Introduction
Neuroendocrine carcinomas (NECs) account for <5%
of unknown primary cancers (CUPs) worldwide (1). A primary site in the larynx is rare;
Hess et al (2) reported 43
patients with NEC in 1,000 CUP patients and there was no case of a
carcinoma in the larynx. To date, there are ~520 cases of NEC with
CUP in the English-language literature (3–6) and to
the best of our knowledge, there is only one previously reported
case of a CUP of NEC from the larynx (6).
Detection of the carcinoma origin in CUP patients is
a challenge. Although the primary sites may be identified by
conventional modalities, including complete physical examination,
panendoscopy and conventional imaging (including computed
tomography [CT], magnetic resonance imaging [MRI] and even random
biopsies (including, tonsillectomies) commonly, the origin remains
undetected using the conventional diagnostic procedures (7).
Accurate identification of the unknown primary site
is important, as it enables the therapy to be focused towards the
known site of origin, thus, decreasing treatment-associated
morbidity and improving therapeutic efficacy (9,10).
18F-fluorodeoxyglucose (FDG) positron emission
tomography (PET)/CT has provided novel insights in the diagnosis of
CUP (8,9). However, there have been few studies
regarding the effectiveness of 18F-FDG PET/CT in
detecting the CUP in NEC (4–6,10).
In the present study, we report a case of cervical
metastatic small-cell (SC) NEC of CUP and detected the origin in
the larynx using 18F-FDG PET/CT. The patient’s family
provided written informed consent.
Case report
Patient
A 67-year-old male presented to the Department of
Otolaryngology, The First Affiliated Hospital, College of Medicine,
Zhejiang University (Hangzhou, China), on August 30, 2010 with a
one-month history of a progressively enlarging mass in the right
side of the neck. The patient’s medical history was unremarkable,
although he was a heavy smoker. The ear, nose and throat
examination was normal, which included a nasoendoscopy and
laryngoscopy. A CT scan of the neck revealed no additional abnormal
finding other than the lymphadenopathy of the right neck. MRI of
the nasopharynx identified abnormal lesions in the nasopharynx and
a biopsy of the lymphadenopathy in the right upper neck indicated a
poorly differentiated metastatic carcinoma; a nasopharyngeal biopsy
did not detect carcinoma cells. Furthermore, a pulmonary CT and
gastroscopy did not reveal any abnormal finding in the lung or
stomach. Subsequently, 18F-FDG PET/CT was performed.
PET/CT
Whole-body imaging was conducted using a combined
PET/CT scanner (Biograph Sensation 16. LSO 39-ring; Siemens
Medical, Erlangen, Germany). Following ≥4–6 h of fasting, the
patient received an intravenous injection of 18F-FDG at
5.5–7.4 MBq (0.15–0.20 mCi)/kg body weight. Patient blood glucose
levels were assessed prior to the 18F-FDG injection.
Data acquisition for the diagnostic CT commenced 60–90 min prior to
18F-FDG administration. The data acquisition procedure
was as follows: i) A 16-section multi-detection row CT scan was
performed from head to mid-thigh at 120 kV, 50 mAs. ii) Using a
tube rotation time of 0.5 sec, a 2–5-mm thick section was matched
to the PET section thickness. iii) Finally, a three-dimensional PET
was conducted with the patient in the same supine position. The PET
scan incorporated the subcranial region to the mid-thigh; however,
the brain scan required an additional bed position. The acquisition
time was 2 min per bed position. The total imaging time of the
PET/CT study was ~20 min. Attenuation correction was based on the
CT scan. The PET images were reconstructed iteratively using the
ordered subset Syngo Speaking software (Wizard Workstation; Siemens
Medical). PET, CT and fused PET/CT images were generated and
reviewed on a computer; the co-registered images were displayed on
a workstation. The PET/CT scans were interpreted independently by
two experienced members of our PET centre who were unaware of the
histology of the metastatic sites. Any differences in their
interpretations were settled by consensus with a final unanimous
opinion. The standardised uptake value (SUV) was collected from the
predominant lesion and calculated based on the
attenuation-corrected images, amount of injected 18F-FDG
and patient body weight: SUVmax = [decay corrected
activity (kBq)/tissue volume (ml)]/[injected 18F-FDG
activity (kBq)/body weight (g)]. When multiple lymph nodes were
found, only the lymph node with the greatest SUVmax was
used.
