Introduction
Lung cancer is one of the most common types of
malignant tumor (1,2) accounting for 22.7% of all cases of
malignant tumor (3). The mortality
rate of lung cancer in China has increased by 464.84% in the past
30 years (4). Furthermore, the
incidence rate of lung cancer in China has exhibited the largest
increase and poses the most severe threat compared with other types
of cancer (5), therefore, an early
and accurate diagnosis is required. Multi-slice spiral computed
tomography (CT) is an important examination measure for the early
screening of lung cancer and fully demonstrates the morphological
characteristics of lung lesions (6,7).
Typical types of lung cancer are easily diagnosed by imaging,
biopsy and additional measures. However, there is a lack of
knowledge concerning the features of atypical or rare types of lung
cancer, thus, these types of cancer are subject to misdiagnosis,
missed diagnosis and treatment delay. Among these types of cancer,
solitary thin-walled cavity lung cancer is particularly rare
(8–11). Doctors often lack the understanding
of this type of cancer and, therefore, misdiagnose it. In the
current study, 16 cases of thin-walled cavity lung cancer are
included and summarized. CT and positron emission tomography (PET)
manifestations, as well as the pathological features of these
cases, were analyzed to determine their imaging characteristics
with the aim of improving the diagnosis rate.
Patients and methods
General data
A total of 16 patients with pathologically confirmed
thin-walled cavity lung cancer from the Shandong Cancer Hospital
(Jinan, China) were enrolled in the present study between July 2008
and April 2012. These cases included 12 males and four females aged
34–69 years (mean age, 52 years). Among these, 11 cases did not
manifest symptoms and were diagnosed only by physical examination.
In addition, three cases suffered with a cough and chest-related
distress, one case presented with hoarseness, tightness in the
chest, pectoralgia and low-grade fever, and one case complained of
right shoulder pain as well as a cough, which was accompanied by
white phlegm. The present study was conducted in accordance with
The Declaration of Helsinki and with approval from the Ethics
Committee of Shandong Cancer Hospital. Written informed consent was
obtained from all participants.
CT examination
A 16-slice spiral CT scanner (Siemens Somatom
Sensation Company, Erlangen, Germany) was used with a
conventional-slice thickness of 5 mm. All of the lesions were
reconstructed at a slice thickness of 1.5 mm and amplified. The
patients were instructed to lie in a supine position, raise their
arms, breathe in and hold their breath. Volume scanning was
subsequently conducted. The scanning range began from the superior
aperture of the thorax and ended at the posterior costophrenic
angle of the left and right lungs. Abdominal scanning was conducted
on certain patients and enhancement scanning was conducted on all
patients. Nonionic contrast medium iohexol (Beijing BeiLu
Pharmaceutical, Co., Ltd., Beijing, China; 300 mgI/ml, 80–100 ml)
was used, and the injection rate ranged between 2.5 and 3.0 ml/sec.
Scanning was conducted 30 and 90 sec after the contrast medium had
been injected.
18F-fluorodeoxyglucose (FDG)
PET/CT imaging method
A Discovery LS PET/CT instrument (GE Healthcare,
Piscataway, NJ, USA) was used and 18F-FDG was generated
by a PET tracer cyclotron (GE Healthcare) with a radiochemical
purity of >95%. Following >4 h of fasting, the patients (in a
tranquil state) were injected with the imaging agent
18F-FDG (259–444 MBq) via an intravenous T-shaped tube.
The total body scan ranged from the mid-thigh to the top of the
head. The PET and CT images were transferred to the eNTEGRA (GE
Healthcare) workstation for the alignment fusion of the images.
Imaging analysis
The CT images of the lesions were independently
analyzed by two experienced imaging doctors to observe the cavity
wall thickness, wall nodules, compartment locations and enhancement
characteristics. In addition, the concentrations of
18F-FDG in the cavity wall nodules of the lesions were
analyzed.
Pathological detection
Biopsy samples were fixed in 10% neutral buffered
formalin and dehydrated in a series of 50, 70 and 80% alcohols and
distilled water. Following embedding in paraffin wax, sections were
sectioned and stained with haematoxylin and eosin prior to
examination under light microscopy (BX5IPF, Olympus Corporation,
Tokyo, Japan).
