Introduction
Neurogenic tumors are the most common type of
mediastinal tumor and constitute the majority of neoplasms of the
posterior mediastinum (1).
Neurogenic tumors derive from the cells of the nerve sheath or from
the ganglionic cells of the spinal ganglia and of the autonomic,
paraganglionic and parasympathetic systems (2). Schwannoma is a type of benign nerve
sheath tumour which is ofen located in the head, neck and
extremities, and mostly asymptomatic. However, occasionally
schwannoma may present with symptoms of compression of the
neighboring structures. The treatment of choice is surgical
excision, with good prognosis. However, schwannoma, which arises
from the intrathoracic vagus nerve, is rare. The present study
describes a rare case of a vagal schwannoma in the left superior
mediastinum, which was resected en bloc using video-assisted
thoracoscopic surgery (VATS). The patient provided written informed
consent.
Case report
Case presentation
A 58-year old male presented with chest pain and
hoarseness for two months. The patient denied symptoms, including
fever, dyspnea, palpitation, hemoptysis, dysphagia and muscle
weakness. The patient’s past medical history was not significant.
Physical examination and laboratory test results showed no
significant abnormalities, including those in carcinoembryonic
antigen, α-fetoprotein and prostate specific antigen levels. A
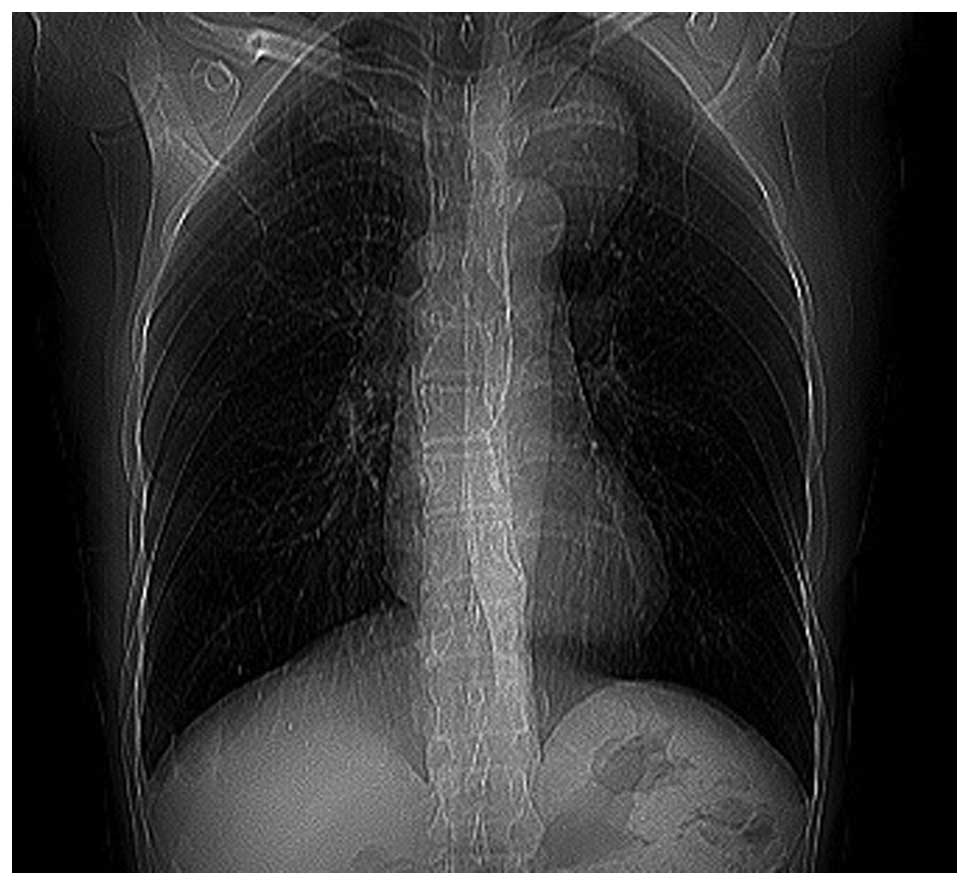
chest roentgenogram revealed a well-defined mass located at the
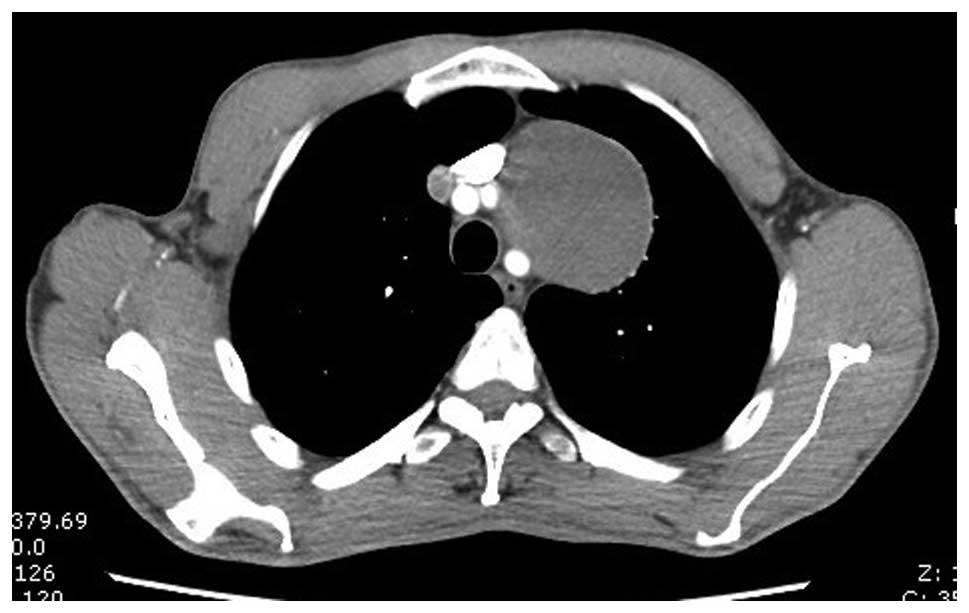
left superior lung field, protruding from the mediastinum (Fig. 1). Contrast-enhanced computed
tomography of the chest showed a sharply demarcated, circumscribed
mass, ~78×66×59 mm in size, in the left superior mediastinum
(Fig. 2).
Surgery and histological analysis
The patient underwent left-sided VATS.
Intraoperatively, a large tumor with a round shape was identified
in the left superior mediastinum. The left phregnic nerve crossed
the surface of the mass and the tumor was originating from, and
encasing, the vagus nerve (Fig. 3).
The mass was located at the anterior and superior to the aortic
arch, and was attached to the left subclavian artery, left common
carotid artery, left innominate vein and superior vena cava. The
tumor was completely excised through amputation of the vagus nerve
encased in the mass. Grossly, the mass had a complete envelop and
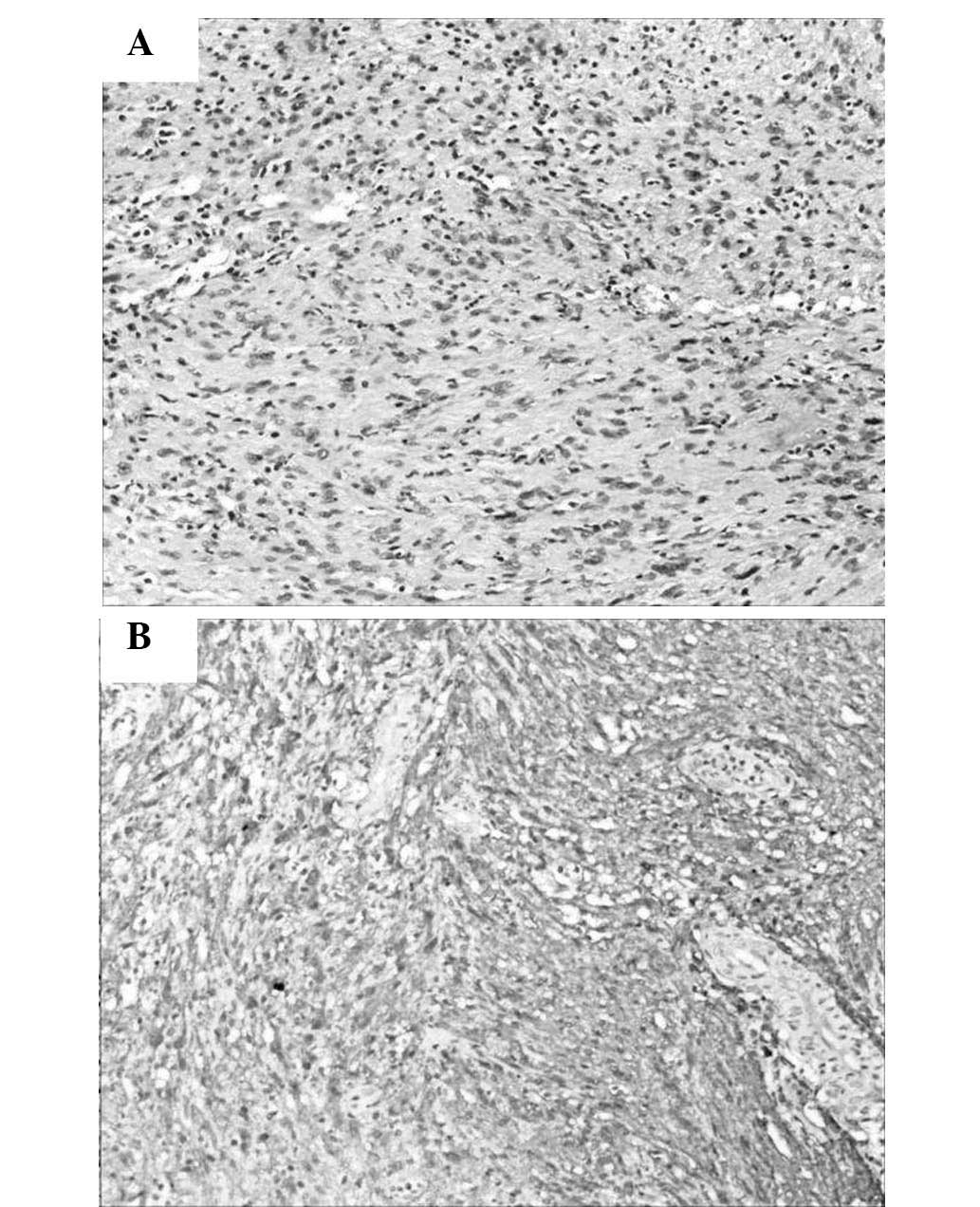
contained dark-colored hydatid fluid. Histologically, the tumor
contained spindle cells with strong positivity for S-100 protein
and was diagnosed as schwannoma of the vagus nerve (Fig. 4).
Follow-up
The patient’s postoperative recovery was uneventful
and the patient was discharged on the seventh postoperative day.
The patient was followed up at six month intervals for 18 months.
At the one-year follow-up, the patient was tumor- and symptom-free,
but presented with hoarseness.
Discussion
Schwannoma, also termed neurilemmoma, is a type of
benign nerve sheath tumor arising from Schwann cells. It is the
most common neurogenic tumor of the chest and approximately 10% of
schwannomas originate from the vagus nerve (3–5). In
1935, Stout (6) first designated
vagal tumors of nerve sheath origin as ‘neurilemmomas’. The tumor
may occur at all ages and does not show a gender preference.
Schwannoma is asymptomatic in the majority of cases; however, a
number of symptoms, including chest pain, dysphagia, coughing and
hoarseness, to varying degrees, may occur due to compression of the
neighboring organs (7,8). Hoarseness may occur when the tumor is
influenced by the recurrent laryngeal nerve, as was shown in the
present case. Schwannomas of the vagus nerve are almost twice as
likely to be located on the left than on the right, as the
recurrent laryngeal nerve arises lower in the thoracic cavity on
the left side and the left nerve trunk is thicker (1,8–11).
