Introduction
Chordomas are low- to intermediate-grade malignant
tumors that recapitulate the notochord. Etiologically, chordomas
belong to the dysontogenetic bone tumors and occur predominantly in
the region of the clivus (1).
Corresponding to their course of embryological development,
chordomas primarily appear in the region of the axial skeleton and
typically occur in midlife, from the ages of 40 to 60 years, and
primarily affect men (2).
The histological appearance of classical chordoma is
of a lobulated tumor composed of groups of cells separated by
fibrous septa. The cells have small round nuclei and abundant
vacuolated cytoplasm, occasionally described as physaliferous
(having bubbles or vacuoles) (3).
Although chordomas are locally invasive, metastasis
has been reported in 10–42% of cases. However, these may be the
result of the misdiagnosis of mucus-producing carcinomas of the
rectum as chordomas in certain case studies (4–6).
Previous studies suggest that secondary pulmonary and lymph-node
metastases occur most frequently, followed by liver, bone and skin
metastases (4,7).
According to the current literature, no case of a
chordoma subtype that has metastasized or transformed into another
subtype with a different histopathology and immunoreactivity has
been previously reported. This study presents a case of secondary
pulmonary conventional chordoma arising from a primary sarcomatoid
chordoma of the sacrum.
Case report
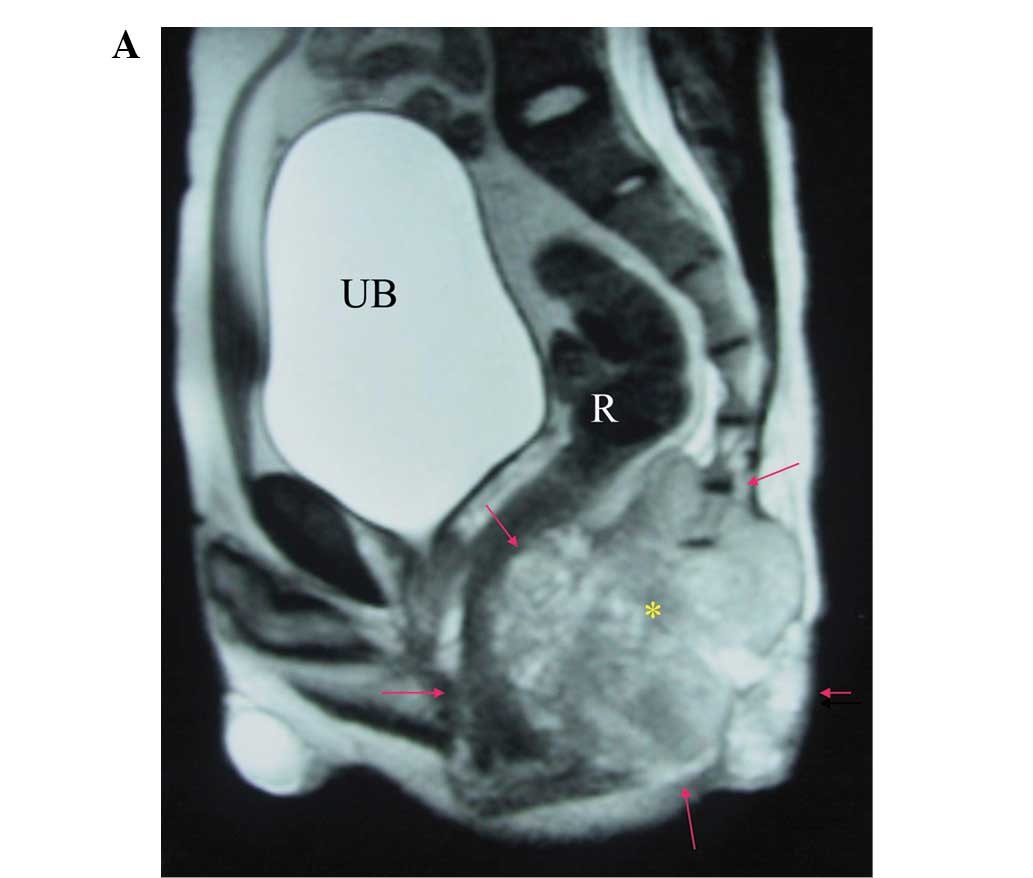
A 24-year-old man was referred to the Tri-Service
General Hospital (Taipei, Taiwan, R.O.C) presenting with a palpable
sacral mass and constipation of two months in duration. A magnetic
resonance imaging (MRI) examination of the sacral spine revealed a
large mass (measuring 13×8×7 cm) with compression of the colon
(Fig. 1A). Based on the clinical
and radiological characteristics, the patient underwent an
exploratory laparotomy with debulking of the tumor. The gross
findings of the sacral tumor included multilobulated, soft,
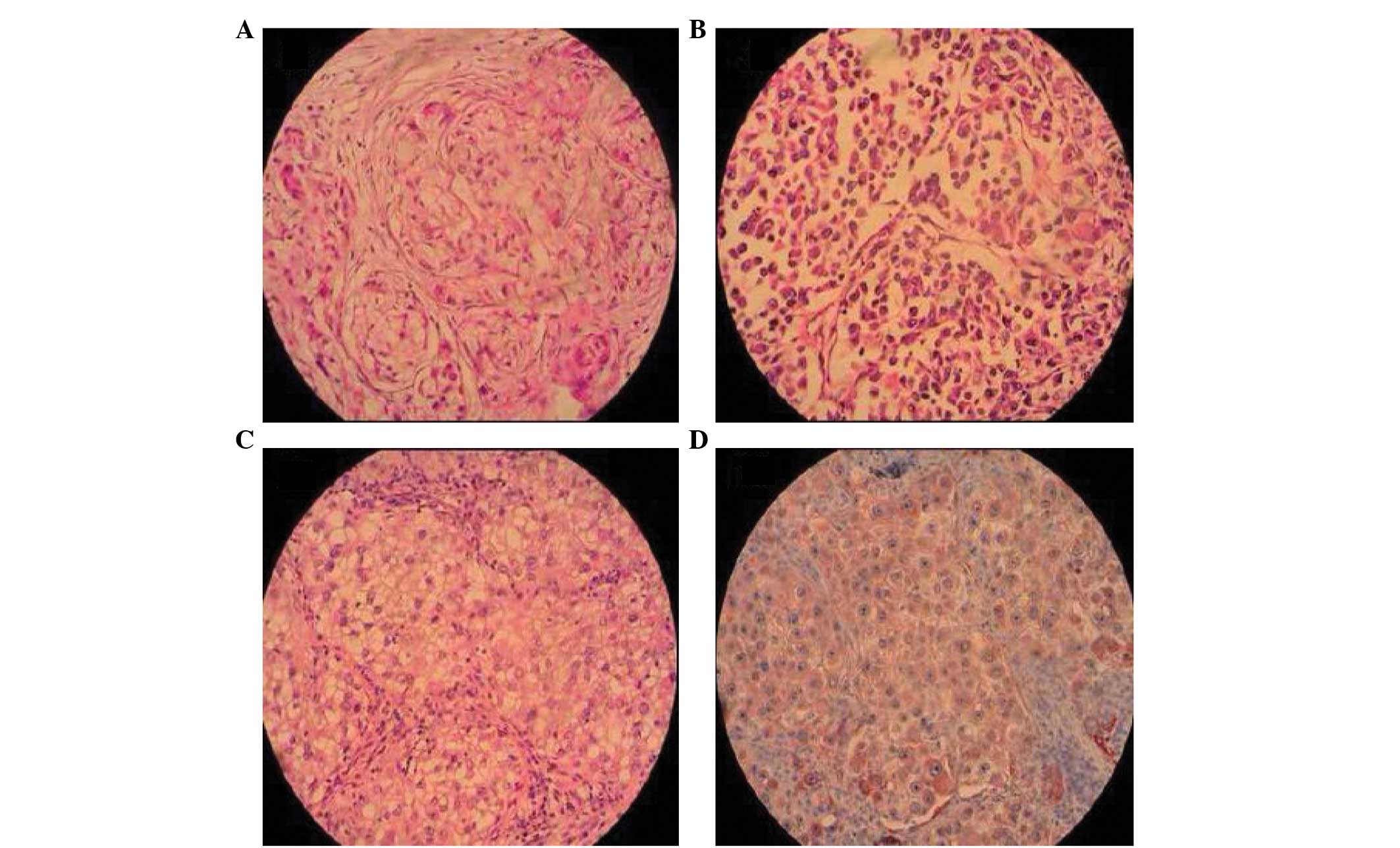
gelatinous masses with deceptively discrete margins. Microscopic
analysis revealed a lobular architecture, spindle tumor cells with
eosinophilic vacuolated cytoplasm and a mucoid matrix. The
pathological diagnosis was a sarcomatoid-type chordoma.