Results
Findings from chest imaging
All of the thin-walled cavities of the 16 patients
were located in the peripheral lung field and exhibited no signs of
lobulation or spicules. Among these patients, three cases of
lesions were located in the posterior segment of the right lung
upper lobe, four were located in the posterior segment of the right
lung lower lobe, two were located in the superior lobe
apicoposterior segment of the left lung, three were located in the
lower lobe basal segment of the left lung, three were located in
the lower lobe posterior basal segment of the left lung and one in
the lower lobe posterior basal segment of the left lung. The
maximum cavity section was 6.5×5.2 cm and the minimum cavity
section was 1.2×1.0 cm. The maximum size of the wall nodule was
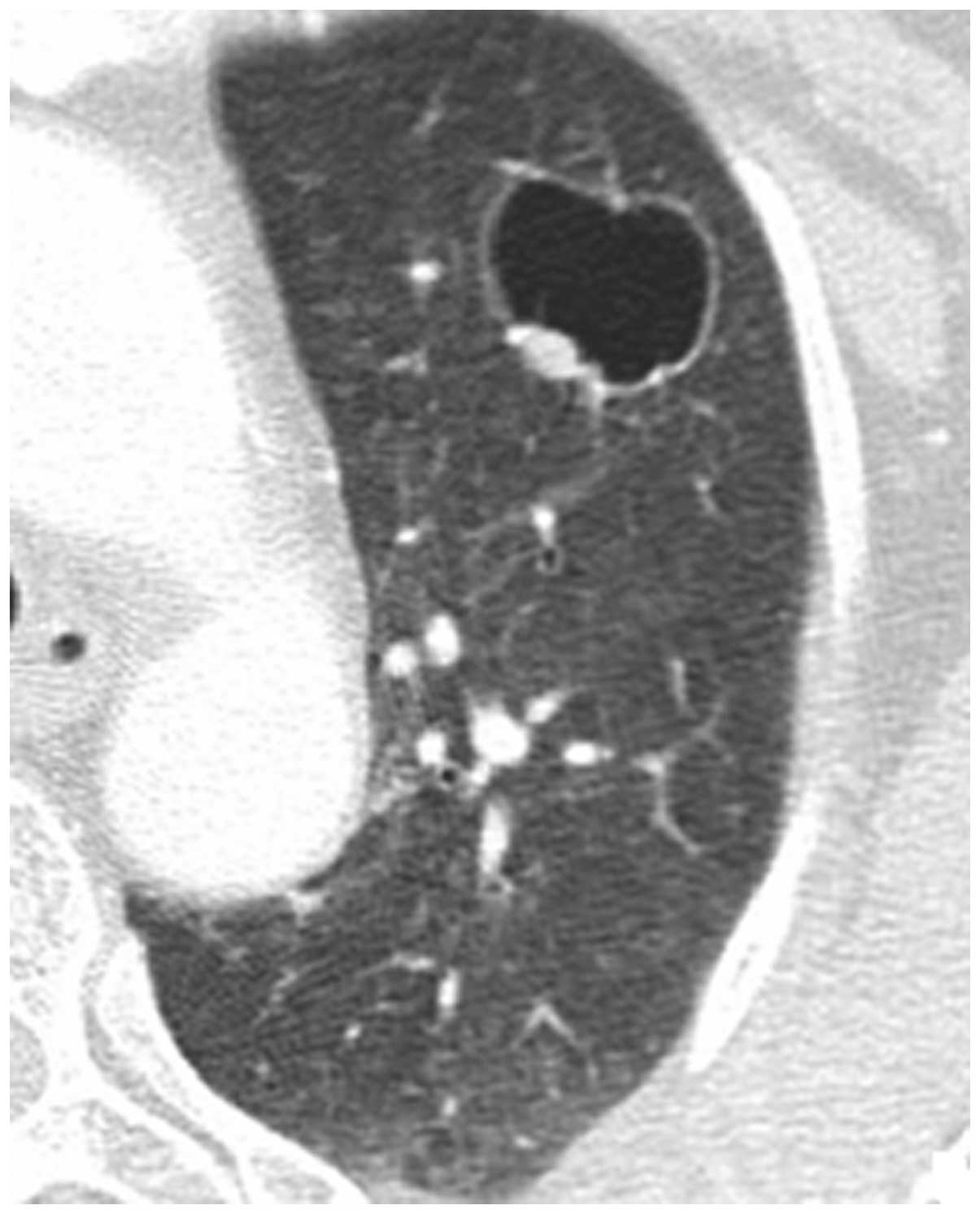
1.0×0.8 cm and the cavity wall thickness was 0.3–1.2 mm. Two cases
(12.5%) presented with a uniform thickening of the cavity wall and
wall nodules (Fig. 1). Three cases
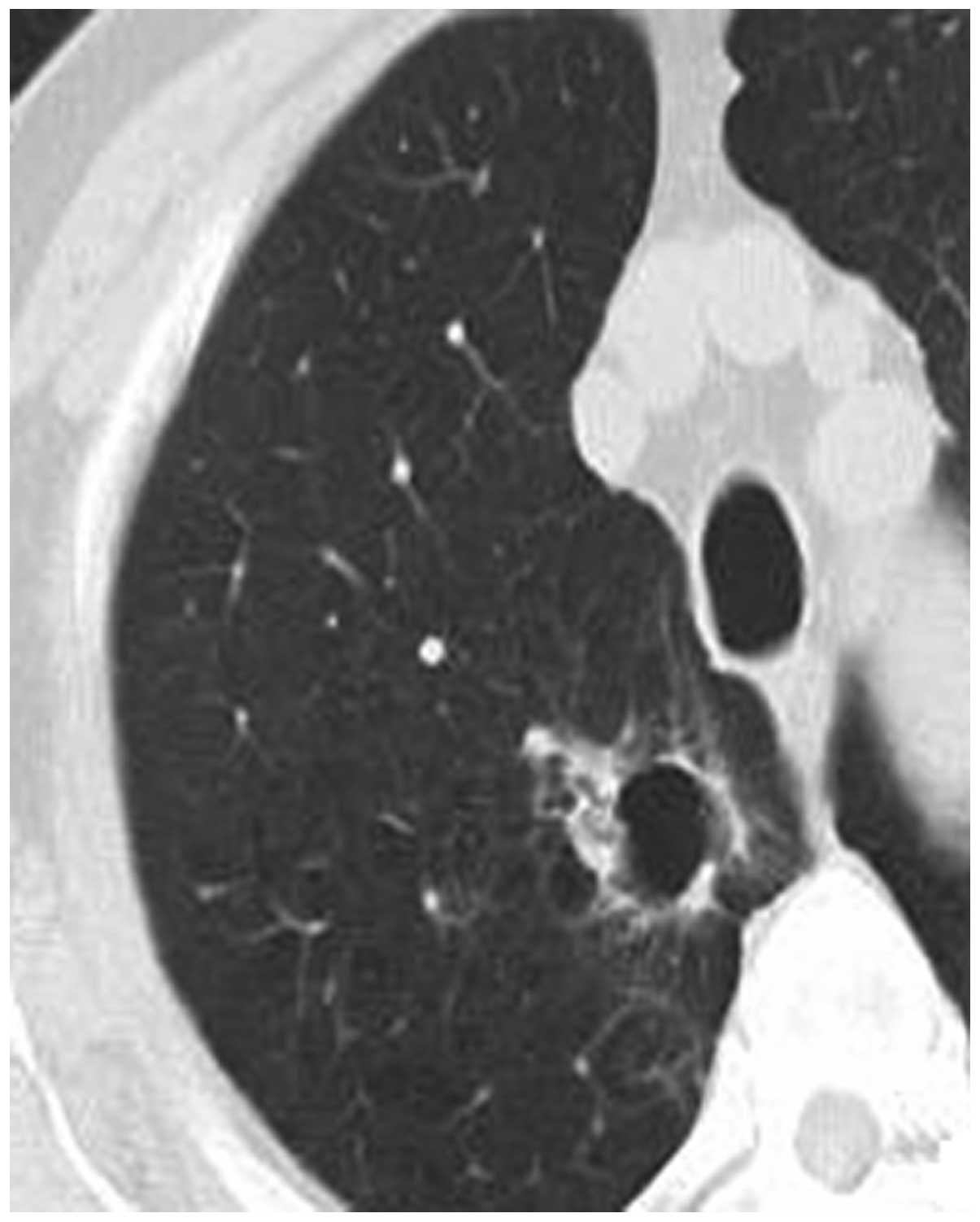
(18.75%) presented with an uneven thickening of the cavity wall and
wall nodules (Fig. 2). Three cases
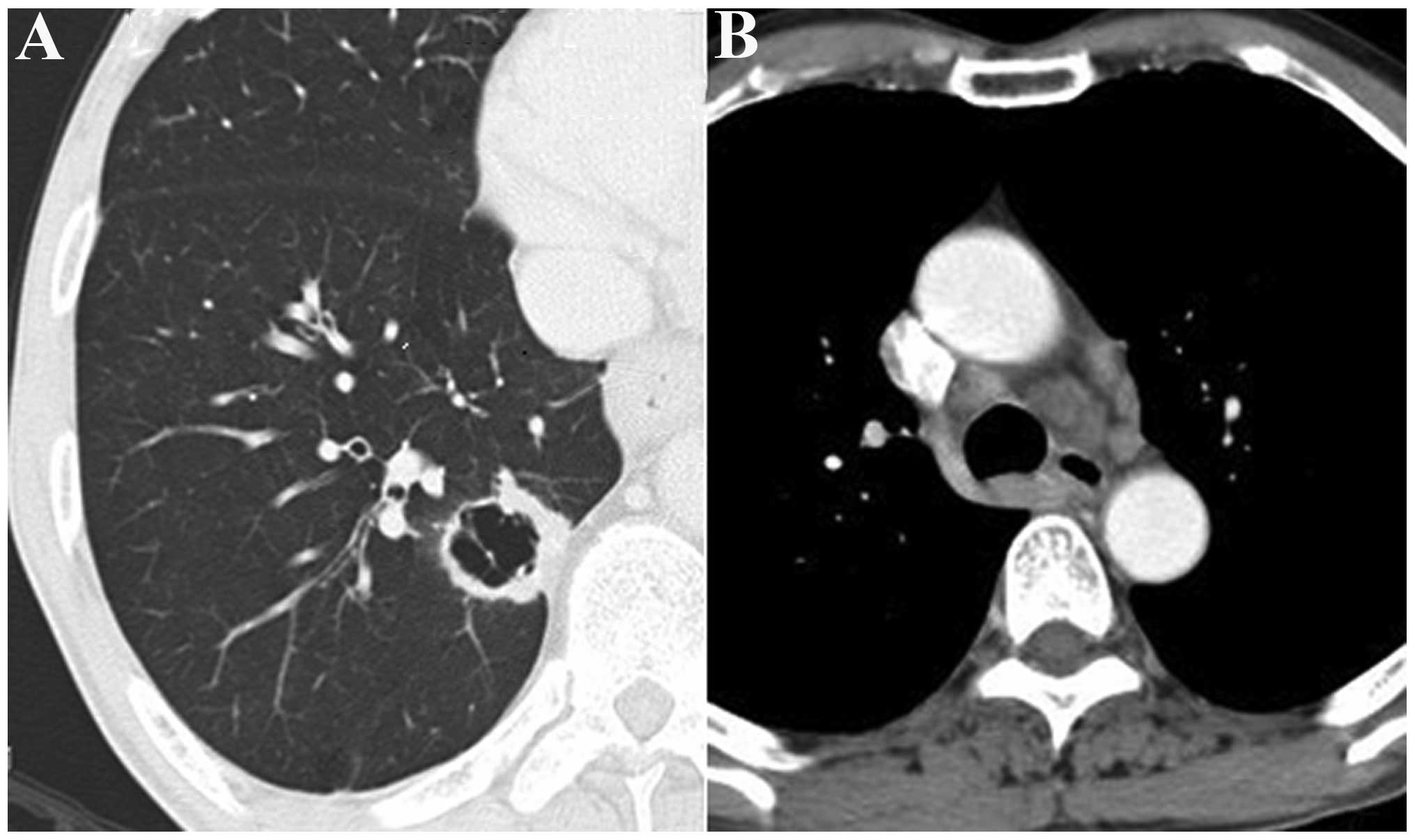
