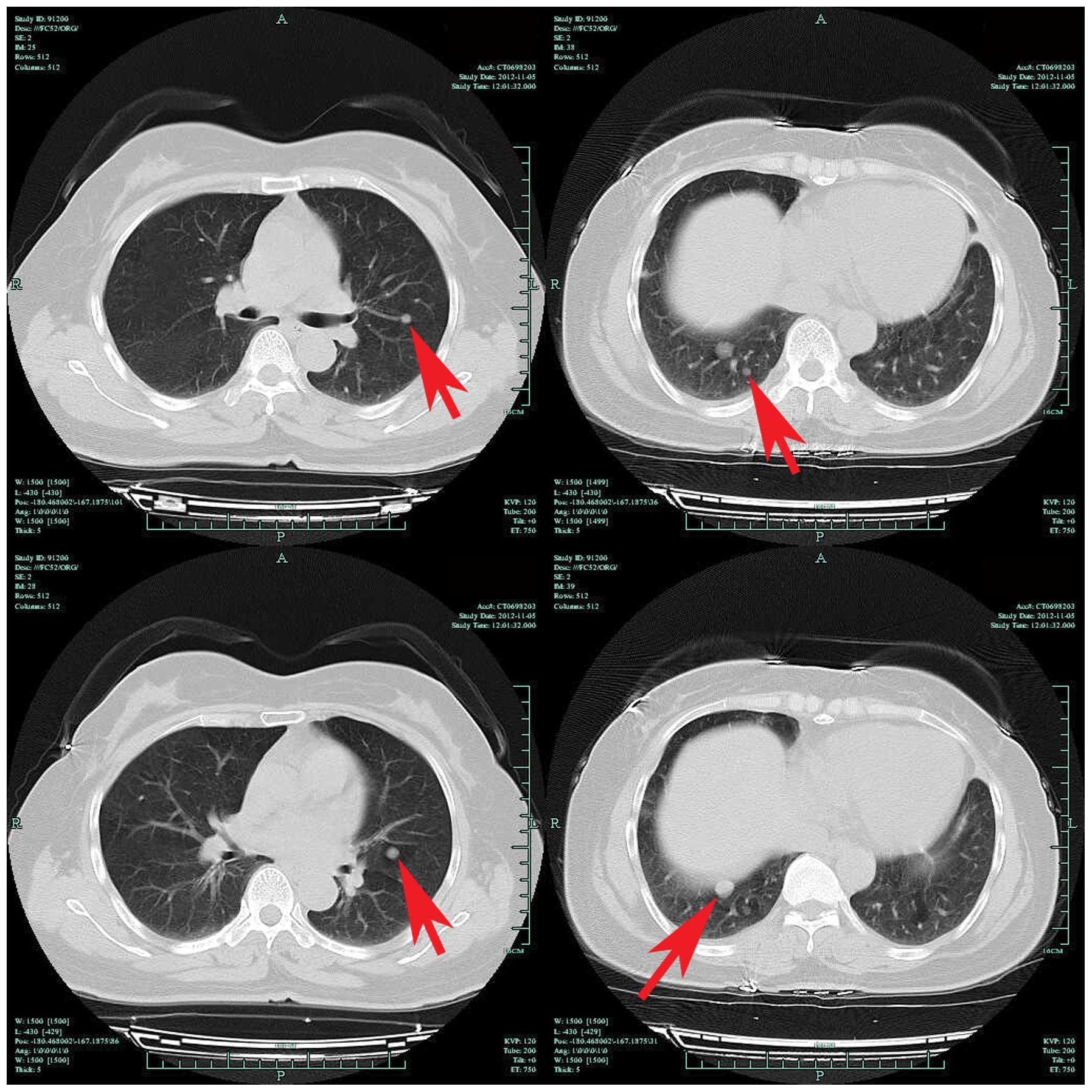
The patient underwent a contrast-enhanced CT of the
chest, which revealed multiple round pulmonary nodules measuring
~10×12 mm with clear boundaries in the lungs (Fig. 1). In addition, an
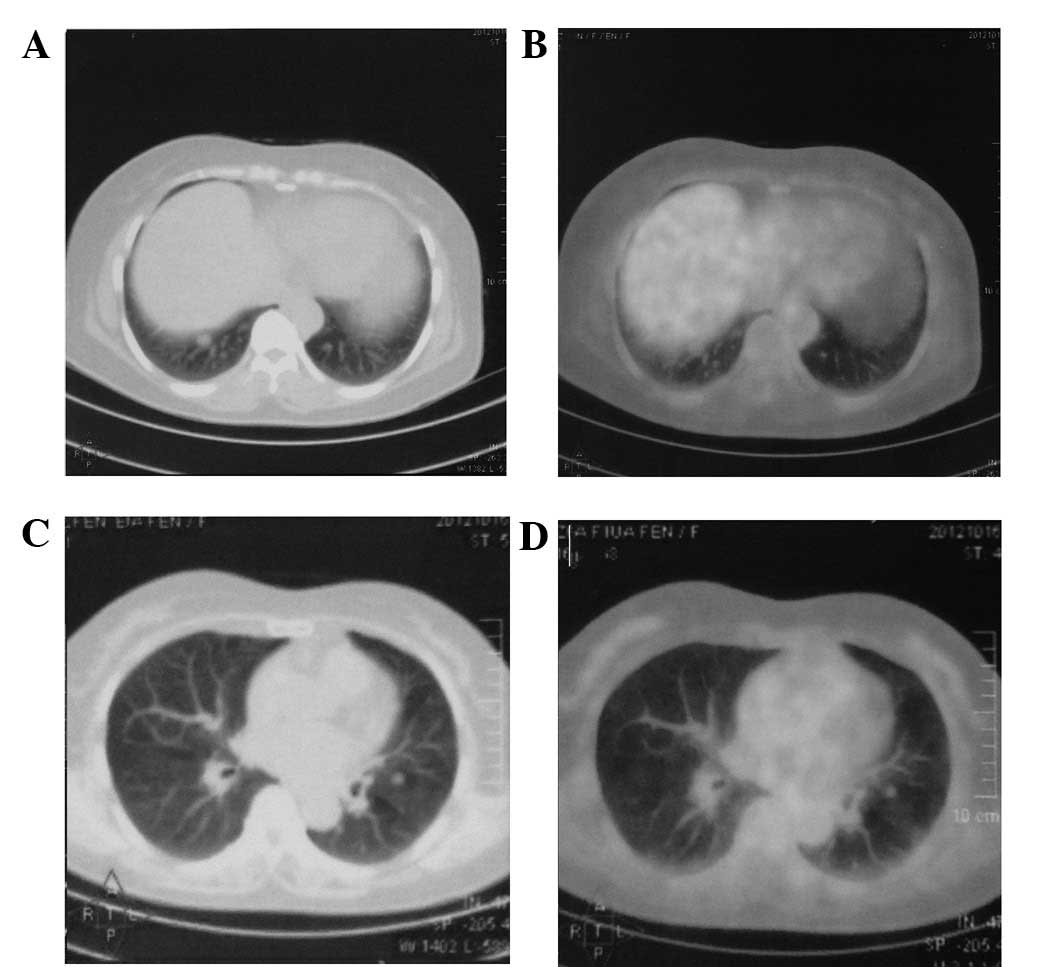
18F-fluoro-2-deoxy-D-glucose (FDG)-positron emission
tomography (PET)/CT scan was performed to characterize the nodules,
which exhibited a mild uptake of FDG that is indicative of
malignancy (Fig. 2). In addition,
bronchoscopy showed normal bronchi. Due to the presence of multiple
small nodules with clear boundaries in the lungs and the history of
a radical nephrectomy, a hypothetical diagnosis of pulmonary
metastasis of a previously removed renal carcinoma was determined
and subsequently confirmed by biopsy.