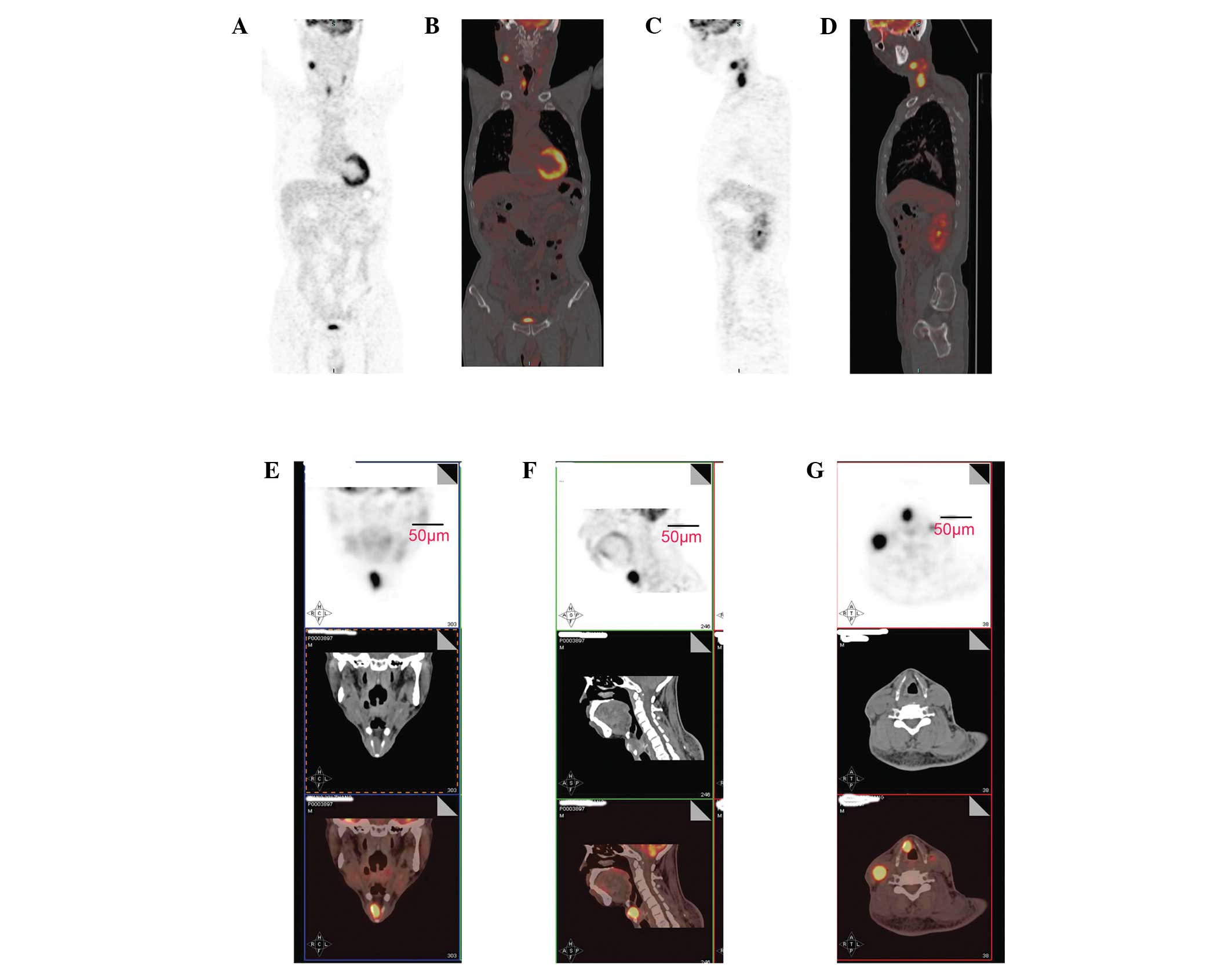
PET/CT showed increased 18F-FDG uptake in
the right larynx (SUVmax = 8.37) and right neck lymph
nodes (SUVmax = 11.5; Fig.
