Introduction
Lung squamous cell carcinoma (LSCC) is one of the
most prevalent subtypes of lung cancer worldwide and its
pathogenesis is closely linked with tobacco exposure. SCC
classically arises in proximal segmental bronchi and extends into
the parenchyma and bronchial lumen, producing obstruction with
resultant atelectasis or pneumonia. Metastasis to the peritoneum
from LSCC is rare and occurs with a poor prognosis (1). Mutations in KRAS and BRAF are present
at the low frequencies of 6 and 2%, respectively, in LSCC, mostly
occurring in current or former smokers (2–5). It
has been reported that BRAF and KRAS mutations do not occur
concomitantly within the same tumor, as simultaneous mutation in
the same RAS/RAF/MEK/ERK signal pathway are redundant for the tumor
cells (3,5). The present study describes the case of
a treatment-naïve LSCC patient with coexisting BRAF V600E and
oncogenic KRAS G12A mutations in the primary lung lesion and the
peritoneum metastases, and with prominent manifestations of
peritoneal carcinomatosis and an eosinophilic leukemoid reaction.
This study was approved by the Ethics Committee of Xiangya Hospital
(Changsha, China) and was performed according to the Declaration of
Helsinki. The patient provided written informed consent.
Case report
A 63-year-old male, with a 40-year smoking history
(40 cigarettes per day) and a 35-year history of coal exposure,
presented with intolerable abdominal distention, severe fatigue,
