Introduction
Primary intraosseous liposarcoma is a rare and
malignant type of skeletal system tumor; the first case was
reported in 1931 by Stewart (1).
Primary intraosseous liposarcoma originate from the intraosseous
adipose tissue. Since 1980, only a small number of cases of primary
liposarcoma involving a long bone have been described in the
English literature. Recently, a patient exhibiting dedifferentiated
liposarcoma presented at the Southwest Hospital (Chongqing, China),
and all of the radiographic, clinical and pathologic evidence
indicated a primary bone origin. The purpose of the present report
is to increase awareness of this uncommon type of malignant tumor
through the description of the clinical, surgical, radiographic and
pathologic findings observed in this particular patient. Patient
provided written informed consent.
Case report
A 26-year-old male presented at the Department of
Orthopedic Surgery, Southwest Hospital, complaining of a dull
intermittent pain, for three months, along the anterolateral aspect
of the right knee. The pain was relieved by taking
Celebrex®, however, it was exacerbated by activity. The
patient had identified a slow-growing mass on the outside of the
right lower thigh and, a month prior to admission, the patient had
noted a moderate sensation of warmth in this region. There was no
history of accident, injury, fever, weakness or weight-loss. The
patient visited another hospital in April 2012 and radiographs
demonstrated a tumorous lesion in the right distal femur. The
patient was referred to the Southwest Hospital in May 2012 with an
unremarkable medical history. However, the physical examination was
notable due to swelling, a decreased range of motion of the right
knee and a palpable mass (size, ~5×4×3 cm). The laboratory
assessments of the patient’s alkaline phosphatase levels were
unremarkable. The radiographs revealed an expansile and osteolytic