1). These findings indicated the possibility of a primary
laryngeal carcinoma.
Surgery
A smooth lesion was observed in the submucosa of the
right laryngeal ventricle and the right false vocal cord using
suspension laryngoscopy under general anaesthesia. A deep biopsy
was performed and a frozen section revealed a laryngeal SC
carcinoma. The diagnosis was supraglottic laryngeal carcinoma
(T2N2CM0), clinical stage IV
according to the tumor, lymph node, metastases (TNM) staging system
(11). A total laryngectomy and
bilateral neck dissection were performed simultaneously. During
surgery, the largest lymph node observed in the left neck was
~3.0×1.8×1.6 cm, and multiple small lymph nodes were identified
around the left jugular vein and carotid artery. These lymph nodes
did not adhere to the blood vessels above. A selective neck
dissection of the left II, III, IV and V regions, preserving the
left jugular vein, sternocleidomastoid muscle and accessory nerve,
was performed. In addition, multiple lymph nodes were observed in
the right neck around the jugular vein and carotid artery. The
largest was ~5.2×3.8×3.5 cm, somewhat adherent to the right carotid
artery and surrounded the right jugular vein tightly. A selective
neck dissection of the right II, III, IV and V regions and
dissection of the right jugular vein and sternocleidomastoid
muscle, with preservation of the accessory nerve, was performed. A
prelaryngeal lymph node of ~5×4×3.4 mm was dissected
simultaneously. The primary lesion in the larynx (size,
~2.5×2.3×1.8 cm) was a smooth submucosal lesion, which was located