(18.75%) presented with an uneven thickening of the cavity wall
(Fig. 3A) and multiple metastases
of the mediastinal lymph node, and partial lymph nodes were fused
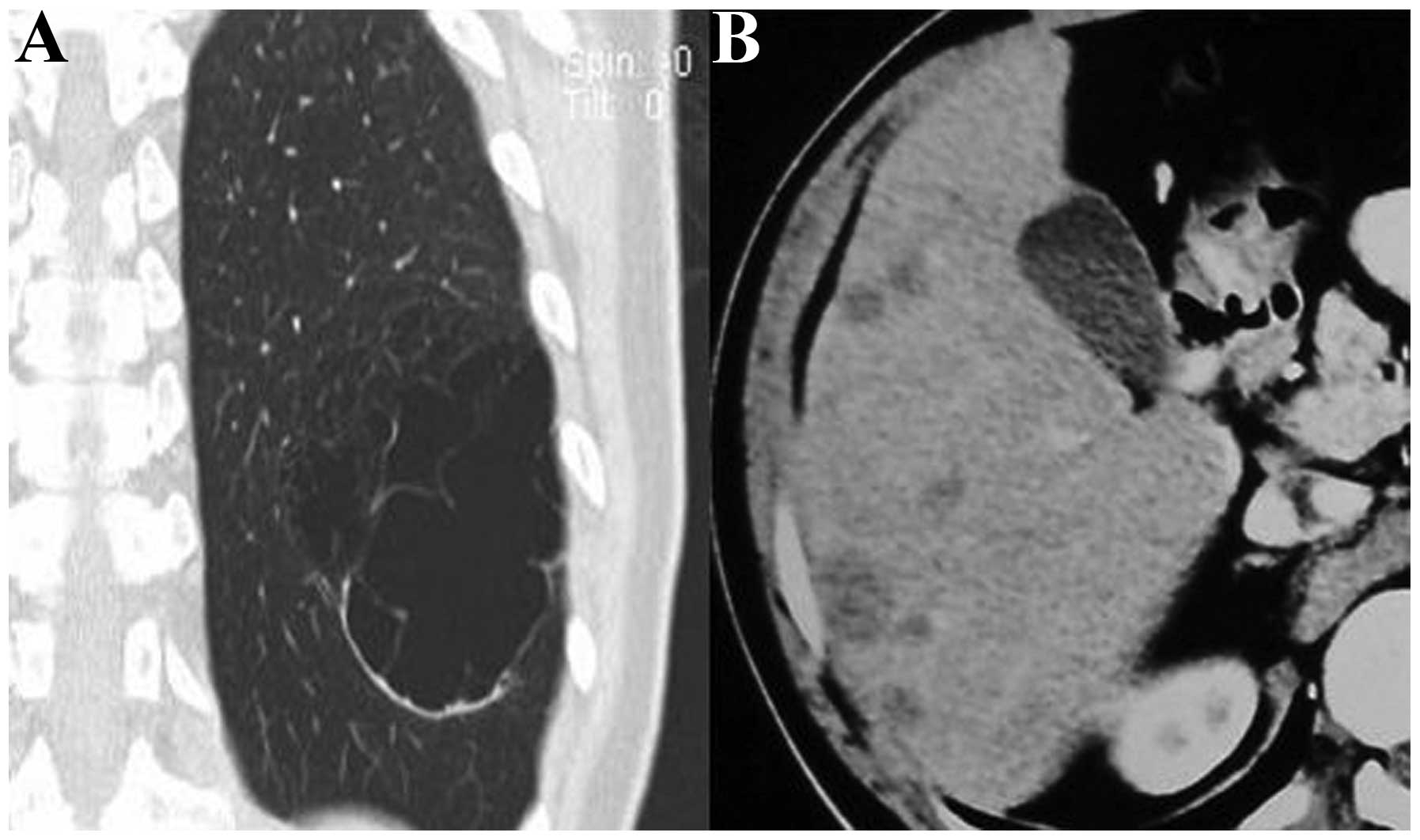
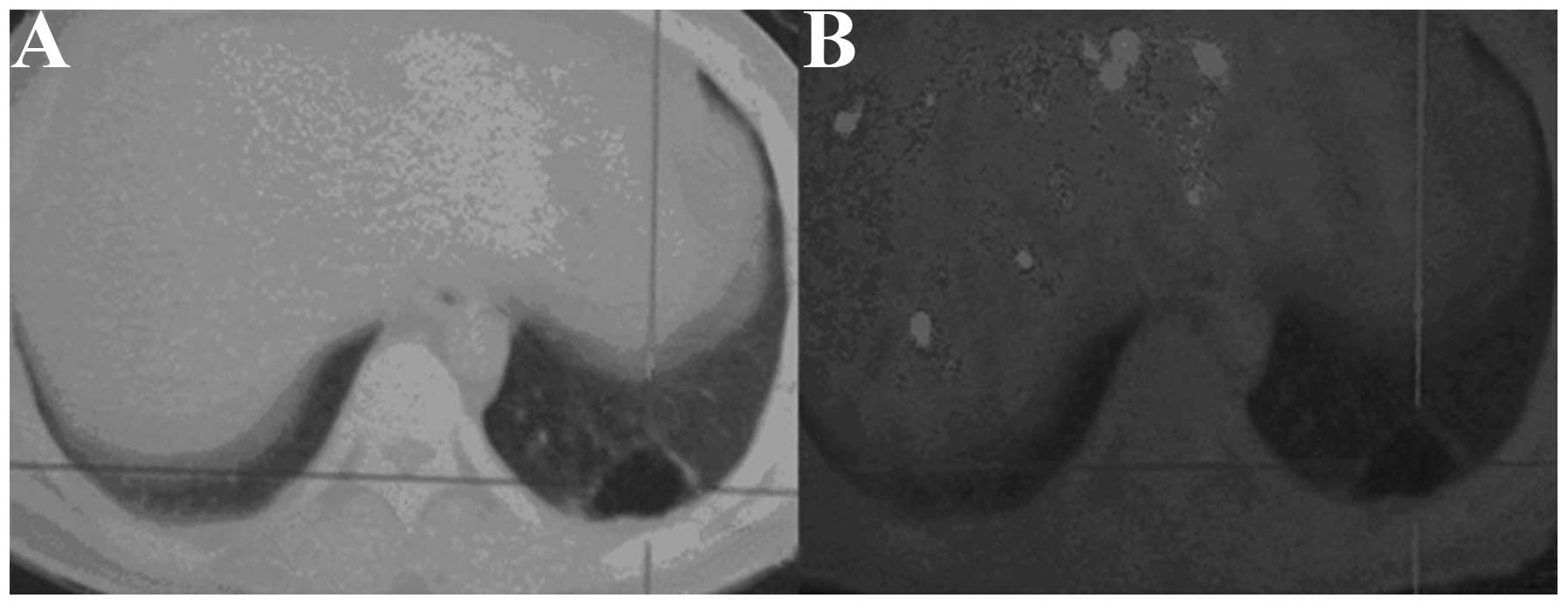
into conglobation (Fig. 3B). One
case (6.25%) presented with a large cavity, local thickening of the
wall, compartments in the cavity (Fig.
