1. Introduction
Head and neck cancer is one of the 10 most common
types of cancer worldwide, afflicting >500,000 individuals each
year. Oral cancer is considered to be a preventable condition, due
to the possibility of early detection and treatment (1). Oral squamous cell carcinoma (OSCC)
represents 95% of all forms of head and neck cancer, and during the
past decade its incidence has increased by 50% (2,3). Snuff
and alcohol consumption are associated with 90% of patients that
exhibit oral cancer (1) and the two
factors appear to have a synergistic effect (4).
The majority of OSCC are diagnosed at a late phase
(5), in stages III or IV (6,7), which
markedly decreases the chances of survival and leads to a
significant deterioration in patient quality of life.
Despite the currently available therapeutic
strategies, which include the excision of malignant tissue and
combination of radiotherapy and chemotherapy, the five-year
survival rate is only 53% (3). In
addition, a high percentage of patients have a poor response to
therapy and high recurrence rates (8).
The purpose of the current review was to present the
histological and molecular characteristics of the most common type
of oral cancer encountered by dental surgeons.
2. Histology
In general, cancers, including OSCC, emerge from the
accumulation of genetic changes and epigenetic anomalies in the
signaling pathways that are associated with cancer, resulting in
phenotypes that facilitate OSCC development. This process was
summarized by Hanahan and Weinberg in ‘Hallmarks of Cancer’
(9).
OSCC is a malignant neoplasm derived from the
stratified squamous epithelium of the oral mucosa (10). Its pathogenesis is multifactorial,
associated with cigarette smoke, alcohol (11) and snuff, as well as the papilloma
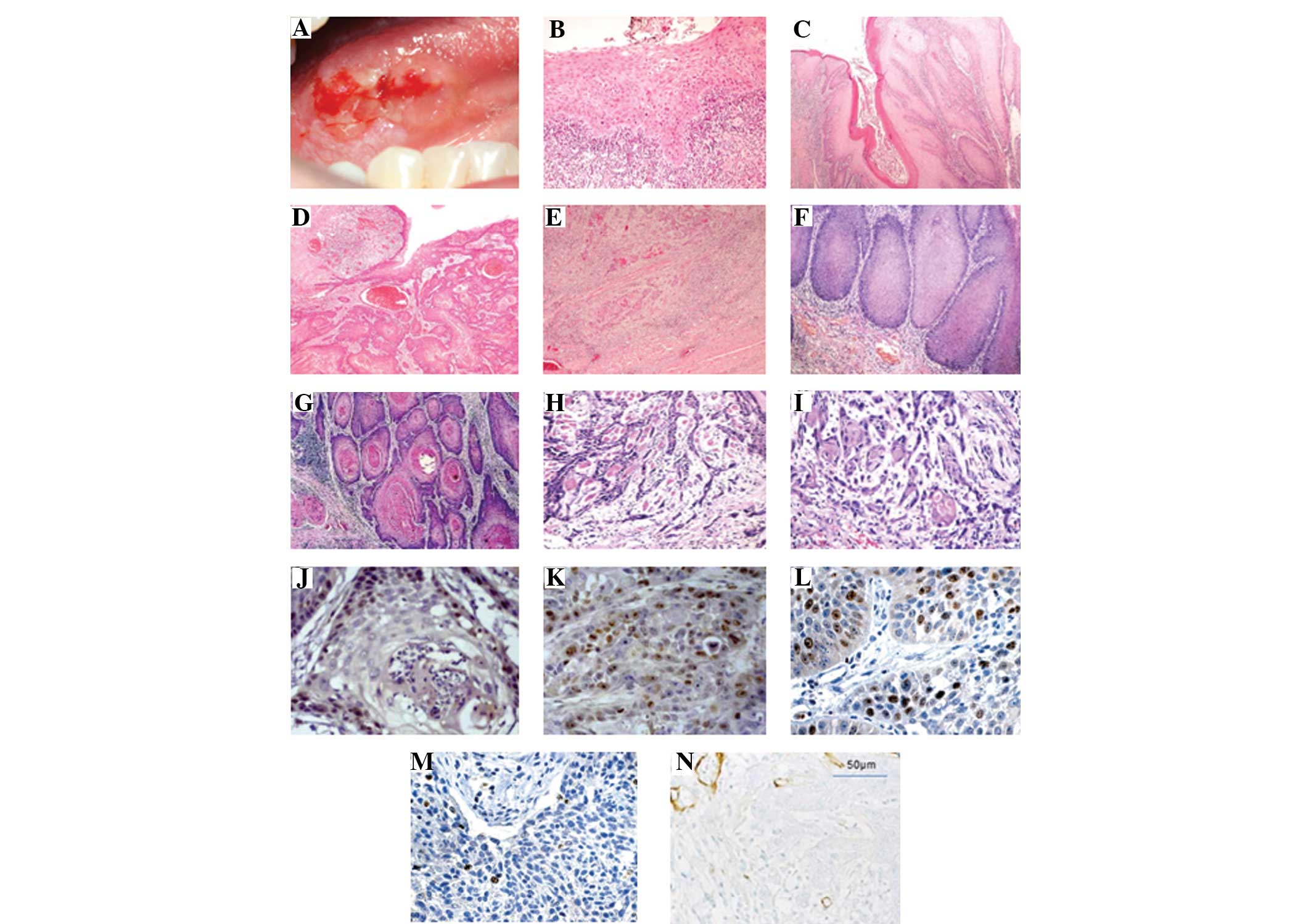
virus, among others (12). The
malignant neoplasm occurs at various sites, the most frequent being
the lip, lateral edges of the tongue (Fig. 1A) (13) and floor of the oral cavity. The
incidence of OSCC increases with age, with the majority of OSCC
occuring in patients >40 years (14).
OSCC is characterized by histopathological and
clinical manifestations. All carcinogenesis evolves from initial
cell injury to the formation of a malignant neoplasm (9). Histologically, the lesion passes
through various phases (preneoplastic damage) until the ultimate
formation of a cancer. This carcinogenesis may be associated with
precancerous lesions (such as leukoplakia, erythroplakia and
mixed). However, it is necessary to consider that not all
reactional lestions or potentially malignant lesions result in the
subsequent development of malignant neoplasms (15).
Potentially malignant changes
According to their histological appearance, lesions
that present in the epithelium during the process of carcinogenesis