adynamic fever and night sweats. These symptoms also dominated the
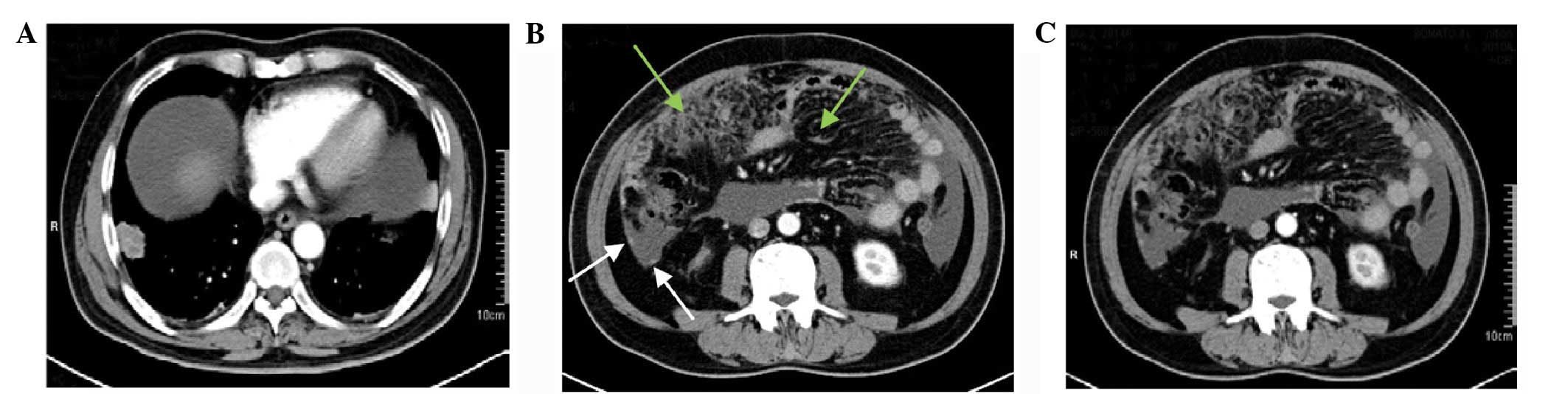
clinical course of the disease. Computed tomography (CT) identified
extensive, caked and nodule-like colic omentum thickening and
massive ascites with a 2.9×2.5-cm primary lesion in the lower lobe
of the right lung (Fig. 1). The
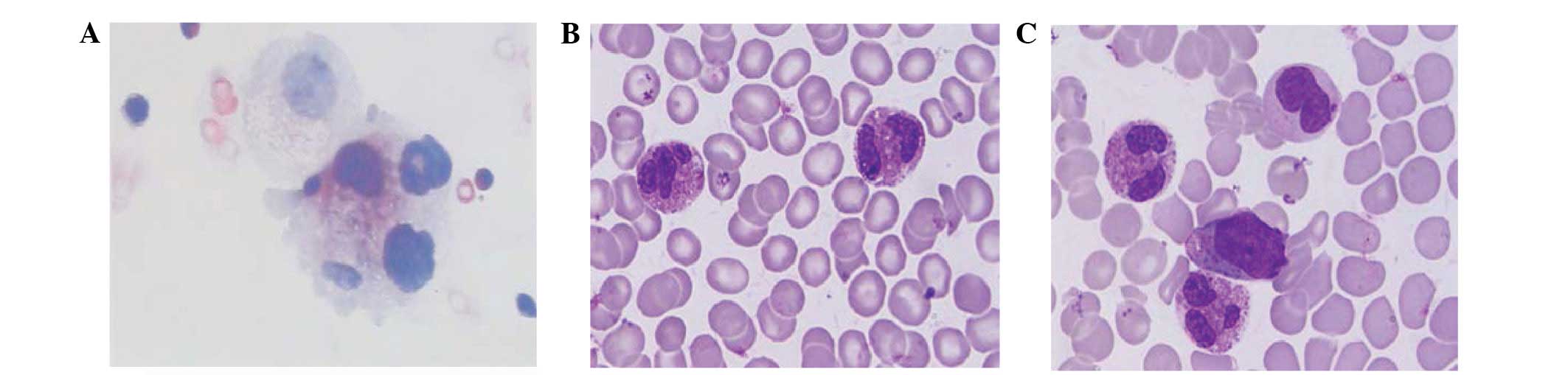
sediment cytology of the ascites following centrifugation showed a
number of dyskaryotic cells, indicating malignant ascites (Fig. 2). The blood and bone marrow cytology
results showed leukocytosis of 52.2×109/l, with
12.9×109 eosinophils per liter. In total, 20% of the
bone marrow cells were eosinophils (Fig. 2). The levels of serum interleukin
(IL)-5, immunoglobulin E and granulocyte-macrophage
colony-stimulating factor were normal. Evaluations for allergies,
infection and autoimmune and clonal mechanisms were negative.
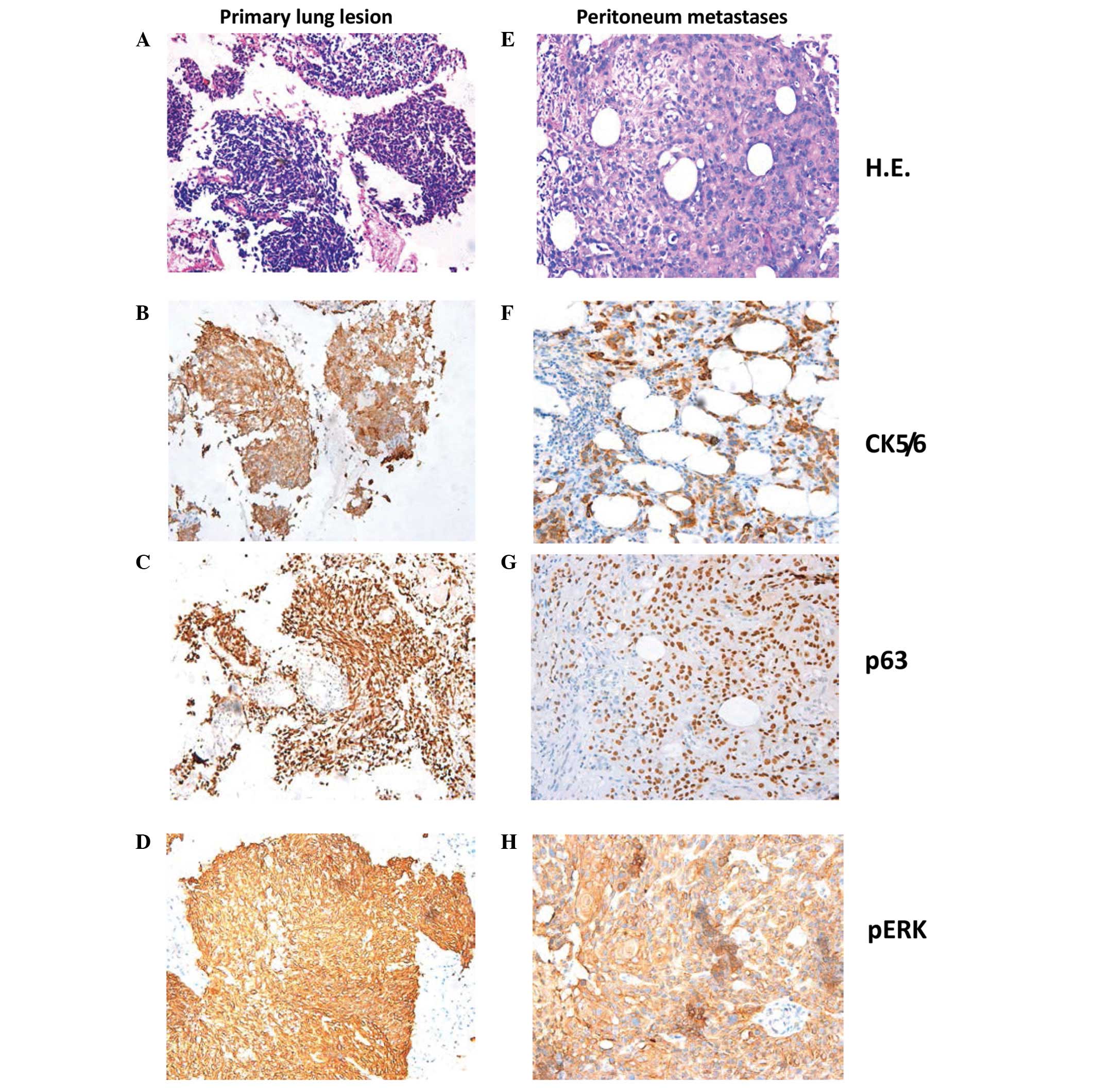
CT-guided needle aspirations from the primary lung lesion and the
thickened omentum were executed, and the histology from these
aspirations revealed poorly-differentiated squamous cells, as
confirmed by the cell morphology observed by hematoxylin and eosin
staining, together with the positive staining for cytokeratin 5/6
and p63 and the negative staining for thyroid transcription
factor-1 and napsin A observed by immunohistochemistry (Fig. 3). The biopsy specimens were sent for
molecular analysis using tissue DNA extraction and pyrosequencing