lesion of the right distal femur with a periosteal reaction
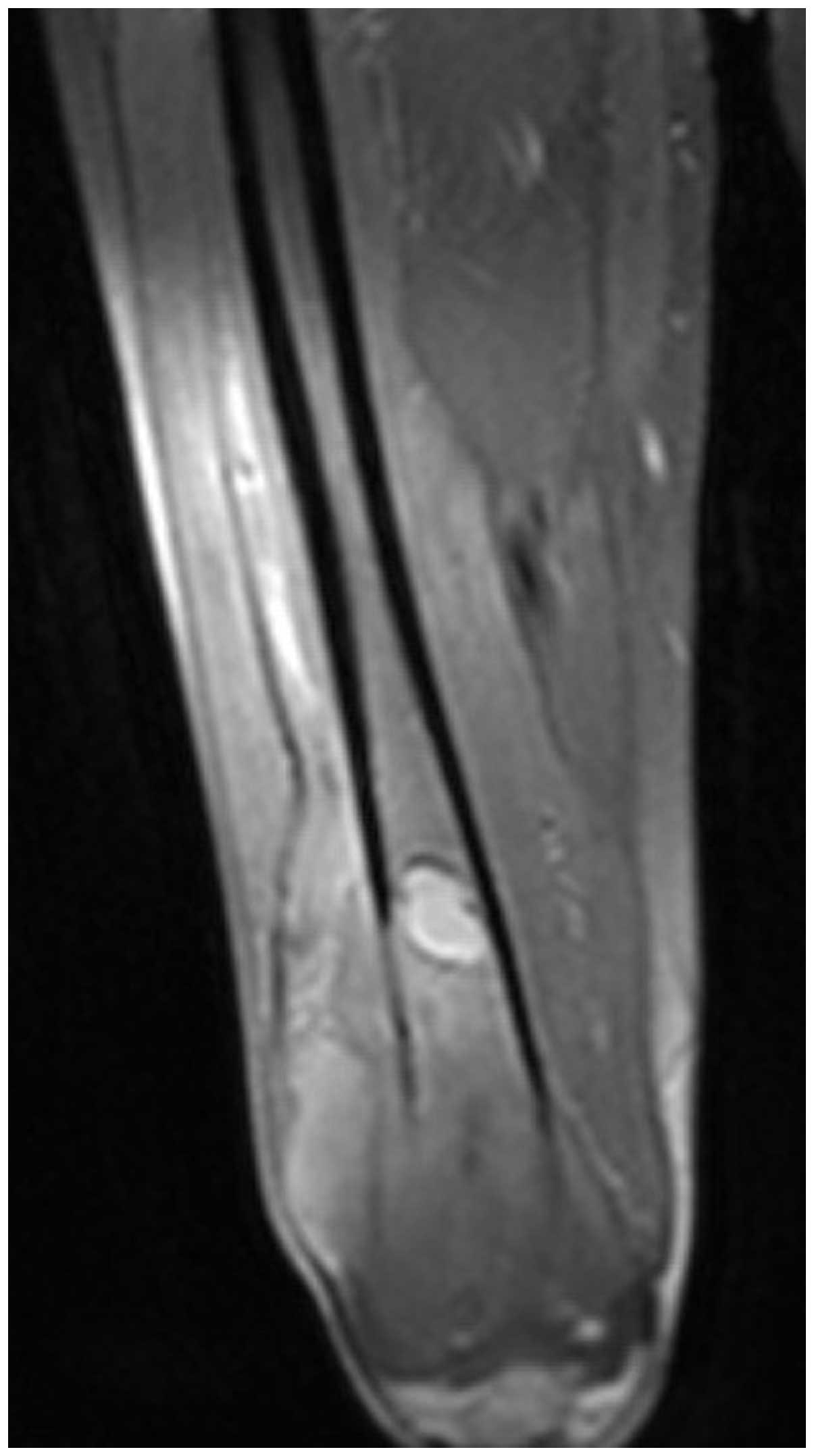
(Fig. 1). Magnetic resonance
imaging demonstrated an expansile, intramedullary, poorly defined
neoplasm with a moderately high signal intensity area on T1- and
T2-weighted images in the distal part of the femur, with diffuse
erosion of the cortex and involvement of the surrounding soft
tissue (Fig. 2). The intraosseous
central location and uniform cortical destruction indicated that
the lesion was not a soft-tissue sarcoma, which are associated with
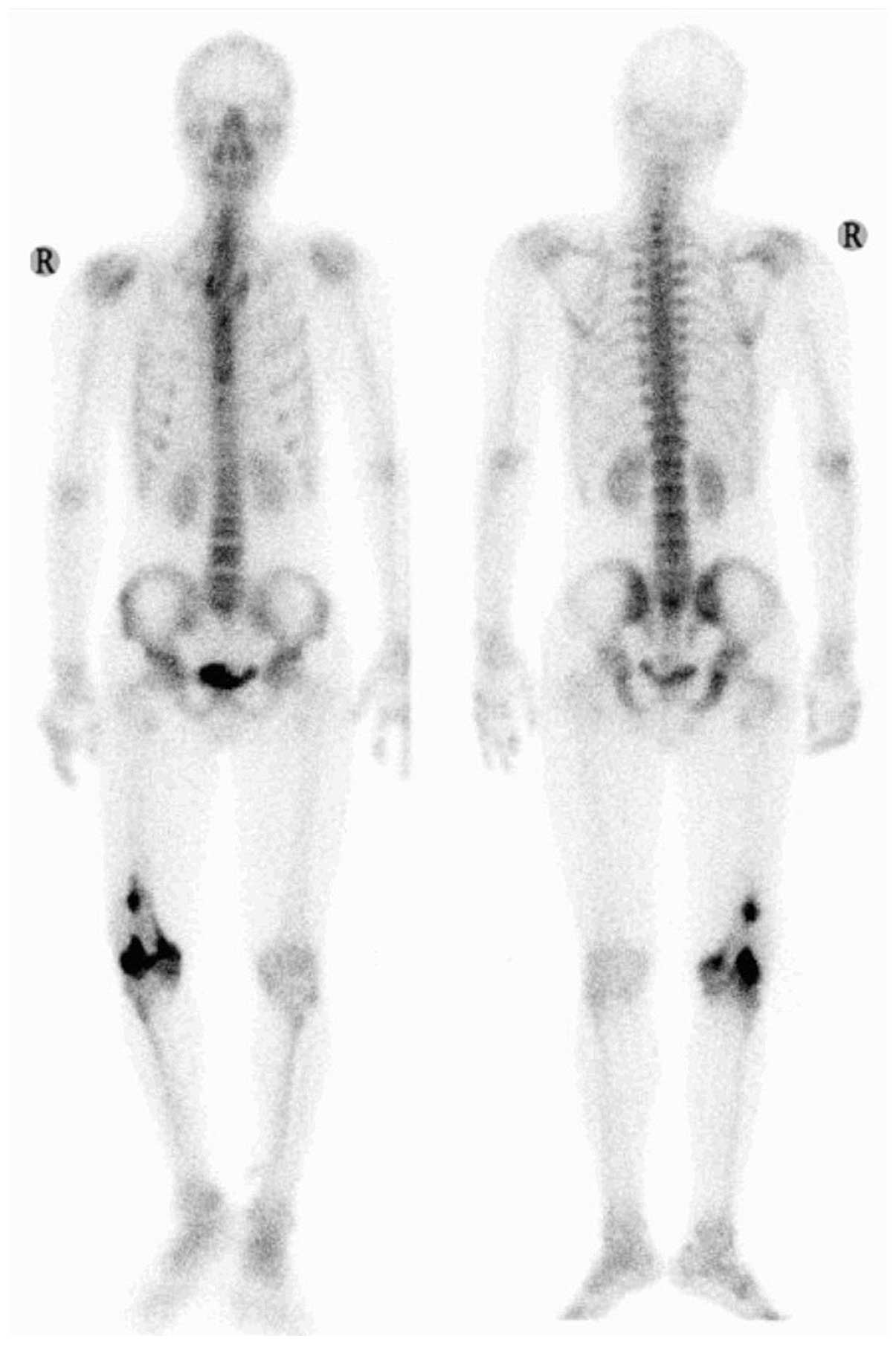
bone invasion. An emission computed tomography (CT) bone scan
demonstrated an abnormal isolated concentration of radioactive
agent (used for bone imaging) at the femoral site, which revealed
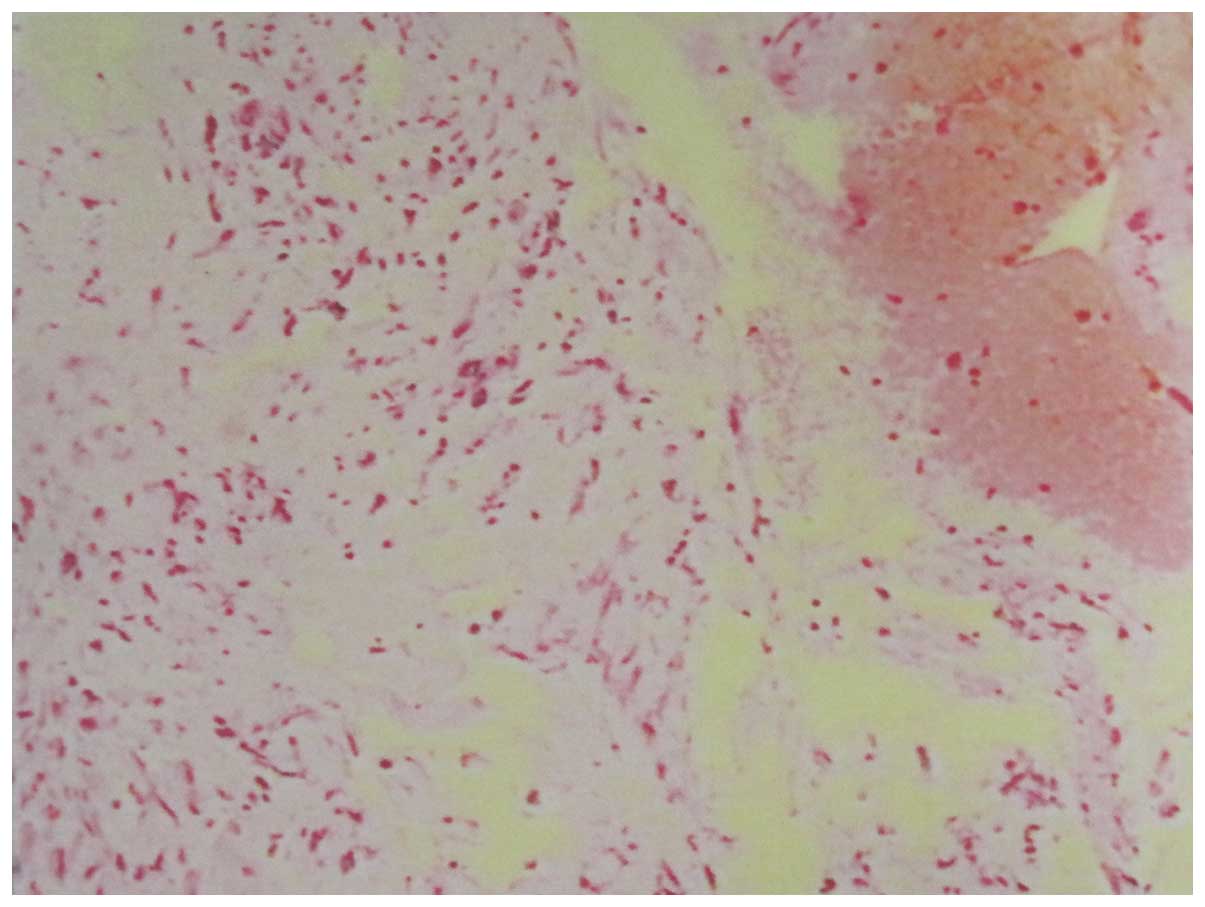
that no distant metastases had occurred (Fig. 3). Chest CT did not demonstrate any
thoracic abnormality and the CT-guided biopsy results showed blood