may be classified according to their reactive epithelial changes
(such as hyperkeratosis, hyperplasia and acanthosis) or
preneoplastic changes (including mild, moderate and severe
dysplasia; Fig. 1B) (16) prior to the establishment of an
invasive carcinoma (12,14,17).
Oral cancer originates as an epithelial dysplasia and is
characterized by the altered proliferation of dysplastic squamous
cells on the surface of the epithelial layer, which subsequently
degrades the subepithelial basement membrane (BM). Degradation of
the BM results in local destruction and distant invasion via
metastasis. Local invasion to the underlying tissue occurs via the
islets and cords of epithelial cells (18).
The ability to metastasize is directly associated
with the differential grade of tumor cells, similar to that of the
neoplastic tissue architecture and normal epithelium (14).
International Classification of Tumors
(World Health Organization) and the tumor invasion front (TIF)
Currently, two systems are used to histologically
classify tumor lesions; the International Histological
Classification of Tumors (Fig.
1C–E) and the pattern of the TIF (19). The initial classification of lesions
is based on the degree of tumor differentiation (well-, moderately-
and undifferentiated) (20), which
is essential to evaluate the tumor’s growth rate and ability to
metastasize (14).
The TIF constitutes the area of the lesion with the
greatest depth of invasion and progression into the surrounding
tissues (21). In addition, the
cells of the TIF have differing molecular characteristics when
compared with the cells at the superficial areas of the tumor
(10,22). The TIF is considered to be the most
representative area of the tumor (23) and is identified by four
characteristics; the degree of keratinization, nuclear
polymorphism, lymphocytic infiltration and pattern of invasion (PI)
(23,24). Of these, the PI is considered to be
a good prognostic factor in OSCC (1). To evaluate the severity of the
invasion, several morphological criteria exist, associated with
certain PIs, according to the following three categories (Fig. 1F–I): i) Islet-infiltrating cells
with wide fronts of invasion; ii) thin infiltrating cords; and iii)
individual infiltrating cells (1).
In the clinical field, the majority of medical
centers base their decisions upon the clinical and pathological
information. The TNM stage (T, tumor size; N, regional lymph node
compromise; and M, metastasis) (25) and the degree of tumor
differentiation (20), combined
with the patient’s health status, are the predominant factors that
determine the therapeutic strategy. To advance the knowledge of
OSCC, numerous pathological and molecular clinical markers have
been identified for the prediction of prognosis (1).