A video-assisted thoracoscopic nodulectomy was
performed on the patient and frozen-section analysis revealed that
the tumor was benign (possibly a pulmonary hamartoma) and the
procedure was terminated.
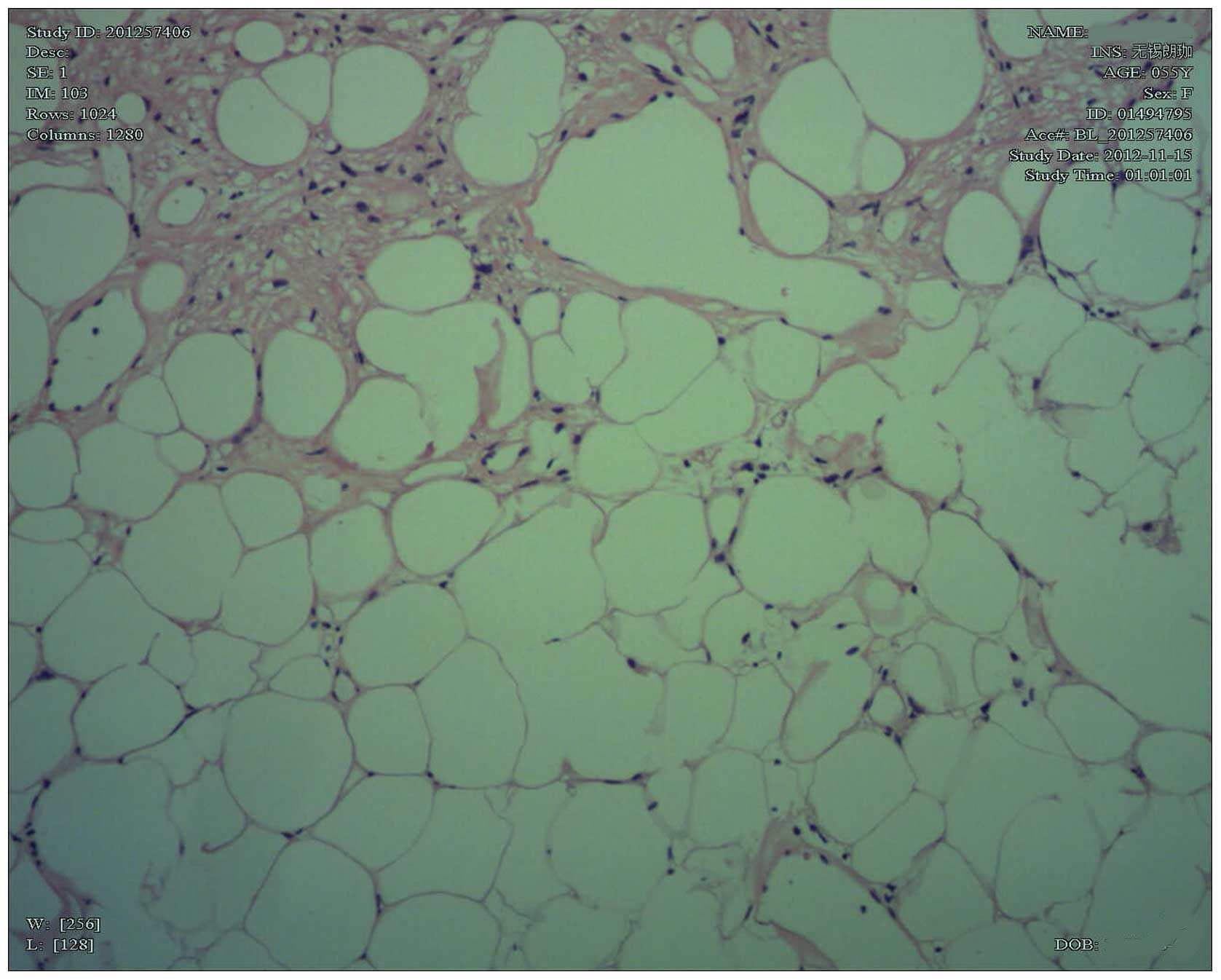
The anatomopathological examination revealed that
the mass was a non-capsulated, regular lesion measuring 10×11×12
mm, with a firm and fibroelastic consistency. In addition,
microscopic analysis revealed blood vessels, well-differentiated
adipose tissue and polygonal cells (Fig. 3). Immunohistochemistry revealed
pan-cytokeratin (−), melan-A (+), HMB45 (−), HHF35 (−), p53 (−),
S-100 (+), desmin (−), cluster of differentiation 68 (−) and smooth
muscle actin (+) expression, which is consistent with pulmonary
hamartoma.