Immunohistochemical staining of the sacral tumor was positive for
cytokeratin (CK), epithelial membrane antigen (EMA), vimentin, S100
and periodic acid-Schiff (Fig 2A and
B). Postoperative adjuvant radiotherapy (50 Gy) was
performed.
After one year, the patient presented to the
Tri-Service General Hospital with dizziness and unstable gait of
one week in duration. Computed tomography (CT) of the brain
revealed a mass lesion over the right cerebellar vermis. A
suboccipital craniotomy was performed, with removal of the mass and
the placement of a ventriculoperitoneal shunt. The pathological
findings identified a sarcomatoid-type metastatic chordoma.
Immunohistochemical staining was positive for CK, EMA, vimentin and
S100. Intracranial whole-brain radiotherapy and adjuvant
chemotherapy with methotrexate were administered to the
patient.
After two years, a CT examination of the lungs was
performed due to a chronic cough, revealing multiple lesions,
enlarged lymph nodes and suspected metastases over the right lower
lobe (Fig. 1B). A thoracotomy with
a wedge resection of the right lower lobe was performed. The final
histopathological evaluation of the lung tumor tissue following an
immunohistochemical examination revealed a metastatic conventional
chordoma (Fig. 2C and D).
Cisplatin-based chemotherapy was administered and the disease was
stable after four courses of treatment. However, disease
progression was noted after six months and persistent salvage
chemotherapy was administered. The patient remained alive at the
end of November, 2009 and, thus, the survival time had exceeded
eight years.
Discussion
In the present case, the patient suffered from two
different subtypes of chordoma. The first was a sarcomatoid
chordoma that responded completely to an exploratory laparotomy
with debulking of the tumor and postoperative radiotherapy, with no
evidence of residual disease. The secondary chordoma was the
conventional subtype. To the best of our knowledge, this study is
the first to present the case of a different subtype of chordoma
arising at a metastatic site.
The majority of patients with conventional-type
chordoma are 50–70 years old and 50% of these tumors arise in the
sacrococcygeal region (8). The
pathological findings of conventional chordoma include sheet- or
cord-like tumor cells floating in the myxoid stroma, with abundant
vacuolated cytoplasm (physaliphorous cells). The mean survival is
4.1 years. In sarcomatoid chordomas, the tumor cells display a
storiform architecture with large, pleomorphic nuclei. A
transitional characteristic distinguishing sarcomatoid chordoma
from conventional chordoma is positive CK immunoreactivity in the
sarcomatoid component, which is required for a pathological
diagnosis (9–12). Prognosis of chordoma is associated
with the extent of surgical removal; a five-year survival of 35%
has been reported with incomplete resection if followed by
conventional radiation therapy (13).
In the dedifferentiated type of chordoma, the
pathological findings show a sharp demarcation between the
conventional chordoma and the high-grade sarcoma, with no
transitional characteristics between the two components, and
negative CK immunoreactivity in the sarcoma component (14–16).
The primary subtype of the chordoma affects the
survival period and the progressive characteristics of the tumor,
including local relapses, surgical pathway seeding and progressive
distal metastasis (5–43% of patients develop metastatic tumors in
the skin, subcutaneous tissue, bones, lungs and lymph nodes)
(17). Therefore, the subtype of a
metastatic lesion correlates with its histological differentiation
and the duration of the clinical course.
Standard treatments for conventional chordoma are
maximal surgical resection and subsequent radiotherapy (50 Gy),
even proton-beam therapy. These treatments may improve morbidity
and mortality (18). However, a
two-year mean overall survival period has previously been reported
for hematogenous metastases that include a sarcomatous component
(19). The patient in the present
case was alive at the end of 2009, despite disease progression with
metastases. In summary, to the best of our knowledge, this study
presents the first patient with primary sarcomatoid chordoma of the
sacrum with complete remission, in whom a secondary pulmonary
conventional chordoma arose from the primary tumor.