3. Tumor biomarkers
Transformed neoplastic cells determine the
biological behavior of the tumor. Aberrant cells, which posess
common features, present a wide range of morphological and
functional disorders.
Genetic and epigenetic alterations in OSCC lead to
changes that include reduced expression or overexpression of
proteins. The accumulation of these changes in oncogenes and tumor
suppressor genes may lead to the formation of OSCC. The genes that
are critically altered in OSCC include cyclin D1, p53,
retinoblastoma, epidermal growth factor receptor, signal transducer
and activator of transcription 3, and vascular endothelial growth
factor receiver, as well as other molecules (26,27).
Ki-67 and p53
Ki-67 and p53 are the most commonly used tumor
markers for studying cell proliferation. The p53 protein is one of
the transcription factors that is implicated in cell cycle control,
apoptosis and preservation of genetic stability (28). In addition, the p53 gene is one of
the most commonly mutated genes in OSCC with mutations detected in
>50% of OSCC cases (29). The
activation of p53 has been reported in a number of processes, such
as DNA damage, hypoxia and oncogene activation. In addition, p53
protects against tumor formation by preventing the accumulation of
cells with DNA damage, which subsequently induces a loss of
function in the majority of malignant neoplasms (30). Although not completely understood,
Ki-67 is considered to be an important protein in cell division, as
it has been observed that the antigen is expressed primarily during
the cell cycle stages of G1, S, G2 and M, with a marked emphasis on
the M phase. However, Ki-67 expression is not observed during the
G0 phase and has a low expression in the G1 and S phases (31). Furthermore, Ki-67 is considered to
be one of the best predictors of survival (Fig. 1J and K) (16) and recurrence (5).
Homeobox (HOX) genes
Recently, novel markers have been used to assess
morphogenesis and cell differentiation. Previous studies have
demonstrated that the aberrant expression of genes is associated
with cancer embryogenesis, particularly the HOX genes that may
induce embryological development, as well as contribute to the
onset and progression of tumors (32,33).
Furthermore, HOX gene overexpression has been associated with
carcinogenesis, including head and neck neoplasms (34) and HOXB7, a member of the family of
homeodomain transcription factors, is a critical regulator of
development, controlling the proliferation and survival of
progenitor cells. In OSCC, HOXB7 is overexpressed (Fig. 1L and M) (32), which has been confirmed to be
associated with a poor prognosis in OSCC and other types of cancer
(32,35).
Collagen type IV (ColIV)
Infiltration is a key prerequisite for cancer
metastasis, making it a significant factor in the prognosis of
patients with OSCC (36). For the
activation of the process, degradation of the BM must occur between
the epithelium and lamina propria, which is located around the nest
of cancer cells and blood vessels. The BM has been identified as a
crucial structure in the regulation of tumor invasion. Its
molecular assembly is a barrier for the invasion of the connective
tissue, in particular of the epithelial cells, unless a molecular
rupture occurs (37).
ColIV is the most important protein component of the
BM and its integrity is altered by the degradation of the BM via
matrix metalloproteinases (MMP) 2 and 9 that are present in OSCC
(Fig. 1N) (38) and the surrounding tissues (36). Furthermore, MMP 2 and 9 facilitate
the development of lymph node metastases (38,39).
Therefore, monitoring the changes in the expression of ColIV may
have prognostic value in OSCC patients (36,40).
4. Tumor microenvironment (TME)
For a number of years, cancer has been considered a
cell-autonomous process in which consecutive mutations in the
oncogenes and tumor suppressor genes lead to the infinite
proliferation of neoplastic cells (41). Thus, cancer therapeutic strategies
have been focused and limited on such mutations within the tumor
cells (4). However, increasing
evidence indicates that the genesis and progression of the tumor is
determined by tumor cells as well as by a low TME (42).
Recent findings have indicated that for the
effective control of cancer, the genesis and progression of the
tumor must not only be considered to be cell-autonomous, but
predominantly as a disease that involves complex heterotypic
multicellular interactions within the newly formed tissue and the
original cancerous tissue. Furthermore, the disease must be
considered to be a a systemic, solid-tumor tissue disease rather
than a single disease entity. Therefore, the concept of the TME has
been proposed as an integral aspect and essential area of cancerous
tissues. Recent evidence from a study concerning the TME has
emerged, forcing the scientific community to review the basics of
cancer biology (43).