The patient recovered well and was discharged on the
third postoperative day. After six months of postoperative
follow-up, the patient has presented no signs of increasing
multiple pulmonary nodules as assessed by computed tomography.
Discussion
Pulmonary hamartoma account for 77% of all benign
lung tumors and 4% of all solitary lung nodules (4–5). The
lesion has been described as a benign neoplasm of the fibrous
connective tissue of the bronchi surrounded by respiratory
epithelium that commonly contains cartilage and adipose tissue,
which does not comply with the usual histological distribution of
the lung (6). In total, 90% of the
hamartomas manifest as a solitary peripheral mass (5) and rarely occur in the form of multiple
lesions (7). In addition, hartoma
is more common in adults and the incidence rate is twice as high in
males compared with females. The mean growth rate of hamartoma is
3.2±2.6 mm/year (8) and the
occurrence of malignancy in hamartoma patients is possible. Certain
studies have found that the incidence of bronchial carcinoma is
6.3-fold higher in patients with hamartoma than in a normal
population, indicating the presence of an etiologic association
(9). The appearance of pulmonary
nodules during the follow-up evaluation of patients who have
undergone nephrectomy is often confusing. Nine patients with a
history of radical nephrectomy for renal cell carcinoma underwent
the surgical removal of newly detected pulmonary nodules at the
Hiroshima University Hospital (Hiroshima, Japan). Of these nine
patients, six had metastatic lung tumors, two had bronchogenic
primary carcinomas and one had a granulomatous infection (10).
The diagnostic algorithm in pulmonary hamartomas
usually begins with structural imaging studies. Chest X-ray and CT
are useful, however, magnetic resonance imaging has a limited role.
Hamartomas are benign lesions containing normal pulmonary tissue
and CT observations, such as internal fat or popcorn-like
calcifications, are useful for distinguishing hamartomas from other
malignancies (11–12). Certain studies have also
demonstrated the presence of adipose tissue in 50% of the
hamartomas that were evaluated by computed tomography (10). Radiological differentiation between
benign and malignant nodules is determined according to size,
margins, contour and internal characteristics, however, the
interpretation may be fallacious (11–13).
For example, in the present case, the lesion did not exhibit any
such features on the CT scan. The CT also failed to reveal any
signs of associated pulmonary tuberculosis.
FDG-PET scan is a useful non-invasive assessment in
the differential diagnosis of indeterminate lung lesions,
particularly in cases with an intermediate risk of malignancy
(14). False-positive results from
FDG-PET have been associated with focal infections or inflammatory
conditions. In a previous study, six patients with pulmonary
hamartoma underwent FDG-PET and only one demonstrated an
accumulation of FDG (15–16). Tumors with a low metabolic rate,
such as bronchioloalveolar carcinomas or carcinoids, may result in
false-negative results, although, more recent results often
describe mild FDG uptake in carcinoid lesions (17–18).
Scott et al (19) also
reported false-negative results in two patients with very small
tumors. The rate of glycolysis in the tumor may have resulted in
the low rate of FDG uptake and the actual amount of FDG uptake by
the malignant tissue may have been relatively small, which resulted
in a low overall FDG uptake. Furthermore, false-negative results
are also possible in small tumors due to partial volume
effects.