methods, which confirmed the tumor to be wild-type for EGFR exons
18, 19, 20 and 21, ROS1 and PI3K gene, and showed no abnormal ALK
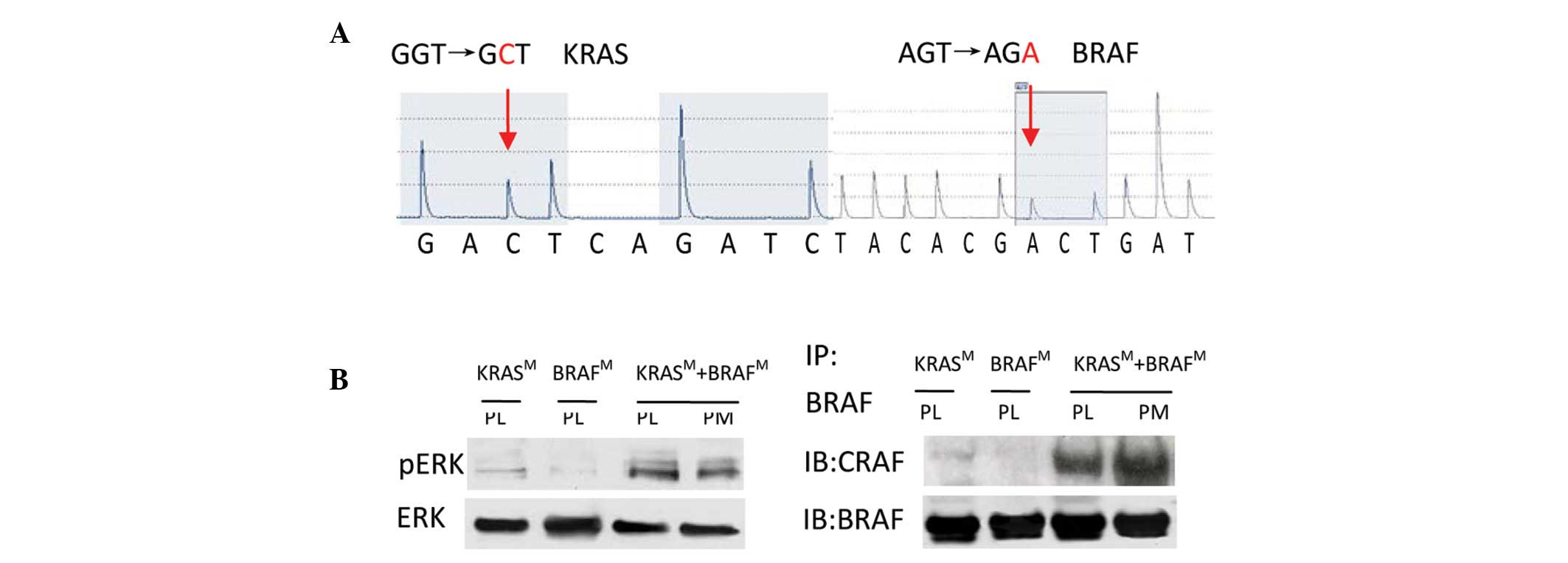
fusions. The presence of the BRAF V600E and KRAS G12A mutations was
confirmed in the primary lung lesion and in the peritoneal
metastases (Fig. 4A). Additionally,
more excessive phosphorylation of ERK protein compared with total
ERK was observed in the aspiration samples than in primary lung
lesions from LSCC with a single BRAF V600E or KRAS G12A mutation,
when analyzed by immunohistochemistry and western blot analysis
(Figs. 3 and 4B). Notably, when using the
co-immunoprecipitation method, endogenous BRAF and CRAF
dimerization was found to be significantly enhanced in the tumor
cells from the primary lung lesion and the peritoneum metastases in
the present case (Fig. 4B). The
prognosis was extremely poor, and the patient succumbed eight days
after the onset of the condition due to rapid aggravation of the
peritoneal carcinomatosis and disease resistance to treatment.
Discussion
The present study reports a noteworthy case of
peritoneal carcinomatosis from LSCC, with coexisting BRAF V600E and
oncogenic KRAS G12A mutations in the primary lung lesion and
peritoneal metastases. To the best of our knowledge, this is the
first case of this type. Other clinicopathological features,
including an eosinophilic leukemoid reaction, adynamic fever and
rapid aggravation also make this case unusual.