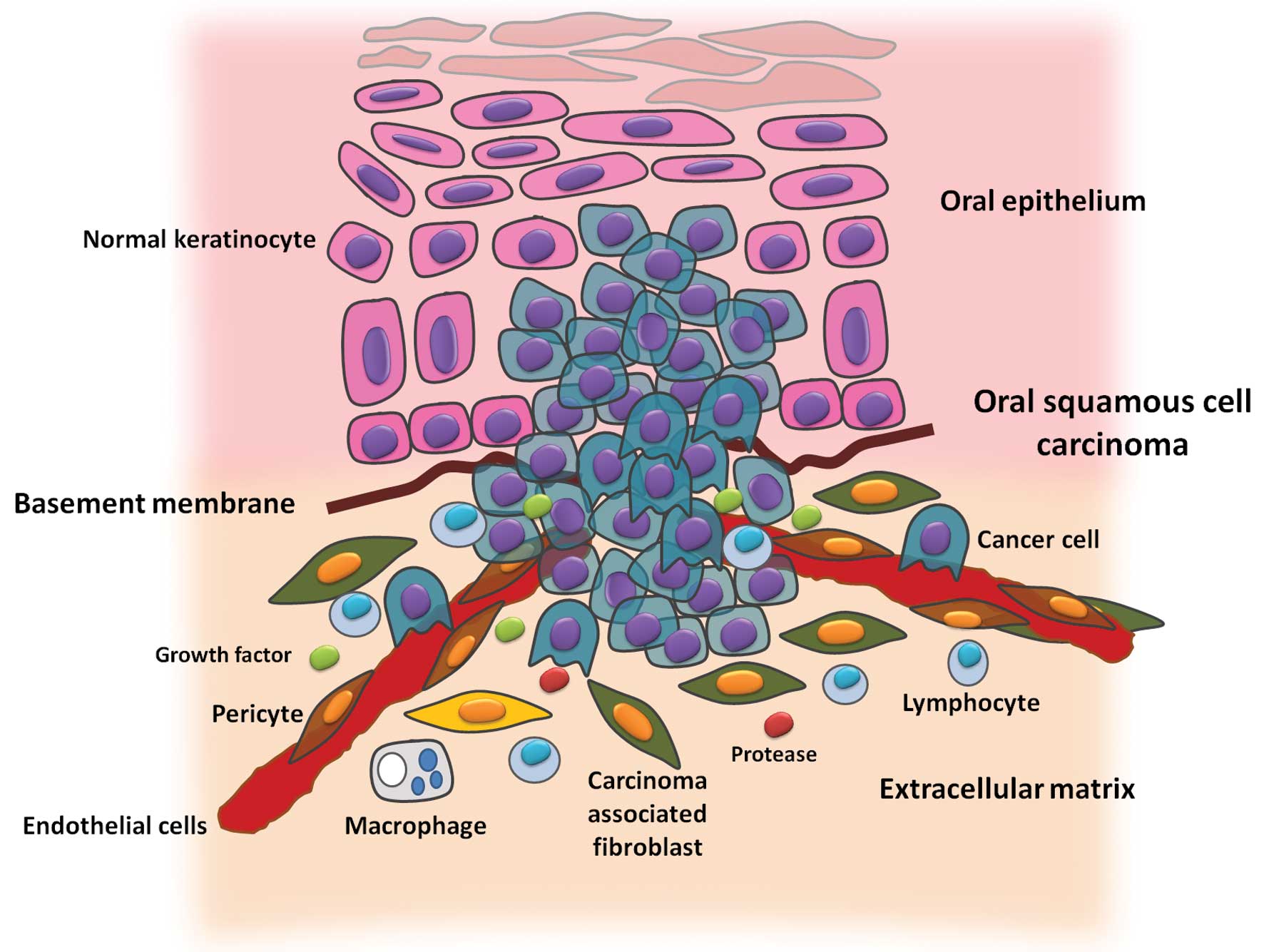
The TME contains numerous types of cells, including
fibroblasts, cancer-associated fibroblasts (CAFs), myofibroblasts,
smooth muscle cells, endothelial cells and their precursors,
pericytes, neutrophils, eosinophils, basophils, mast cells, T and B
cells, natural killer cells, and antigen presenting cells, such as
macrophages and dendritic cells (Fig.