As the preoperative diagnosis of pulmonary hamartoma
is often difficult, surgical resection is required for the
differential diagnosis of lung cancer or metastatic lung tumors,
unless clinical imaging reveals typical observations of pulmonary
hamartoma. In the present study, considering the presence of
multiple pulmonary nodules and the patient’s history of radical
nephrectomy, metastasis was suggested as the initial diagnosis.
Therefore, the histopathological diagnosis of hamartoma was
unpredicted. The pulmonary nodules presented in patients who have
undergone nephrectomy for renal cancer are not always pulmonary
metastases and the confirmation of the histopathological diagnosis
is fundamentally important to determine the optimal treatment
method.
In conclusion. bronchoscopy with a biopsy is
recommended for endobronchial lesions, as well as for patients with
pulmonary symptoms, such as a cough, hemoptysis, recurrent
pulmonary infections or atelectasis (20). In addition, percutaneous
transthoracic aspiration biopsy diagnoses 85% of hamartomas, that
present close to the thoracic wall, by differentiating them from
nodules of other etiologies, such as renal cancer lung metastasis.
Despite thorough clinical assessment with advanced imaging
technology and needle biopsy, a number of patients continue to
undergo surgery for benign disease. Therefore, future studies are
required to identify novel strategies for the diagnosis and
treatment of early-stage lung cancer (21). In cases where a diagnosis has not
been determined due to the stiffness of the tumor, rendering a
percutaneous biopsy useless, enucleation or resection via open
thoracotomy or video-assisted resection is recommended (22).
Acknowledgements
The present study was supported by a grant from the
National Key Clinical Specialty Construction Project of China.
References
|
1
|
Tsakiridis K, Visouli AN, Zarogoulidis P,
Mpakas A, Machairiotis N, Stylianaki A, Katsikogiannis N,
Courcoutsakis N and Zarogoulidis K: Lost in time pulmonary
metastases of renal cell carcinoma: complete surgical resection of
metachronous metastases, 18 and 15 years after nephrectomy. J
Thorac Dis. 4(Suppl 1): S69–S73. 2012.
|
|
2
|
Oddsson SJ, Hardarson S, Petursdottir V,
Jonsson E, Sigurdsson MI, Einarsson GV, Pfannschmidt J and
Gudbjartsson T: Synchronous pulmonary metastases from renal cell
carcinoma - a whole nation study on prevalence and potential
resectability. Scand J Surg. 101:160–165. 2012. View Article : Google Scholar
|
|
3
|
Hamano A, Yamashita Y, Yumura Y, Takase K,
Ogo Y, Noguchi S, Morohoshi T, Satomi Y and Fukuda M: Three cases
of pulmonary hamartoma appearing after radical nephrectomy for
renal cell carcinoma. Hinyokika Kiyo. 51:805–807. 2005.(In
Japanese).
|
|
4
|
Arrigoni MG, Woolner LB, Bernatz PE,
Miller WE and Fontana RS: Benign tumors of the lung. A ten-year
surgical experience. J Thorac Cardiovasc Surg. 60:589–599.
1970.PubMed/NCBI
|
|
5
|
Khouri NF, Meziane MA, Zerhouni EA,
Fishman EK and Siegelman SS: The solitary pulmonary nodule.
Assessment, diagnosis, and management. Chest. 91:128–133. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bateson EM: So-called hamartoma of the
lung - a true neoplasm of fibrous connective tissue of the bronchi.
Cancer. 31:1458–1467. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bennett LL, Lesar MS and Tellis CJ:
Multiple calcified chondrohamartomas of the lung: CT appearance. J
Comput Assist Tomogr. 9:180–182. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hansen CP, Holtveg H, Francis D, Rasch L
and Bertelsen S: Pulmonary hamartoma. J Thorac Cardiovasc Surg.