LSCC typically presents with the local symptoms of
coughing, chest pain and hemoptysis, or metastasis to the bone,
liver, brain and adrenal glands. Peritoneal metastases, which
usually originate from carcinoma of the gastrointestinal tract or
ovary, are believed to originate from lung cancer rarely and from
LSCC even more infrequently, always with a poor prognosis (1). Eosinophilia is rare and is usually due
to IL-5 secretion in lung cancer, although the definitive cause in
the present patient was unknown.
The patient of the present study primarily presented
with combined somatic BRAF and KRAS mutations with an aggressive
clinical history, unusual disease burden and poor prognosis. In
animal experiments, oncogenic KRAS and activated BRAF mutations
cooperate to accelerate the rapid onset of cancer (6). Oliveira et al (7) reported 5 cases of BRAF V600E and
oncogenic KRAS that preferentially coexisted in advanced colorectal
carcinoma; one of the 5 cases harbored the KRAS G12A mutation,
indicating that activation of the two genes plays a synergistic
role in tumor progression.
The BRAF and KRAS molecules share a common
RAS/RAF/MEK/ERK signaling pathway, and the ERK kinase is the
downstream convergence point of the BRAF and KRAS signaling
proteins (7). The present study
therefore evaluated the phosphorylation level of ERK by
immunohistochemistry and western blotting. The results showed that
pERK expression, compared with total ERK, was strongly positive,