clots as well as a small quantity of heterogeneous cells (Fig. 4). Therefore, the clinical diagnosis
was a malignant bone tumor, with the most likely diagnosis
considered to be an osteosarcoma, as a primary bone tumor.
A limb-salvage procedure, involving a wide resection
and a total knee endoprosthesis replacement, was performed in May
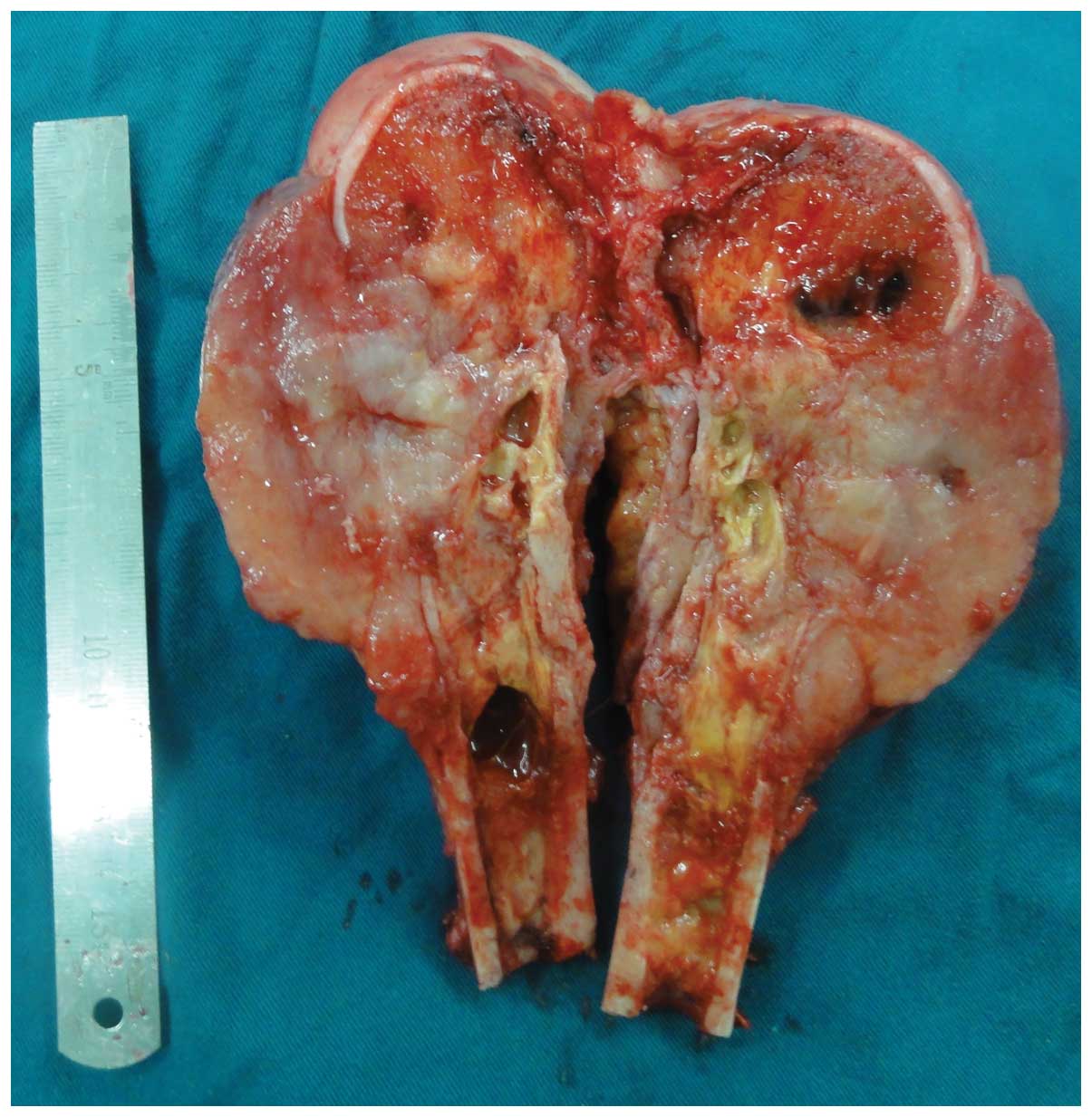
2012. Examination of the resection specimen showed a soft,
light-yellow (or gray), gelatinous tumor measuring 13 cm along the
long axis of the femur and 6 cm transversely. The tumor was
centered in the distal part of the femur, with involvement of the
surrounding soft tissues. A central hemorrhagic and necrotic area
contained serosanguineous fluid, with an abundant local blood
supply (Fig. 5). No intra-articular
extension was observed and there was no indication of regional
metastasis on dissection of the popliteal fossa lymph nodes. The
patient’s postoperative course was uneventful.
Microscopically, the tumor was identified as a
sarcoma, which demonstrated ovoid and polygonal tumor cells that
were of diffuse distribution with obvious atypia and mitotic
figures. In addition, a combination of numerous giant tumor cells
and fatty tissue with different degrees of differentiation was
observed (Fig. 6).
Immunohistochemistry showed positive staining for S-100 protein and
cluster of differentiation (CD)68, and negative staining for smooth
muscle actin, CD34 and vimentin. The final pathological diagnosis
was a primary dedifferentiated liposarcoma of the femur, and the
dedifferentiated tissue was identified as malignant fibrous
histiocytoma.
No other types of therapy, including chemotherapy
and radiation, were selected prior to and following surgery. The
patient was followed up for 12 months after surgery, and no
recurrence and metastasis was detected. In addition, radiography
indicated that the artificial joint was in good condition.