4A) and multiple metastatic tumors of the liver (Fig. 4B). Three cases (18.75%) presented
with compartments in the cavity and exhibited no signs of
metastasis. Two cases (12.5%) presented with wall nodules on the
cavity wall (Fig. 5A) and exhibited
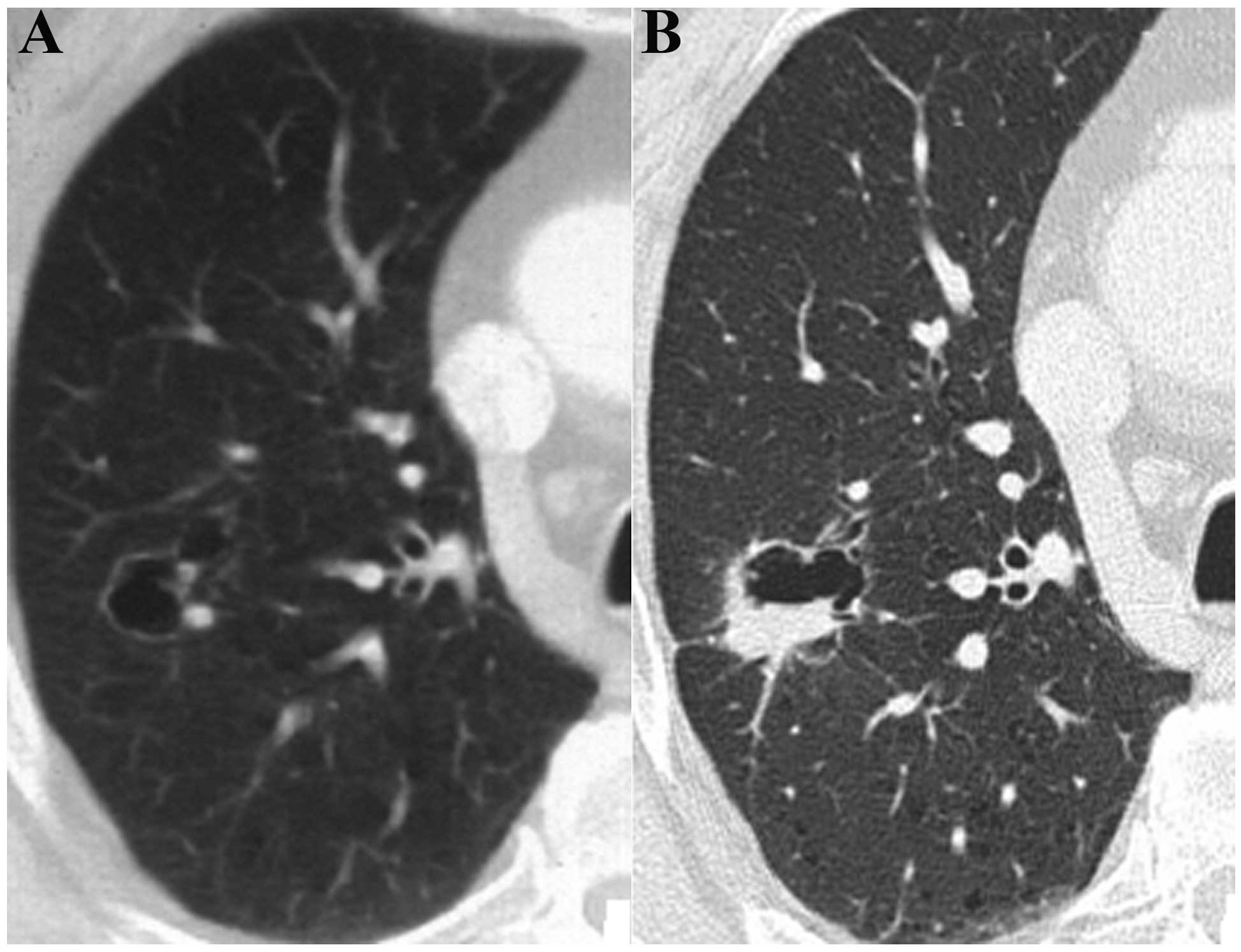
marginally increased standard uptake values (SUVs; Fig. 5B). One case (6.25%) presented with a
cystic cavity in the posterior segment of the right lung upper lobe
(Fig. 6A), no compartment, a wall
thickness of ~1.0 mm and punctiform wall nodules. The cavity size
was ~1.4×1.2 cm, no swollen lymph node was visible in the
mediastinum, and the bilateral hilar and other organs demonstrated
no signs of metastasis. Reexamination after 18 months demonstrated
a marginally enlarged cavity (~1.6×1.5 cm), significantly enlarged
and moderately enhanced wall nodules, a thickened wall (~2.0 mm)
and no compartments or signs of metastasis in the cavity (Fig. 6B). For the other patient, a cystic
cavity (~2.4×2.6 cm) was identified in the superior lobe
apicoposterior segment of the left lung. The cavity wall presented
local thickening and smooth edges and neither compartments nor
signs of metastasis were identified in the cavity. Reexamination on
the third and 12th month showed no variation in the lesions, and
reexamination at 18 months demonstrated an enlarged cavity (2.8×2.2
cm) and wall nodules. Numerous swollen lymph nodes were observed in
the mediastinum and the short diameter of the large lymph nodes was
~0.8 cm.
Results of surgery and pathology
Six patients were not subjected to surgery due to
mediastinal lymph node metastasis and liver metastasis. Therefore,
biopsy samples were acquired by needle punctuation under CT
guidance. For the 10 remaining cases, the affected lung was
subjected to a partial lobectomy. The pathological results
confirmed that the 16 patients were diagnosed with adenocarcinoma.
Among these cases, four had moderately differentiated
adenocarcinoma, five had highly differentiated adenocarcinoma
accompanied by bronchial alveolar carcinoma, one had slightly
differentiated adenocarcinoma accompanied by neuroendocrine
carcinoma, two had mixed-type adenocarcinoma (bronchial alveolar
carcinoma and alveolar-type adenocarcinoma) with visceral pleura
involvement and four had highly differentiated adenocarcinoma.