and that it was more intense than the level in primary lung lesions
from LSCC with a single BRAF V600E or KRAS G12A mutation. BRAF
V600E is activated 500-fold more than the wild-type BRAF and
directly phosphorylates the ERK signaling protein in cells, which
plays a dominant role in promoting angiogenesis during tumor
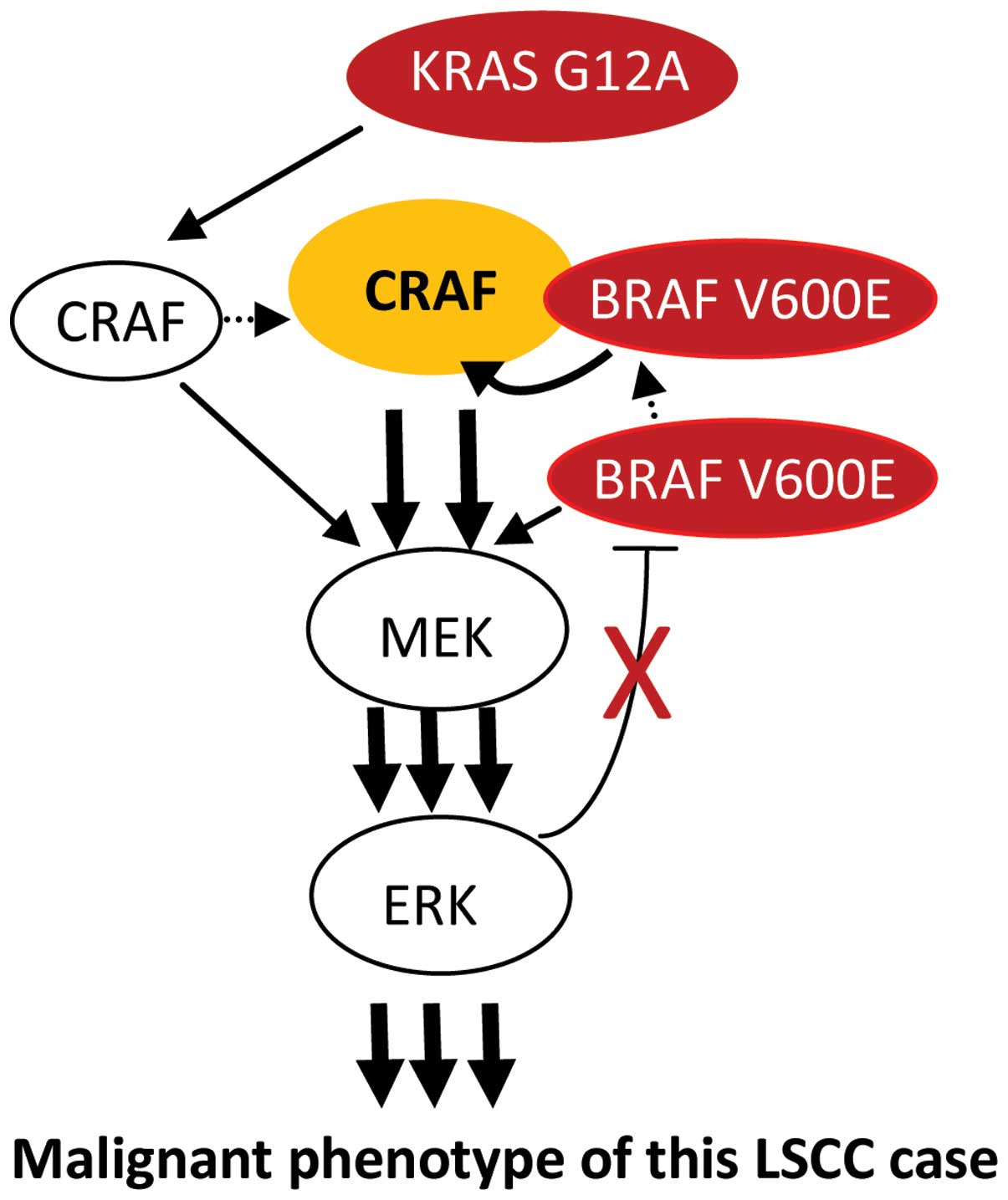
development. Oncogenic KRAS binds and activates CRAF more
efficiently and mediates KRAS signaling to ERK kinase in lung
cancer cells, thus fulfilling an important role as an
anti-apoptotic protein independent of BRAF (6,8).
Furthermore, BRAF V600E binds, transphosphorylates and
hyperactivates CRAF in the presence of oncogenic KRAS to augment
MEK/ERK signaling activation (9).
The present study results showed that endogenous BRAF and CRAF
dimerization was significantly enhanced in the tumor cells from the
primary lung lesion and the peritoneal metastases in this case.
These results raise the possibility that BRAF V600E cooperated with
KRAS G12A to augment the ERK kinase activation, which may also have
preference to eosinophil production. In addition, BRAF V600E is
highly resistant to the two negative-feedback loops of ERK-mediated
feedback phosphorylation and the induction of Sprouty proteins by
ERK signaling via a delayed feedback loop (9), which may result in persistent and
excessive activation of ERK kinase. One possible model showing the
cooperation of the activating mutations, KRAS G12A and BRAF V600E,
is shown in Fig. 5.