104:674–678. 1992.PubMed/NCBI
|
|
9
|
Karasik A, Modan M, Jacob CO and Lieberman
Y: Increased risk of lung cancer in patients with chondromatous
hamartoma. J Thorac Cardiovasc Surg. 80:217–220. 1980.PubMed/NCBI
|
|
10
|
Nakamoto T, Igawa M, Mitani S, Usui A,
Yoshioka S, Nishiki M and Usui T: Pulmonary nodules in patients
with a history of radical nephrectomy for renal cell carcinoma. Int
J Urol. 2:229–231. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Diederich S and Das M: Solitary pulmonary
nodule: detection and management. Cancer Imaging. 6:S42–S46. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wahidi MM, Govert JA, Goudar RK, Gould MK
and McCrory DC; American College of Chest Physicians. Evidence for
the treatment of patients with pulmonary nodules: when is it lung
cancer? ACCP evidence-based clinical practice guidelines (2nd
edition). Chest. 132(3 Suppl): S94–S107. 2007. View Article : Google Scholar
|
|
13
|
Jeong YJ, Yi CA and Lee KS: Solitary
pulmonary nodules: Detection, characterization, and guidance for
further diagnostic workup and treatment. AJR Am J Roentgenol.
188:57–68. 2007. View Article : Google Scholar
|
|
14
|
Gould MK, Fletcher J, Iannettoni MD, Lynch
WR, Midthun DE, Naidich DP and Ost DE; American College of Chest
Physicians. Evaluation of patients with pulmonary nodules: when is
it lung cancer? ACCP evidence-based clinical practice guidelines
(2nd edition). Chest. 132(3 Suppl): S108–S130. 2007. View Article : Google Scholar
|
|
15
|
Sminohara S, Hanagiri T, Kuwata T,
Takcenaka M, Oka S, Chikainsi Y, Nagata Y, Shimokawa H, Shigematsu
Y, Nakagawa M, et al: Clinical characteristics of pulmonary
hamartoma resected surgically as undiagnosed pulmonary nodule. J
UOEH. 34:41–46. 2012.(In Japanese).
|
|
16
|
Okagawa T, Uchida T and Suyama M:
Endobronchial hamartoma suspected lung cancer due to false positive
of fluorodeoxyglucose-positron emission tomography; report of a
case. Kyobu Geka. 62:833–835. 2009.(In Japanese).
|
|
17
|
Zhang LN, Xue XY, Wang N and Wang JX:
Mimicking pulmonary multiple metastatic tumors: A case of primary
nodular parenchymal pulmonary amyloidosis with review of the
literature. Oncol Lett. 4:1366–1370. 2012.
|
|
18
|
Daniels CE, Lowe VJ, Aubry MC, Allen MS
and Jett JR: The utility of fluorodeoxyglucose positron emission
tomography in the evaluation of carcinoid tumors presenting as
pulmonary nodules. Chest. 131:255–260. 2007. View Article : Google Scholar
|
|
19
|
Scott WJ, Schwabe JL, Gupta NC, et al:
Positron emission tomography of lung tumors and mediastinal lymph
nodes using [18F]fluorodeoxyglucose. The Members of the PET-Lung
Tumor Study Group. Ann Thorac Surg. 58:698–703. 1994.
|
|
20
|
Cosío BG, Villena V, Echave-Sustaeta J, de
Miguel E, Alfaro J, Hernandez L and Sotelo T: Endobronchial
hamartoma. Chest. 122:202–205. 2002.
|
|
21
|
Smith MA, Battafarano RJ, Meyers BF, Zoole
JB, Cooper JD and Patterson GA: Prevalence of benign disease in
patients undergoing resection for suspected lung cancer. Ann Thorac
Surg. 81:1824–1828. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ramming KP: Surgery for pulmonary
metastases. Surg Clin North Am. 60:815–824. 1980.
|