2).
CAFs
Despite a marked recruitment of immune cells in the
TME, immune cells do not represent the main population of tumor
stromal cells; CAFs are the most abundant cells of the TME. CAFs
are generally identified by the expression of α-smooth muscle
actin, which is similar to the expression of myofibroblasts that
occurrs at the site of wound healing and chronic inflammation,
however, is absent in normal skin fibroblasts (44,45).
CAFs may be locally differentiated from normal
fibroblasts or surrounding stromal stem cells that are derived from
the mesenchymal cells of bone marrow, which is recruited by the
tumor (46). The tumor stroma is
rich in CAFs, which may be scattered or found in the tumor
periphery. Certain evidence indicates that CAFs mechanically
reshape the extracellular matrix, via the use of proteases, to
facilitate the invasion of cancer cells (4). Previous studies have also demonstrated
the existence of a molecular dialogue between CAFs and tumor cells,
the latter of which secrete interleukin 1α, which stimulates the
secretion of chemokine (CC motif) ligand 7 from the CAFs, resulting
in tumor progression (6). The
increased presence of CAFs observed in OSCC has been associated
with a diffuse invasion pattern, preparing the environment for
tumor invasion and metastasis (47), and is associated with a poor
prognosis (48).
5. Conclusion
In conclusion, an association between cell
proliferation markers in the basal lamina and connective tissue has
been identified in OSCC. In addition, hyperproliferative neoplastic
cells may induce ColIV degradation and facilitate tumor invasion.
Once installed in the connective tissue, the invading tumor cells
may stimulate fibroblasts, which results in an increase in the
presence of CAFs. This scenario may be associated with clinical and
histopathological characteristics, in terms of a more aggressive
stage of disease and a poor differentiation grade of tumor
invasion, as well as the decreased survival time of patients with
increased rates of cell proliferation, loss of BM integrity and CAF
expression within the connective tissue.
Therefore, the comparison of these factors with the
survival time of OSCC patients, from the time of histopathological
diagnosis, is of interest. The results of the present review may be
useful to clarify the tumor-stromal interaction, and its
significance regarding the clinical and histological
characteristics of OSCC, in order to expand the quantity of
specific prognostic factors available as alternatives to the
classic TNM.
Acknowledgements
The authors would like to thank the Investigations
Directorate (DI) and the Master Program of Biomedical Sciences,
University of Talca (Talca, Chile) for its cooperation.
References
|
1
|
Dissanayaka WL, Pitiyage G, Kumarasiri PV,
Liyanage RL, Dias KD and Tilakaratne WM: Clinical and
histopathologic parameters in survival of oral squamous cell
carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol. 113:518–525.
2012.
|
|
2
|
Bray F, Sankila R, Ferlay J and Parkin DM:
Estimates of cancer incidence and mortality in Europe in 1995. Eur
J Cancer. 38:99–166. 2002.
|
|
3
|
Parkin D, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108.
2005.
|
|
4
|
Koontongkaew S: The tumor microenvironment
contribution to development, growth, invasion and metastasis of
head and necksquamous cell carcinomas. J Cancer. 4:66–83. 2013.
|
|
5
|
Wangsa D, Ryott M, Avall-Lundqvist E, et
al: Ki-67 expression predicts locoregional recurrence in stage I
oral tongue carcinoma. Br J Cancer. 99:1121–1128. 2008.
|
|
6
|
Jung DW, Che ZM, Kim J, Kim K, Kim KY and
Williams D: Tumor-stromal crosstalk in invasion of oral squamous
cell carcinoma: a pivotal role of CCL7. Int J Cancer. 127:332–344.
2010.
|
|
7
|
Centelles PV, Seoane-Romero JM, Gómez I,
Diz-Dios P, de Melo NS and Seoane J: Timing of oral cancer
diagnosis: Implications for prognosis and survival. Oral Cancer.
Ogbureke KUE: InTech; pp. 173–188. 2012
|
|
8
|
Bettendorf O, Piffkò J and Bànkfalvi A:
Prognostic and predictive factors in oral squamous cell cancer:
important tools for planning individual therapy? Oral Oncol.