Pathological features
Light microscopy indicated that the cancer cells in
12 cases had directly diffused along the alveolar and bronchial
walls and the pulmonary mesenchyme. Furthermore, the results
demonstrated that the alveolar and bronchial walls were not damaged
(Fig. 7A). In four cases, the
cancer cells had invaded the bronchial wall, which resulted in
bronchial wall stenosis (Fig. 7B).
Necrotic tumor cells were not visible in any of the 16
patients.
Discussion
Lung cancer is one of the most common types of
malignant tumor and the progression of this type of cancer is
associated with the pathological type. Solitary thin-walled cavity
lung cancer is a unique and rare type of lung cancer, which is
seldom reported. Therefore, this type of cancer is subject to
misdiagnosis due to inadequate knowledge concerning its onset and
progression. The improvement of diagnostic levels, particularly the
invention of multi-slice spiral CT, has advanced our understanding
of lung cancer. Cancer cells directly diffuse along the alveolar
and bronchial walls, and the pulmonary mesenchyme. Bronchi
stricture occurs and the structures of the alveolar and bronchial
walls are not damaged (12,13). In other pathways, the cancer cells
invade the bronchial wall, which results in bronchial wall stenosis
(14). Therefore, the bronchi form
a valve leading to excessive gas accumulation in the tumor that
increasingly expands the cavities. Partial cavities subsequently
break to form larger hollow cavities and tumors grow along the
hollow cavity wall to form wall nodules or a cavity wall with an
uneven thickness. In the present study, the cancer cells of six
patients were observed to directly diffuse along the alveolar and
bronchial walls, as well as the pulmonary mesenchyme. However, the
alveolar and bronchial walls were not damaged. In 10 cases, the
cancer cells invaded the bronchial wall, which resulted in
bronchial wall stenosis. Necrotic tumor cells were not visible in
any of the 16 patients.
Xue et al (15) reported that 18 cases of thin-walled
cavity lung cancer were adenocarcinomas and in the present study,
all 16 cases were adenocarcinomas. Among these cases, four had
moderately differentiated adenocarcinoma, five had highly
differentiated adenocarcinoma accompanied by bronchial alveolar
carcinoma, one had slightly differentiated adenocarcinoma
accompanied by neuroendocrine carcinoma, two had mixed-type
adenocarcinoma (bronchial alveolar carcinoma and alveolar-type
adenocarcinoma) with visceral pleura involvement and four had
highly differentiated adenocarcinomas. These results are consistent
with the study by Xue et al (15). Liu (16) also reported 25 cases of thin-walled
cavity lung cancer. The pathological types included adenocarcinoma
(21 cases), metastatic tumor (two cases), large-cell carcinoma (one
case) and atypical hyperplasia (one case). Further studies are
required to determine whether or not other types of cancer are
present (for example, squamous cell and small-cell carcinoma).
In the present study, the mean age of the 16 cases
was 52 years and the number of male patients compared with female
patients was higher (12:4). The clinical manifestations of these
patients varied with the lesion size. The tumors in the current
study occurred in the periphery of the lungs. By contrast, Xue
et al (15) described a
different distribution pattern in 18 cases of cavity-type lung
cancer. Given that the sample size of the current study is small,
further studies are required to investigate whether the incidence
rate is associated with gender and whether tumors primarily occur
in the periphery of the lungs.
Few studies have examined thin-walled cavity lung
cancer; its malignant signs are atypical, therefore, this type of
lung cancer is easily missed during diagnosis. In the present
study, 16 patients presented with cavities of varying sizes. The
cavities contained gas, were located in the periphery of the
affected lung and had no sign of lobulation or spicules. The
partial cavities were of uneven wall thickness and their inner
compartments were visible and became gradually enlarged.
Specifically, the cavities of two patients were gradually enlarged
and their wall nodules were pronounced. The partial-cavity patients
exhibited thick cavity walls and presented with lymph node or organ
metastasis. These CT observations are consistent with the malignant
manifestations of thin-walled cavity lung cancer that have
previously been observed (15) and
are important signs for diagnosing this type of lung cancer. In the
current study, the cavity wall of partial-cavity patients was thick
and formed local nodules. Two patients exhibited thick cavity walls
and PET demonstrated that the SUVs were 1.2 and 1.4 higher compared
with normal values. Postoperative pathological results indicated a
diagnosis of pulmonary adenocarcinoma. Given that the sample size
of the present study was small, further investigations are required
to determine whether or not these signs may be used as judgment
standards for cystic lung cancer.