predominantly in the right supraglottic area and involved the
preepiglottic space, right false vocal cord and laryngeal
ventricle. The postoperative period was uneventful.
Pathological and immunohistochemical
findings
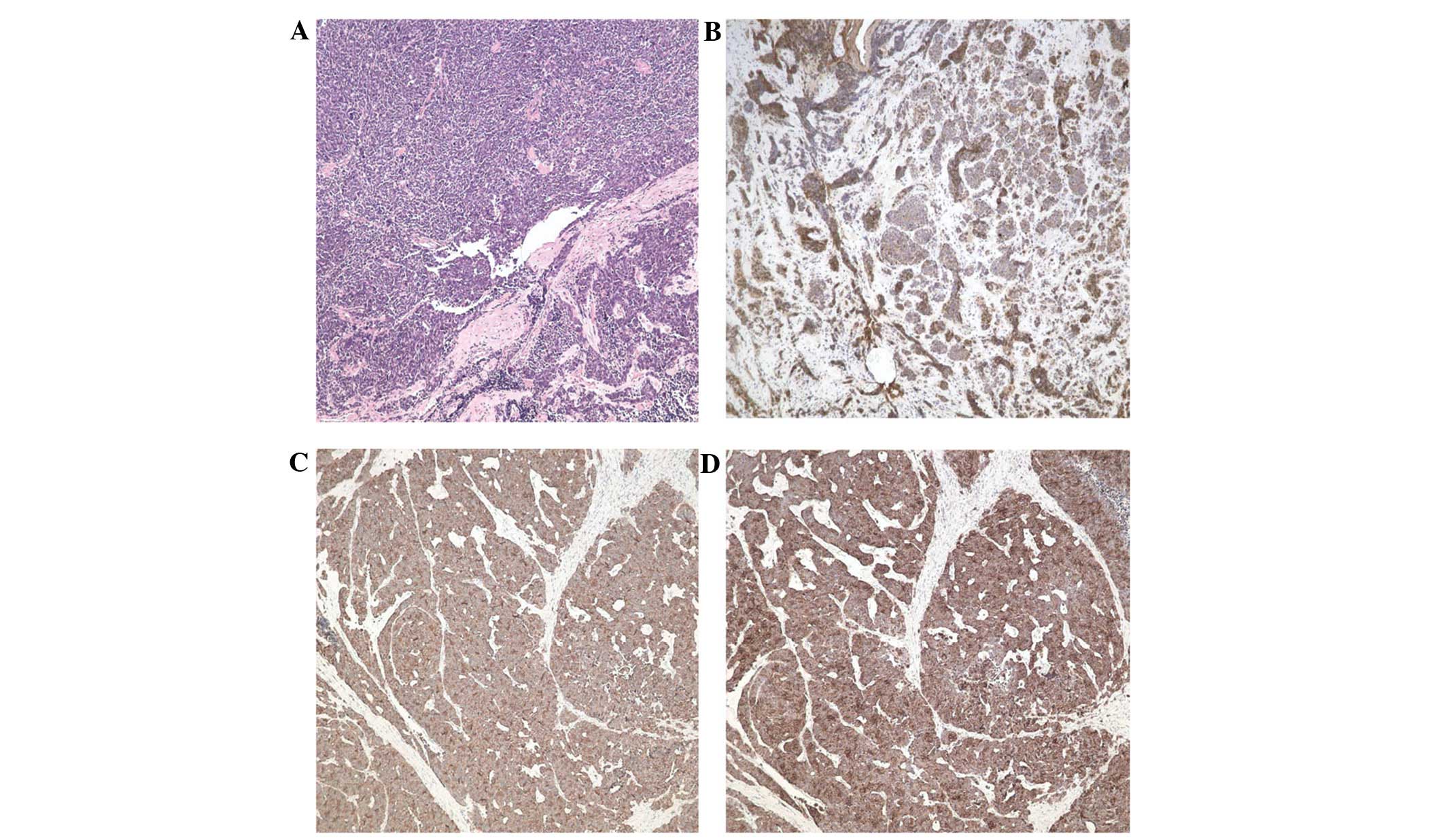
Microscopically, the lesions were composed of sheets
of small atypical cells with sparse cytoplasm and large, round
nuclei (Fig. 2A). The
immunohistochemical results revealed that the neoplastic cells were
positive for cytokeratins (Fig.
2B), synaptophysin (Fig. 2C)
and chromogranin A (Fig. 2D), and
negative for neuron-specific enolase, vimentin, desmin and S-100.
These resulted indicated SCNEC in the larynx. Five lymph nodes in
the right neck, one lymph node in the left neck and one
prelaryngeal lymph node were positive for metastatic SCNEC. The
pathological TNM stage was pT2N2M0
and the resection margins were negative.
Follow-up
The patient received concurrent chemoradiotherapy
postoperatively, however, succumbed due to distant metastasis one
year following surgery.
Discussion
NEC of CUP is rare, and its diagnosis and therapy
are complex. Stoyianni et al (12) systematically reviewed all
English-language publications studying neuroendocrine CUP patients,
and identified only 500 cases. Since that study, an additional 20
NEC patients with CUP have been reported (3–6). To
the best of our knowledge, there is only one reported case of CUP
of NEC from the larynx (6). NEC of
CUP has a particularly poor outcome. If the primary site is
detected and the metastasis is confined to a single site, surgery
or radiation therapy may be conducted and can occasionally be
curative (1).