40:110–119. 2004.
|
|
9
|
Hanahan D and Weinberg RA: The hallmarks
of cancer. Cell. 100:57–70. 2000.
|
|
10
|
Tumuluri V, Thomas GA and Fraser IS:
Analysis of the Ki-67 antigen at the invasive tumour front of human
oral squamous cell carcinoma. J Oral Pathol Med. 31:598–604.
2002.
|
|
11
|
Wilkey JF, Buchberger G, Saucier K, et al:
Cyclin D1 overexpression increases susceptibility to
4-nitroquinoline-1 -oxide-induced dysplasia and neoplasia in murine
squamous oral epithelium. Mol Carcinog. 48:853–861. 2009.
|
|
12
|
Neville B, Damm D, Allen C and Bouquot J:
Oral and Maxillofacial Pathology. 3rd edition. Saunders Elsevier;
Philadelphia, PA: pp. 356–367. 2009
|
|
13
|
Jerjes W, Upile T, Petrie A, et al:
Clinicopathological parameters, recurrence, locoregional and
distant metastasis in 115 T1–T2 oral squamous cell carcinoma
patients. Head Neck Oncol. 2:92010.
|
|
14
|
Sapp JP, Eversole LR and Wysocki GP:
Contemporary Oral and Maxillofacial Pathology Chapter 6: Epithelial
Disorders. 2nd edition. Mosby Year Book Inc; Maryland Heights, MO:
pp. 184–193. 2004
|
|
15
|
Neville BW and Day TA: Oral cancer and
precancerous lesions. CA Cancer J Clin. 52:195–215. 2002.
|
|
16
|
Wang Z, Zhang B, Jiang L, et al: RACK1, an
excellent predictor for poor clinical outcome in oral squamous
carcinoma, similar to Ki67. Eur J Cancer. 45:490–496. 2009.
|
|
17
|
Rivera MCA: 4NQO carcinogenesis: A model
of oral squamous cell carcinoma. Int J Morphol. 30:309–314.
2012.
|
|
18
|
Fuentes B, Duaso J, Droguett D, et al:
Progressive extracellular matrix disorganization in chemically
induced murine oral squamous cell carcinoma. ISRN Pathology.
2012.
|
|
19
|
Rivera CA, Droguett DA, Kemmerling U and
Venegas BA: Chronic restraint stress in oral squamous cell
carcinoma. J Dent Res. 90:799–803. 2011.
|
|
20
|
Pindborg JJ, Reichart PA, Smith CJ and Van
der Waal I: WHO International Histological Classification of
Tumours Histological typing of cancer and precancer of the oral
mucosa. Springer-Verlag; New York: 1997
|
|
21
|
Wang X, Zhang J, Fan M, et al: The
expression of E-cadherin at the invasive tumor front of oral
squamous cell carcinoma: immunohistochemical and RT-PCR analysis
with clinicopathological correlation. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod. 107:547–554. 2009.
|
|
22
|
Bànkfalvi A and Piffkò J: Prognostic and
predictive factors in oral cancer: the role of the invasive tumour
front. J Oral Pathol Med. 29:291–298. 2000.
|
|
23
|
Kurokawa H, Zhang M, Matsumoto S, et al:
The high prognostic value of the histologic grade at the deep
invasive front of tongue squamous cell carcinoma. J Oral Pathol
Med. 34:329–333. 2005.
|
|
24
|
Bryne M, Koppang HS, Lilleng R and
Kjaerheim A: Malignancy grading of the deep invasive margins of
oral squamous cell carcinomas has high prognostic value. J Pathol.
166:375–381. 2005.
|
|
25
|
Oliveira L, Ribeiro-Silva A, Costa J,
Simões A, Matteo M and Zucoloto S: Prognostic factors and survival
analysis in a sample of oral squamous cell carcinoma patients. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod. 106:685–695. 2008.
|
|
26
|
Leemans CR, Braakhuis BJ and Brakenhoff
RH: The molecular biology of head and neck cancer. Nat Rev Cancer.