References
|
1
|
Wright D: Nasopharyngeal and cervical
chordoma-some aspects of their development and treatment. J
Laryngol Otol. 81:1337–1355. 1967.
|
|
2
|
Jenny J and Sulser H: Metastazing chordoma
of the lumbar spine. Schweiz Med Wochenschr. 103:697–701. 1973.(In
German).
|
|
3
|
Chugh R, Tawbi H, Lucas DR, Biermann JS,
Schuetze SM and Baker LH: Chordoma: the nonsarcoma primary bone
tumor. Oncologist. 12:1344–1350. 2007.
|
|
4
|
Chambers PW and Schwinn CP: Chordoma. A
clinicopathologic study of metastasis. Am J Clin Pathol.
72:765–776. 1979.
|
|
5
|
Dahlin DC and MacCarthy CS: Chordoma.
Cancer. 5:1170–1178. 1952.
|
|
6
|
Higinbotham NL, Phillips RF, Farr HW and
Hustu HO: Chordoma. Thirty-five-year study at Memorial Hospital.
Cancer. 20:1841–1850. 1967.
|
|
7
|
Su WP, Louback JB, Gagne EJ and
Scheithauer BW: Chordoma cutis: a report of nineteen patients with
cutaneous involvement of chordoma. J Am Acad Dermatol. 29:63–66.
1993.
|
|
8
|
Unni KK: Chordoma. Dahlin’s Bone Tumors:
General Aspects and Data on 11,087 cases. 5th edition.
Lippincott-Raven; New York, NY: pp. 291–305. 1996
|
|
9
|
Gay E, Sekhar LN, Rubinstein E, Wright DC,
Sen C, Janecka IP and Snyderman CH: Chordomas and chondrosarcomas
of the cranial base: results and follow-up of 60 patients.
Neurosurgery. 36:887–897. 1995.
|
|
10
|
Hug EB, Loredo LN, Slater JD, DeVries A,
Grove RI, Schaefer RA, Rosenberg AE and Slater JM: Proton radiation
therapy for chordomas and chondrosarcomas of the skull base. J
Neurosurg. 91:432–439. 1999.
|
|
11
|
Forsyth PA, Cascino TL, Shaw EG,
Scheithauer BW, O’Fallon JR, Dozier JC and Piepgras DG:
Intracranial chordomas: a clinicopathological and prognostic study
of 51 cases. J Neurosurg. 78:741–747. 1993.
|
|
12
|
O’Connell JX, Renard LG, Liebsch NJ, et
al: Base of skull chordoma. A correlative study of histologic and
clinical features of 62 cases. Cancer. 74:2261–2267. 1994.
|
|
13
|
Zorlu F, Gürkaynak M, Yildiz F, Oge K and
Atahan IL: Conventional external radiotherapy in the management of
clivus chordomas with overt residual disease. Neurol Sci.
21:203–207. 2000.
|
|
14
|
Hruban RH, May M, Marcove RC and Huvos AG:
Lumbo-sacral chordoma with high-grade malignant cartilaginous and
spindle cell components. Am J Surg Pathol. 14:384–389. 1990.
|
|
15
|
Miettinen M, Karaharju E and Järvinen H:
Chordoma with a massive spindle-cell sarcomatous transformation. A
light- and elctron-microscopic and immunohistochemical study. Am J
Surg Pathol. 11:563–570. 1987.
|
|
16
|
Meis JM, Raymond AK, Evans HL, Charles RE
and Giraldo AA: ‘Dedifferentiated’ chordoma. A clinicopathologic
and immunohistochemical study of three cases. Am J Surg Pathol.
11:516–525. 1987.
|
|
17
|
Berven S, Zurakowski D, Mankin HJ,
Gebhardt MC, Springfield DS and Hornicek FJ: Clinical outcome in
chordoma: utility of flow cytometry in DNA determination. Spine
(Phila Pa 1976). 27:374–379. 2002.
|
|
18
|
Ikeda H, Honjo J, Sakurai H, Mitsuhashi N,
Fukuda T and Niibe H: Dedifferentiated chordoma arising in
irradiated sacral chordoma. Radiat Med. 15:109–111. 1997.
|
|
19
|
Saito A, Hasegawa T, Shimoda T, Toda G,
Hirohashi S, Tajima G and Moriya Y: Dedifferentiated chordoma: a
case report. Jpn J Clin Oncol. 28:766–771. 1998.
|