Laryngeal NEC is rare and constitutes <1% of all
tumours originating from the larynx (13). Laryngeal SCNEC, located in the
submucosa of the larynx (14), and
approximately half of all laryngeal SCNEC occur as cervical
lymphadenopathy; however, the primary lesion may be difficult to
detect as CUP (6). PET/CT has been
used widely in the detection of CUP; however, there have been few
reports concerning the detection of CUP of NEC using PET/CT
(3–6). Naswa et al (5) detected the primary tumour in 12/20
(60%) patients with CUP of NEC using 68Ga-DOTA-NOC
PET/CT. In addition, Prasad et al (10) demonstrated that
68Ga-DOTA-NOC PET/CT localised the primary tumour in 59%
of patients. The management of 15 and 10% of patients in the two
reports, respectively, was modified upon identifying the primary
tumour. The authors proposed that 68Ga-DOTA-NOC PET/CT
had particularly high sensitivity and specificity in the detection
of NECs. Certain studies have shown that 18F-FDG PET/CT
is able to detect unknown primary tumours and additional metastatic
sites in patients with CUP (9,15).
However, Adams et al (16)
also identified false-negative results in the detection of 15 NECs
due to a low rate of tumour glucose metabolism. Thus, whether there
is high uptake of 18F-FDG in the NECs remains
controversial. In the present case, we detected high
18F-FDG uptake in the larynx and cervical lymph nodes.
High 18F-FDG uptake in cancer lesions (including NEC) is
associated with the overexpression of glucose transporter-1
(GLUT-1) (17). In the present
case, GLUT-1 protein expression was identified as positive by
immunohistochemistry. In our previous case report, high
18F-FDG uptake in the cervical lymph nodes and lungs was
observed in a patient with tonsillar metastasis from a lung SCNEC
(18). Furthermore, Miki et
al (6) reported high
18F-FDG uptake in a case of a metastatic cervical SCNEC
from the larynx by 18F-FDG PET/CT. In addition, high
18F-FDG uptake has been detected in metastatic NECS from
other sites (19–22). Song et al (17) found that 18F-FDG uptake
was correlated with GLUT-1 expression in 32 lung NECs. Thus,
whether there is low or high glucose metabolism in NECs requires
further investigation according to the NEC type.
Laryngeal NECs usually arise submucosally and may be
too small to be detected by PET (6). Therefore, the performance of deeper
submucosal biopsies is required once NECs have been detected via
radiological imaging. SCNECs are particularly aggressive tumours.
Approximately 50% of all SCNEC patients present with cervical lymph
node metastases and >90% of patients with this type of tumour
develop metastatic disease (23).
Laryngeal SCNEC is located predominantly in the supraglottis and
its metastasis to neck lymph nodes always occurs earlier than that
in the glottic area and unilaterally. In the present case,
bilateral metastatic cervical lymph nodes (including the
prelaryngeal lymph node) were present, which were demonstrated by
the pathological examination.
There is no specific treatment for NEC of the
larynx. Patients may benefit from surgery; however, radiotherapy
and chemotherapy remain the treatments of choice (14). However, surgical management of
laryngeal SCNEC is not as effective. Radical surgical procedures
(including total laryngectomy and radical neck dissection) have
failed in the majority of reported cases (24). A total laryngectomy was performed in
the present case and the patient received concurrent
chemoradiotherapy postoperatively. However, the outcome was
unfavourable as the patient succumbed due to distant metastasis one
year after surgery, which is similar to a previous report (6). As a result of the current case, it is
proposed that frozen sections should not be obtained during surgery
and that the pathological type of the laryngeal tumour requires
accurate identification preoperatively, using routine pathological
examinations, including immunohistochemistry. Once the diagnosis of
laryngeal SCNEC is established, concurrent chemoradiotherapy is
considered to be the optimum treatment regimen (24). As early as 1986, Baugh et al
(25) found that the combination of
radiotherapy and chemotherapy resulted in a significantly longer
survival time compared with any other treatment regimen. In the
same year, Ferlito et al (26) reported a case of laryngeal SCNEC,
where the patient was free of disease for more than five years
following treatment with chemotherapy and radiotherapy. Recently,
definitive chemoradiotherapy was associated with better outcomes in
extrapulmonary SC cancers (27).