Discussion
Liposarcoma is a common type of sarcoma that affects
the soft tissues, however, primary intraosseous liposarcomas are
particularly rare (2) with only 10
cases described in previous reports since 1980 (Table I) (3–12). To
the best of our knowledge, no cases of primary dedifferentiated
liposarcoma of the bone have been reported.
 | Table IPrimary liposarcoma of various bones
as reported in the English literature since 1980. |
Table I
Primary liposarcoma of various bones
as reported in the English literature since 1980.
| First author
(Ref.) | Year | Age
(years)/Gender | Site | Subtype | Treatment | Metastasis | Outcome (months) |
|---|
| Schneider (3) | 1980 | 69/M | Fibula | Unknown | Amputation | (-) | Unknown (24) |
| Bolen (4) | 1981 | 39/M | Humerus | Pleomorphic | Humeroscapular
disarticulation | (-) | Unknown |
| Addison (5) | 1982 | 19/M | Humerus | Pleomorphic | Amputation,
radiation, chemotherapy | Lung | Succumbed (10) |
| Torok (6) | 1983 | 34/M | Femur | Pleomorphic | Wide resection,
radiation, chemotherapy | Lung | Succumbed (16) |
| Kenan (7) | 1991 | 57/M | Scapula | Myxoid | Curettage | Supra-clavicular | Alive (36) |
| Rabah (8) | 1999 | 16/F | Humerus | Pleomorphic | Chemotherapy, limb
salvage procedure | Liver | Succumbed (70) |
| Hamlat (9) | 2005 | 45/F | Thoracic | Pleomorphic | Radiation, vertebrae
decompressive laminectomy resection, endoporosthesis
replacement | Lung, rib | Alive (6) |
| Torigoe (10) | 2006 | 38/F | Humerus | Pleomorphic | Chemotherapy | Liver | Succumbed (7) |
| Seo (11) | 2007 | 69/M | Temporal bone | Well-
differentiated | Palliative
resection | (-) | Alive (24) |
| Lmejjati (12) | 2008 | 45/M | Lumbar vertebrae | Pleomorphic | Decompressive
laminectomy, novel adjuvant chemotherapy, limb salvage | Unknown | Succumbed (3) |
Table I indicates
that the long bone is most commonly affected by liposarcoma,
particularly in the humerus and there has only been one case where
the lesion occurred in the femur. As with other malignant tumors of
the bone, patients present with a history of pain, swelling,
decreased range of motion, and an expansile and osteolytic lesion
as demonstrated by radiographs. Clinically, it is possible to
mistake a primary intraosseous liposarcoma for an osteosarcoma,
Ewing’s sarcoma, plasmacytoma or a lymphoma. Primary intraosseous
liposarcoma can only definitively be diagnosed by pathological
methods. The initial observations of the biological behavior of the
lesion, the imageology data and past experience indicated that the
present case was exhibiting an osteosarcoma. However, the final
pathological diagnosis following surgery was a dedifferentiated
liposarcoma.
Due to the limited quantity of previous cases and
the various treatment modalities that were used, there is no
definitive standard treatment for primary intraosseous liposarcoma
and it is difficult to formulate an effective treatment protocol.
Surgical resection remains the primary treatment method. To reduce
recurrence, Mouret (13) proposed
that during complete resection of liposarcoma a margin around the
lesion of ≥2 cm is required, as satellite nodules are occasionally
present within this margin. However, complete resection may be
difficult in certain regions, for example the head and neck, due to
the presence of critical organs. Chemotherapy is another treatment
modality selected by certain clinicians rather than surgery.
Although the first case in 1982 reported the use of chemotherapy as
the treatment strategy (5), a total
of five cases have been reported (5,6,8,10,12),
where combined-treatment chemotherapy was adopted; the survival
times for these patients were 10, 16, 70, 7 and 3 months,
respectively. In 1999, Rabah et al (8) reported the case of a patient with a
liposarcoma of the humerus. The patient was systematically
administered with adjuvant chemotherapy, which comprised of four
cycles of cisplatin, doxorubicin and ifosfamide prior to surgery,
and continued for five further cycles following surgery. The
patient survival time of 70 months was the longest. Thus,
chemotherapy may be an additional optional adjuvant treatment.