Solitary thin-walled cavity lung cancer is
distinguishable from peripheral pulmonary cysts and thin-walled
cavernous lung cancer. Pulmonary cyst walls are thin with uniform
thickness, however, without wall nodules. Pulmonary cysts are not
associated with compartments, lymphadenectasis or distant organ
metastasis. In addition, long-term observations reveal no changes,
and identification and diagnosis are simple to perform. CT signs of
thin-walled cavernous lung cancer are widely reported and its
malignant signs are clear, resulting in an easy diagnosis. For
thin-walled cavernous lung cancer, the majority of pathological
types belong to squamous carcinoma (17). The formation mechanism is
characterized by extremely rapid tumor growth and central
tumor-tissue necrosis, and necrotic components are formed by
bronchial elimination. Imaging demonstrates that the cavernous wall
is thicker than the cavity wall, the inner edges are rough, no
compartments are found, and lobulation, spicules and pleural
indentation are common.
In conclusion, thin-walled cavity lung cancer is
rare with an incidence rate of 1.00–2.07% (17). Furthermore, there is a lack of
knowledge regarding solitary thin-walled cavity lung cancer,
therefore, it is easily misdiagnosed as a benign lesion, which
delays treatment. Lung cancer may be indicated by the following
clinical signs: Uneven thickening of the thin-walled cavity wall;
wall nodule formation; the presence of compartments in the cavity;
SUV value elevation; a thin-walled cavity accompanied by
mediastinal lymph node or distant organ metastasis; or cavity
enlargement under long-term observation. Further studies are
required to determine whether certain signs, including an increase
in the SUV of the cavity wall and enhancement of the wall nodule,
may be used as judgment standards for solitary thin-walled cavity
lung cancer.
References
|
1
|
Bruzzi JF and Munden RF: PET/CT imaging of
lung cancer. J Thorac Imaging. 21:123–136. 2006.
|
|
2
|
Fritscher-Ravens A, Bohuslavizki KH,
Brandt L, Bobrowski C, Lund C, Knöfel WT and Pforte A: Mediastinal
lymph node involvement in potentially resectable lung cancer:
comparison of CT, positron emission tomography, and endoscopic
ultrasonography with and without fine-needle aspiration. Chest.
123:442–451. 2003.
|
|
3
|
Chen Z: Third national retrospect
port-check of death-causation. 1st edition. Peking Union Medical
College Press; Beijing, China: pp. 153–154. 2008
|
|
4
|
Kong LZ and Zhao P: Chinese Cancer
Mortality Report-Third national retrospect spot-check of
death-causation. 1st edition. People’s Medical Publishing House;
Beijing, China: pp. 301–303. 2010
|
|
5
|
Dong ZW, Qiao YL, Li LD, et al: Report of
Chinese cancer control strategy. Bullet Chin Cancer. 11:250–260.
2002.
|
|
6
|
Goldin JG, Brown MS and Petkovska I:
Computer-aided diagnosis in lung nodule assessment. J Thorac
Imaging. 23:97–104. 2008.
|
|
7
|
Swensen SJ, Jett JR, Hartman TE, et al: CT
screening for lung cancer: five-year prospetive experience.
Radiology. 235:259–265. 2005.
|
|
8
|
Matsuoka T, Fukamitsu G, Onoda M, Uesugi
N, Kawano K and Katou T: Synchronous multiple lung cancer including
a lesion with a thin-walled cavity; report of a case. Kyobu Geka.
63:164–167. 2010.(In Japanese).
|
|
9
|
Isobe K, Hata Y, Iwata M, et al: An
autopsied case of mucinous bronchioloalveolar carcinoma associated
with multiple thin-walled cavities. Nihon Kokyuki Gakkai Zasshi.
47:512–517. 2009.(In Japanese).
|
|
10
|
Sekine A, Hagiwara E, Ogura T, et al: A
case of lung adenocarcinoma with gradual enlargement of thin-walled
cavity causing pneumothorax. Nihon Kokyuki Gakkai Zasshi.
46:552–527. 2008.(In Japanese).
|
|
11
|
Nakahara Y, Mochiduki Y and Miyamoto Y:
Percutaneous needle washing for the diagnosis of pulmonary
thin-walled cavitary lesions filled with air. Intern Med.
46:1089–1094. 2007.
|
|
12
|
Swensen SJ, Viggiiano RW, Midthun DE, et
al: Lung nodule enhancement at CT: multicenter study. Radiology.
214:73–80. 2000.
|
|
13
|
Tuddenham WJ: Glossary of terms for
thoracic radiogy: recommendation of the Nomenclature Committee of
the Fleischner Society. AJR Am J Roentgenol. 143:509–517. 1984.
|
|
14
|
He WT: Analysis of adenocarcinoma with
cavitation misdiagnosed as tuberculosis in lung. J Pract Radiol.
17:47–48. 2001.
|
|
15
|
Xue X, Wang P, Xue Q, et al: Comparative
study of solitary thin-walled cavity lung cancer with computed
tomography and pathological findings. Lung cancer. 78:45–50.
2012.
|
|
16
|
Liu L: CT characteristics and pathological
correlation of lung tumor with cysts. China PLA Postgrad Med School
Press; Beijing: pp. 180–182. 2011
|
|
17
|
Yin ZF: Chest CT diagnostics. 1st edition.
Science and Technology Press; Jinan, Shandong: pp. 234–236.
1996
|