Thus, it is proposed that the therapeutic methods for laryngeal
SCNEC should not follow those of squamous cell carcinoma as others
have recommended (14) and,
instead, laryngeal SCNEC should be considered as a systemic
disease, as SC lung cancer is (24).
In conclusion, the present study is the second case
of a CUP of NEC from the larynx. 18F-FDG PET/CT is
considered to be an effective work-up for the detection of CUP of
NEC. As a result of the present case, it is proposed that frozen
sections should not be obtained during surgery and that the
pathological type of the laryngeal tumour should be accurately
established preoperatively via routine pathological examinations,
including immunohistochemistry. Once the diagnosis of laryngeal
SCNEC is established, concurrent chemoradiotherapy is considered to
be the optimum treatment regimen.
Acknowledgements
The authors would like to thank the National Natural
Science Foundation of China (grant nos. 81172562 and 81372903) and
the Health Department of Zhejiang Province (grant nos. 2009B042 and
2010KYA062).
References
|
1
|
Spigel DR, Hainsworth JD and Greco FA:
Neuroendocrine carcinoma of unknown primary site. Semin Oncol.
36:52–59. 2009.
|
|
2
|
Hess KR, Abbruzzese MC, Lenzi R, Raber MN
and Abbruzzese JL: Classification and regression tree analysis of
1000 consecutive patients with unknown primary carcinoma. Clin
Cancer Res. 5:3403–3410. 1999.
|
|
3
|
Lee HS, Han HS, Lim SN, et al: Poorly
differentiated neuroendocrine carcinoma in a perigastric lymph node
from an unknown primary site. Cancer Res Treat. 44:271–274.
2012.
|
|
4
|
Kim HY, Choi SI and Kim YH: Neuroendocrine
tumor of unknown primary accompanied with stomach adenocarcinoma. J
Gastric Cancer. 11:234–238. 2011.
|
|
5
|
Naswa N, Sharma P, Kumar A, et al:
68Ga-DOTANOC PET/CT in patients with carcinoma of
unknown primary of neuroendocrine origin. Clin Nucl Med.
37:245–251. 2012.
|
|
6
|
Miki K, Orita Y, Nose S, et al:
Neuroendocrine carcinoma of the larynx presenting as a primary
unknown carcinoma. Auris Nasus Larynx. 39:98–102. 2012.
|
|
7
|
de Bree R: The real additional value of
FDG-PET in detecting the occult primary tumour in patients with
cervical lymph node metastases of unknown primary tumour. Eur Arch
Otorhinolaryngol. 267:1653–1655. 2010.
|
|
8
|
Deron PB, Bonte KM, Vermeersch HF and Van
de Wiele C: Lymph node metastasis of squamous cell carcinoma from
an unknown primary in the upper and middle neck: Impact of
(18)F-fluorodeoxyglucose positron emission tomography/computed
tomography. Cancer Biother Radiopharm. 26:331–334. 2011.
|
|
9
|
Zhao K, Luo XM, Zhou SH, et al:
18F-fluorodeoxyglucose positron emission
tomography/computed tomography as an effective diagnostic workup in
cervical metastasis of carcinoma from an unknown primary tumor.
Cancer Biother Radiopharm. 27:685–693. 2012.
|
|
10
|
Prasad V, Ambrosini V, Hommann M, Hoersch
D, Fanti S and Baum RP: Detection of unknown primary neuroendocrine
tumours (CUP-NET) using (68)Ga-DOTA-NOC receptor PET/CT. Eur J Nucl
Med Mol Imaging. 37:67–77. 2010.
|
|
11
|
Sobin LH and Wittekind CH: International
Union Against Cancer (UICC). TNM classification of malignant
tumours. 5th edition. Wiley-Liss; New York, NY: pp. 3361997
|
|
12
|
Stoyianni A, Pentheroudakis G and Pavlidis
N: Neuroendocrine carcinoma of unknown primary: a systematic review
of the literature and a comparative study with other neuroendocrine
tumors. Cancer Treat Rev. 37:358–365. 2011.
|
|
13
|
Ferlito A, Silver CE, Bradford CR and
Rinaldo A: Neuroendocrine neoplasms of the larynx: an overview.