The occurrence of carcinoma is a multistep procedure
and the result of an accumulation of gene mutations or abnormal
expression. Cigarette and coal dust have been proven to be
mutagenic factors of KRAS and BRAF in lung cancer (3). The present patient had an unusual
history of heavy smoking with 40 cigarettes per day for 40 years
and a 35-year history of coal exposure, which maybe the principal
cause of the individual genotype found. A recent study has
suggested that the dominant molecular oncogenes are associated with
different biological behaviors manifesting as distinct patterns of
metastatic spread in treatment-naïve lung cancer (10). Although the exact interaction
between tobacco, coal and the carcinogenesis of bronchial
epithelial cells has not yet been studied, the present case appears
to indicate that intensive phosphorylation of ERK kinase caused the
unusual spread pattern and eosinophilia of this specific type of
LSCC, with dual mutations of KRAS G12A and BRAF V600E.
In conclusion, this is the first case study on the
coexistence of the KRAS G12A and BRAF V600E mutations in LSCC. This
case indicates that this specific double mutation of BRAF V600E and
KRAS G12A results in a poor clinical course, potentially through
the acceleration of tumor progression. The case also demonstrated
an unusual spread pattern of this specific dual-mutated tumor, such
that clinicians should be aware of its identification. Recently,
certain studies have confirmed that single target inhibitors in a
double BRAF-V600E and oncogenic RAS mutation accelerate tumor
progression (11,12). Although the exact pathogenesis
remains uncertain, the present study highlights the importance of
obtaining a complete understanding of how networks function in this
specific dual-mutated tumor. The mechanism of cooperation of the
BRAF V600E and oncogenic KRAS mutations may represent a model for
the mutation of differing molecules in the same signaling
pathway.
Acknowledgements
This study was supported by grants from the National
Natural Scientific Foundation of China (nos. 30670990, 30871189,
81171841, 81200366 and 81372515) and The Key Subject Education
Department of Hunan [no. (2012)594].
References
|
1
|
Su HT, Tsai CM and Perng RP: Peritoneal
carcinomatosis in lung cancer. Respirology. 13:465–467. 2008.
|
|
2
|
Sos ML and Thomas RK: Genetic insight and
therapeutic targets in squamous-cell lung cancer. Oncogene.
31:4811–4814. 2012.
|
|
3
|
Paik PK, Arcila ME, Fara M, et al:
Clinical characteristics of patients with lung adenocarcinomas
harboring BRAF mutations. J Clin Oncol. 29:2046–2051. 2011.
|
|
4
|
Cancer Genome Atlas Research Network.
Comprehensive genomic characterization of squamous cell lung
cancers. Nature. 489:519–525. 2012.
|
|
5
|
Heist RS, Sequist LV and Engelman JA:
Genetic changes in squamous cell lung cancer: A review. J Thorac
Oncol. 7:924–933. 2012.
|
|
6
|
Heidorn SJ, Milagre C, Whittaker S, et al:
Kinase-dead BRAF and oncogenic RAS cooperate to drive tumor
progression through CRAF. Cell. 140:209–221. 2010.
|
|
7
|
Oliveira C, Velho S, Moutinho C, et al:
KRAS and BRAF oncogenic mutations in MSS colorectal carcinoma
progression. Oncogene. 26:158–163. 2007.
|
|
8
|
Blasco RB, Francoz S, Santamaría D, et al:
c-Raf, but not B-Raf, is essential for development of K-Ras
oncogene-driven non-small cell lung carcinoma. Cancer Cell.
19:652–663. 2011.
|
|
9
|
Röring M and Brummer T: Aberrant B-Raf
signaling in human cancer - 10 years from bench to bedside. Crit
Rev Oncog. 17:97–121. 2012.
|
|
10
|
Doebele RC, Lu X, Sumey C, et al: Oncogene
status predicts patterns of metastatic spread in treatment-naive
nonsmall cell lung cancer. Cancer. 118:4502–4511. 2012.
|
|
11
|
Kaplan FM, Shao Y, Mayberry MM and Aplin
AE: Hyperactivation of MEK-ERK1/2 signaling and resistance to
apoptosis induced by the oncogenic B-RAF inhibitor, PLX4720, in
mutant N-RAS melanoma cells. Oncogene. 30:366–371. 2011.
|
|
12
|
Kern F, Doma E, Rupp C, et al: Essential,
non-redundant roles of B-Raf and Raf-1 in Ras-driven skin
tumorigenesis. Oncogene. 32:2483–2492. 2013.
|