Surgical resection is recommended for mediastinal
neurogenic tumors and thoracoscopic surgery is preferred due to its
less invasive nature, which is beneficial when resecting sharply
marginated masses, as in the present case. Although certain studies
have proposed that VATS was contraindicated in tumors larger than 6
cm (9,10), Yamaguchi et al (12) reported that VATS was capable of
excising a neurogenic tumor of the thorax as large as 7 cm in
diameter, with no complications. In the present case, the tumor was
large and attached to the great vessels; however, it was partly
cystic and the tumor was resected using VATS with tumor incision
and hydatid fluid outflow. When the tumor encased the vagal nerve,
enucleation of the schwannoma from the vagal nerve is difficult and
amputation of the nerve is unavoidable with sacrifice of the
recurrent laryngeal nerve branch, as was shown in the present case.
The patient should be closely observed for cardiac rhythm
abnormalities, as severe bradycardia or asystole may develop during
removal of the tumor (13,14).
The specific diagnosis of schwannoma requires
pathological examination. In the present case, microscopic
examination revealed spindle cells in fascicles in a loose stroma.
If atypia, mitoses, pleomorphism and necrosis are identified,
malignant schwannoma should be considered in the diagnosis,
although they are extremely rare (4).
The prognosis of schwannoma of the vagus nerve
following complete resection of the tumor appears to be
satisfactory. The patient described in the present case was free of
recurrence with no symptoms at the one-year follow-up; however,
long-term survival should be assessed.
References
|
1
|
Singer RL: Thoracoscopic excision of a
malignant schwannoma of the intrathoracic vagus nerve. Ann Thorac
Surg. 59:1586–1587. 1995.
|
|
2
|
Shields TW and Reynolds M: Neurogenic
tumor of the thorax. Surg Clin North Am. 68:645–668. 1988.
|
|
3
|
Reed JC, Hallet KK and Feigin DS: Neural
tumors of the thorax: subject review from the AFIP. Radiology.
126:9–17. 1978.
|
|
4
|
Rammos KS, Rammos SK, Foroulis CN and
Zaramboukas TK: Schwannoma of the vagus nerve, a rare middle
mediastinal neurogenic tumor: case report. J Cardiothorac Surg.
4:682009.
|
|
5
|
Biswas D, Marnane CN, Mal R and Baldwin D:
Extracranial head and neck schwannomas - a 10-year review. Auris
Nasus Larynx. 34:353–359. 2007.
|
|
6
|
Stout AP: The peripheral manifestations of
the specific nerve sheath tumor (neurilemmoma). Cancer Res.
24:751–780. 1935.
|
|
7
|
Mallios DI, Krassas A, Kakaris S and
Sepsas E: Compression of the trachea by intrathoracic vagus nerve
schwannoma. Asian Cardiovasc Thorac Ann. 20:862012.
|
|
8
|
Shirakusa T, Tsutsui M, Montonaga R,
Takata S, Yoshomine K, Kondo K and Yoshida T: Intrathoracic tumors
arising from the vagus nerve. Review of resected tumors in Japan.
Scand J Thorac Cardiovasc Surg. 23:173–175. 1989.
|
|
9
|
Menal Muñoz P, García Tirado FJ and Rivas
de Andrés JJ: Intrathoracic vagal nerve schwannoma. Arch
Bronconeumol. 47:374–375. 2011.(In English and Spanish).
|
|
10
|
Huang TW, Yang MH, Cheng YL, Tsai WC and
Lee SC: Vagus nerve schwannoma in the middle mediastinum. Thorac
Cardiovasc Surg. 58:312–314. 2010.
|
|
11
|
Strickland B and Wolverson MK:
Intrathoracic vagus nerve tumours. Thorax. 29:215–222. 1974.
|
|
12
|
Yamaguchi M, Yoshino I, Fukuyama S,
Osoegawa A, Kameyama T, Tagawa T and Maehara Y: Surgical treatment
of neurogenic tumors of the chest. Ann Thorac Cardiovasc Surg.
10:148–151. 2004.
|
|
13
|
Wood BM and McNeil WT: Schwannoma of the
vagus nerve. Anaesthesia. 41:1130–1132. 1986.
|
|
14
|
Mukherjee DK: Neurilemmoma of the vagus
nerve: a case report. J Laryngol Otol. 93:187–192. 1979.
|