Head Neck. 31:1634–1646. 2009.
|
|
14
|
Mikić A, Zvrko E, Trivić A, Stefanović D
and Golubović M: Small cell neuroendocrine tumor of the larynx - a
small case series. Coll Antropol. 36(Suppl 2): 201–204. 2012.
|
|
15
|
Møller AK, Loft A, Berthelsen AK, et al: A
prospective comparison of 18F-FDG PET/CT and CT as diagnostic tools
to identify the primary tumor site in patients with extracervical
carcinoma of unknown primary site. Oncologist. 17:1146–1154.
2012.
|
|
16
|
Adams S, Baum R, Rink T, Schumm-Dräger PM,
Usadel KH and Hör G: Limited value of fluorine-18
fluorodeoxyglucose positron emission tomography for the imaging of
neuroendocrine tumours. Eur J Nucl Med. 25:79–83. 1998.
|
|
17
|
Song YS, Lee WW, Chung JH, Park SY, Kim YK
and Kim SE: Correlation between FDG uptake and glucose transporter
type 1 expression in neuroendocrine tumors of the lung. Lung
Cancer. 61:54–60. 2008.
|
|
18
|
Chen XH, Bao YY, Zhou SH, Wang QY and Zhao
K: Palatine tonsillar metastasis of small-cell neuroendocrine
carcinoma from the lung detected by FDG-PET/CT after tonsillectomy:
A case report. Iran J Radiol. 10:148–151. 2013.
|
|
19
|
Ozpacaci T, Tamam MO, Mulazimoglu M,
Kamali G and Ozcan D: Isolated adrenal metastasis of small cell
neuroendocrine carcinoma of the ovary detected with FDG-PET/CT. Rev
Esp Med Nucl Imagen Mol. 31:297–298. 2012.
|
|
20
|
Treglia G, Salomone E, Petrone G, Giaccari
A, Rindi G and Rufini V: A rare case of ectopic adrenocorticotropic
hormone syndrome caused by a metastatic neuroendocrine tumor of the
pancreas detected by 68Ga-DOTANOC and 18F-FDG PET/CT. Clin Nucl
Med. 38:e306–e308. 2013.
|
|
21
|
Treglia G, Plastino F and Campitiello M:
Staging and treatment response evaluation in a metastatic
neuroendocrine tumor of the pancreas with G2 grading: insights from
multimodality diagnostic approach by F-18-FDG and Ga-68-DOTANOC
PET/CT. Endocrine. 43:729–731. 2013.
|
|
22
|
Liu Y: FDG PET-CT demonstration of
metastatic neuroendocrine tumor of prostate. World J Surg Oncol.
6:642008.
|
|
23
|
Kim HJ and Hwang EG: Small cell carcinoma
of the larynx: imaging findings. Auris Nasus Larynx. 24:423–427.
1997.
|
|
24
|
Ferlito A and Rinaldo A: Primary and
secondary small cell neuroendocrine carcinoma of the larynx: a
review. Head Neck. 30:518–524. 2008.
|
|
25
|
Baugh RF, Wolf GT, Beals TF, Krause CJ and
Forastiere A: Small cell carcinoma of the larynx: results of
therapy. Laryngoscope. 96:1283–1290. 1986.
|
|
26
|
Ferlito A, Pesavento G, Recher G, et al:
Long-term survival in response to combined chemotherapy and
radiotherapy in laryngeal small cell carcinoma. Auris Nasus Larynx.
13:113–123. 1986.
|
|
27
|
Brennan SM, Gregory DL, Stillie A,
Herschtal A, Mac Manus M and Ball DL: Should extrapulmonary small
cell cancer be managed like small cell lung cancer? Cancer.
116:888–895. 2010.
|