11:9–22. 2010.
|
|
27
|
Choi S and Myers J: Molecular pathogenesis
of oral squamous cell carcinoma: implications for therapy. J Dent
Res. 87:14–32. 2008.
|
|
28
|
Massano J, Regateiro F, Januário G and
Ferreira A: Oral squamous cell carcinoma: review of prognostic and
predictive factors. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 102:67–76. 2006.
|
|
29
|
van Houten VM, Tabor MP, van den Brekel
MW, et al: Mutated p53 as a molecular marker for the diagnosis of
head and neck cancer. J Pathol. 198:476–486. 2002.
|
|
30
|
Maddocks OD and Vousden KH: Metabolic
regulation by p53. J Mol Med (Berl). 89:237–245. 2011.
|
|
31
|
Yerushalmi R, Woods R, Ravdin PM, Hayes M
and Gelmon KA: Ki-67 in breast cancer: prognostic and predictive
potential. Lancet Oncol. 11:1742010.
|
|
32
|
Bitu CC, Carrera M, Lopes MA, Kowalski LP,
Soares FA and Coletta RD: HOXB7 expression is a prognostic factor
for oral squamous cell carcinoma. Histopathology. 60:662–665.
2012.
|
|
33
|
Shah N and Sukumar S: The Hox genes and
their roles in oncogenesis. Nat Rev Cancer. 10:361–371. 2010.
|
|
34
|
Tucci R, Campos MS, Matizonkas-Antonio LF,
Durazzo M, dos Pinto Junior DS and Nunes FD: HOXB5 expression in
oral squamous cell carcinoma. J Appl Oral Sci. 19:125–129.
2011.
|
|
35
|
Liao WT, Jiang D, Yuan J, et al: HOXB7 as
a prognostic factor and mediator of colorectal cancer progression.
Clin Cancer Res. 17:3569–3578. 2011.
|
|
36
|
Fan HX, Li HX, Chen D, Gao ZX and Zheng
JH: Changes in the expression of MMP2, MMP9, and ColIV in stromal
cells in oral squamous tongue cell carcinoma: relationships and
prognostic implications. J Exp Clin Cancer Res. 31:902012.
|
|
37
|
Kumar V, Abbas AK and Aster JC: Robbins
Basic Pathology Chapter 7: Neoplasia. 8th ed. Saunders;
Philadelphia, PA: pp. 298–299. 2012
|
|
38
|
Tamamura R, Nagatsuka H, Siar CH, et al:
Comparative analysis of basal lamina type IV collagen alpha chains,
matrix metalloproteinases-2 and −9 expressions in oral dysplasia
and invasive carcinoma. Acta Histochem. 115:113–119. 2013.
|
|
39
|
de Vicente JC, Fresno MF, Villalain L,
Vega JA and Hernández Vallejo G: Expression and clinical
significance of matrix metalloproteinase-2 and matrix
metalloproteinase-9 in oral squamous cell carcinoma. Oral Oncol.
41:283–293. 2005.
|
|
40
|
Baba Y, Iyama K, Ikeda K, et al: The
Expression of type IV collagen α6 chain is related to the prognosis
in patients with esophageal squamous cell carcinoma. Ann Surg
Oncol. 15:555–565. 2008.
|
|
41
|
Kenny PA, Lee GY and Bissell MJ: Targeting
the tumor microenvironment. Front Biosci. 12:3468–3474. 2007.
|
|
42
|
Zhang J and Liu J: Tumor stroma as targets
for cancer therapy. Pharmacol Ther. 137:200–215. 2013.
|
|
43
|
Liotta LA and Kohn EC: The
microenvironment of the tumour-host interface. Nature. 411:375–379.
2001.
|
|
44
|
Shimoda M, Mellody KT and Orimo A:
Carcinoma-associated fibroblasts are a rate-limiting determinant
for tumour progression. Semin Cell Dev Biol. 21:19–25. 2010.
|
|
45
|
Räsänen K and Vaheri A: Activation of
fibroblasts in cancer stroma. Exp Cell Res. 316:2713–2722.
2010.
|
|
46
|
Xouri G and Christian S: Origin and
function of tumor stroma fibroblasts. Semin Cell Dev Biol.
21:40–46. 2010.
|
|
47
|
de-Assis EM, Pimenta LG, Costa-e-Silva E,
Souza PE and Horta MC: Stromal myofibroblasts in oral leukoplakia
and oral squamous cell carcinoma. Med Oral Patol Oral Cir Bucal.
17:e733–e738. 2012.
|
|
48
|
Thode C, Jørgensen TG, Dabelsteen E,
Mackenzie I and Dabelsteen S: Significance of myofibroblasts in
oral squamous cell carcinoma. J Oral Pathol Med. 40:201–207.
2011.
|