Liposarcoma is commonly classified into five
pathological categories, as follows: Well-differentiated;
dedifferentiated; round cell; myxoid; and pleomorphic (14). The histological classification is
important for treating liposarcoma, as the clinical features and
prognosis are dependent on it. Enzinger and Weiss (14) reported that the five-year survival
rate of patients with well-differentiated liposarcoma is ~90%,
while that of patients with the myxoid type is ~80%, pleomorphic
type is ~20% and the round cell type is <20%. There is no
five-year survival rate for the dedifferentiated type, as few cases
have been reported.
In conclusion, based on Table I, it is apparent that the majority
of patients with primary intraosseous liposarcoma succumb to this
metastatic disease, with the common metastatic site being the
lungs, indicating that this type of tumor is associated with a poor
prognosis. Therefore, careful observation during follow-up is
recommended to ensure the early detection of recurrence and distant
metastasis. The patient in the present study returned for follow-up
one year following surgery, and no recurrence and metastasis was
detected. To the best of our knowledge, this is the first report to
present a case of dedifferentiated primary liposarcoma of the
bone.
References
|
1
|
Stewart FW: Primary liposarcoma of bone.
Am J Pathol. 7:87–94. 1931.
|
|
2
|
Downey EF Jr, Worsham GF and Brower AC:
Liposarcoma of bone with osteosarcomatous foci: case report and
review of the literature. Skeletal Radiol. 8:47–50. 1982.
|
|
3
|
Schneider HM, Wunderlich T and Puls P: The
primary liposarcoma of the bone. Arch Orthop Trauma Surg.
96:235–239. 1980.
|
|
4
|
Bolen JW and Thorning D: Liposarcomas. A
histogenetic approach to the classification of adipose tissue
neoplasms. Am J Surg Pathol. 8:3–17. 1984.
|
|
5
|
Addison AK and Payne SR: Primary
liposarcoma of bone. Case report. J Bone Joint Surg Am. 64:301–304.
1982.
|
|
6
|
Torok G, Meller Y and Maor E: Primary
liposarcoma of bone. Case report and review of the literature. Bull
Hosp Jt Dis Orthop Inst. 43:28–37. 1983.
|
|
7
|
Kenan S, Lewis MM, Abdelwahab IF, Hermann
G and Klein MJ: Case report 652: Primary intraosseous low grade
myxoid sarcoma of the scapula (myxoid liposarcoma). Skeletal
Radiol. 20:73–75. 1991.
|
|
8
|
Rabah R, Lucas DR, Farmer DL, Ryan JR and
Ravindranath Y: Primary liposarcoma of bone in an adolescent - A
case report. Int J Surg Pathol. 7:45–51. 1999.
|
|
9
|
Hamlat A, Saikali S, Gueye EM, Le Strat A,
Carsin-Nicol B and Brassier G: Primary liposarcoma of the thoracic
spine: case report. Eur Spine J. 14:613–618. 2005.
|
|
10
|
Torigoe T, Matsumoto T, Terakado A, Takase
M, Yamasaki S and Kurosawa H: Primary pleomorphic liposarcoma of
bone: MRI findings and review of the literature. Skeletal Radiol.
35:536–538. 2006.
|
|
11
|
Seo T, Nagareda T, Shimano K, Saka N,
Kashiba K, Mori T and Sakagami M: Liposarcoma of temporal bone: a
case report. Auris Nasus Larynx. 34:511–513. 2007.
|
|
12
|
Lmejjati M, Loqa C, Haddi M, Hakkou M and
BenAli SA: Primary liposarcoma of the lumbar spine. Joint Bone
Spine. 75:482–485. 2008.
|
|
13
|
Mouret P: Liposarcoma of the hypopharynx.
A case report and review of the literature. Rev Laryngol Otol
Rhinol (Bord). 120:39–42. 1999.
|
|
14
|
Enzinger FM and Weiss SW: Liposarcoma.
Soft Tissue Tumors. 3rd edition. Mosby; St. Louis, MO: pp. 431–466.
1995
|