Introduction
Primary intraosseous carcinoma (PIOC) of the jaw is
a rare carcinoma arising from the odontogenic epithelium without
connection to the oral mucosa. The tumor is considered to develop
from a remnant of the odontogenic epithelium.
PIOC was first described as a central epidermoid
carcinoma of the jaw by Loos (1) in
1913. The classification of PIOC has since undergone numerous
revisions and the precise diagnostic criteria of PIOC has not yet
been established.
The term PIOC was established by the World Health
Organization (WHO) as part of the classification for the
histological typing of odontogenic tumors (2). Elzay (3) reviewed the literature associated with
PIOC of the jaw and subsequently insisted that a modification of
the WHO classification was required. Slootweg and Müller (4) also recommended modifications, while a
study by Waldron and Mustoe (5) and
Müller and Waldron (6) added
intraosseous mucoepidermoid carcinoma to the classification.
According to the WHO (7), PIOC may be categorized into three
types: i) A solid tumor invading the bone marrow spaces and
inducing osseous resorption; ii) a squamous cell carcinoma arising
from the epithelial lining of an odontogenic cyst; and iii) a
squamous cell carcinoma that is associated with other benign
epithelial odontogenic tumors.
Although the classification has improved, the
etiology of PIOC remains unclear. PIOC may be derived from the
direct transformation of the odontogenic epithelium, particularly
the odontogenic epithelial rests, such as Malassez’s epithelial
rest, from within the alveolar bone following tooth loss or from
the remnants of the dental lamina and the reduced enamel epithelium
surrounding an unerupted or impacted tooth (8).
With regard to the rare cases of PIOC derived from
odontogenic cysts, a common criteria for PIOC has been established
based on the published case reports and is as follows: i) The
absence of another primary tumor on chest radiographs, as
metastatic carcinoma is the most common malignancy of the jaw and
thus, the diagnosis of PIOC must always be confirmed by the
exclusion of a metastasis; ii) the absence of an ulcer in the oral
mucosa overlaying the tumor; and iii) histopathological evidence of
transition of the epithelial lining into squamous cell carcinoma
(9,10).
In the current study, a case of PIOC arising from an
odontogenic cyst is presented and the issues concerning the
differential diagnosis and management are discussed. The patient
provided written informed consent.
Case report
A 59-year-old female was referred to Asahi
University Murakami Memorial Hospital (Gifu, Japan), with acute
pain in the right molars. There was no history of tobacco or
alcohol use, however, the patient had suffered from hyperlipidemia
several years previously.
Initial observations revealed right buccal swelling
and paresthesia of the mental nerve. An intraoral examination
revealed a normal oral mucosa, however, percussion pain was
experienced between the lower right first premolar and second
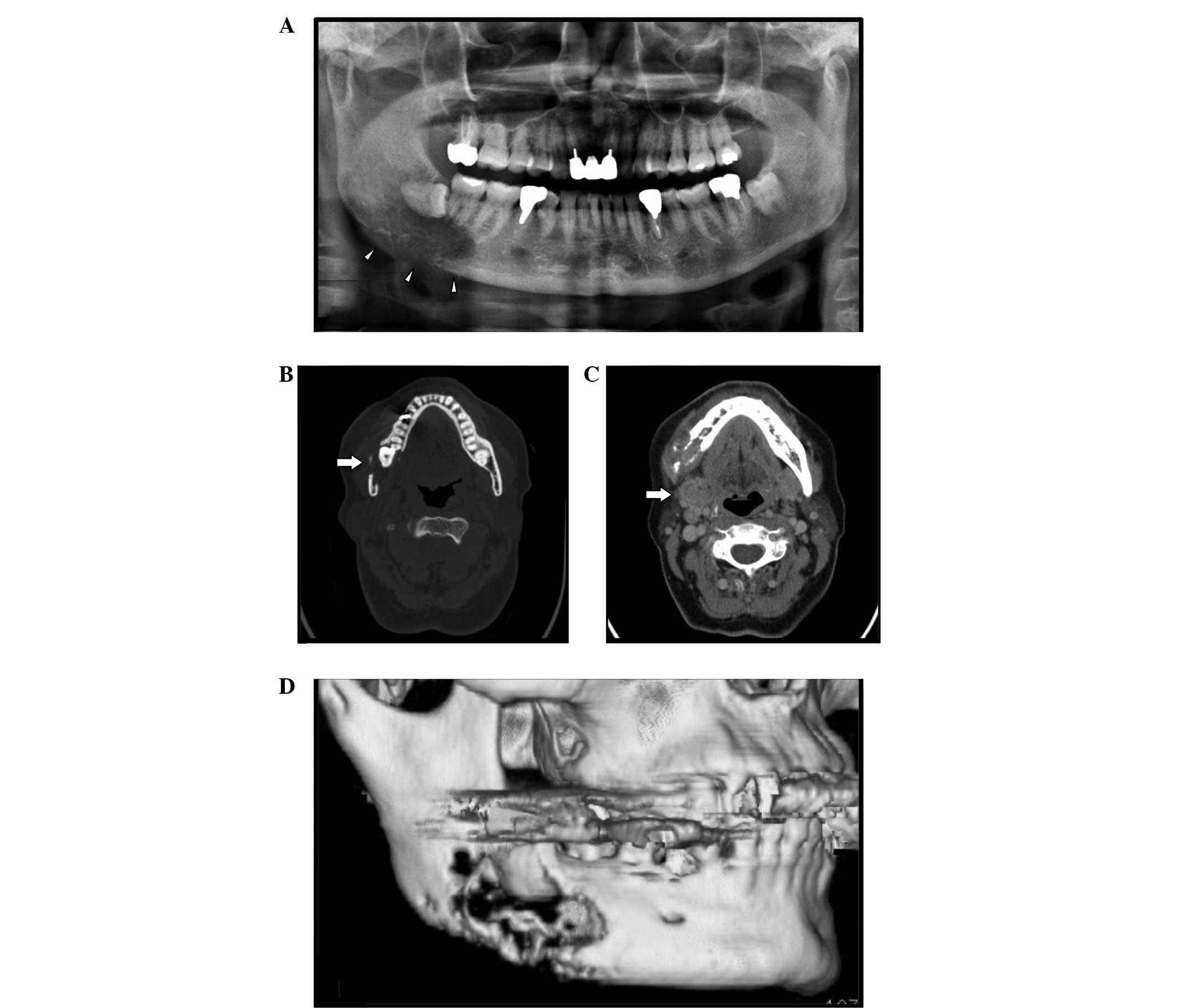
molar. The routine panoramic radiograph showed a retained lower
right wisdom tooth and an irregular radiolucent area between the
lower right molar and mandibular angle, with unclear margins
(Fig. 1A). In addition, computed
tomography (CT) revealed a large oval mass, 44×31×35 mm in size, at
the right angle of the mandible between the second premolar and
ramus, with extensive bony destruction of the lingual and buccal
cortex and pathological lymph node enlargement at the right
submandibular lesion (Fig.
1B–D).
Laboratory results revealed that the white blood
cell count was 5,400 cells/μl and the C reactive protein level was
0.3 mg/dl.
Following a biopsy of the lesion, squamous cell
carcinoma arising from an epithelial lining of an odontogenic cyst
was diagnosed. Two weeks after diagnosis, radical surgery (a
hemi-mandibulectomy with primary suture and reconstruction using a
titan reconstruction plate and modified radical neck dissection)
was performed under general anesthesia.
Intraoperative observations revealed that the tumor
had extended through the buccal and lingual cortex and invaded the
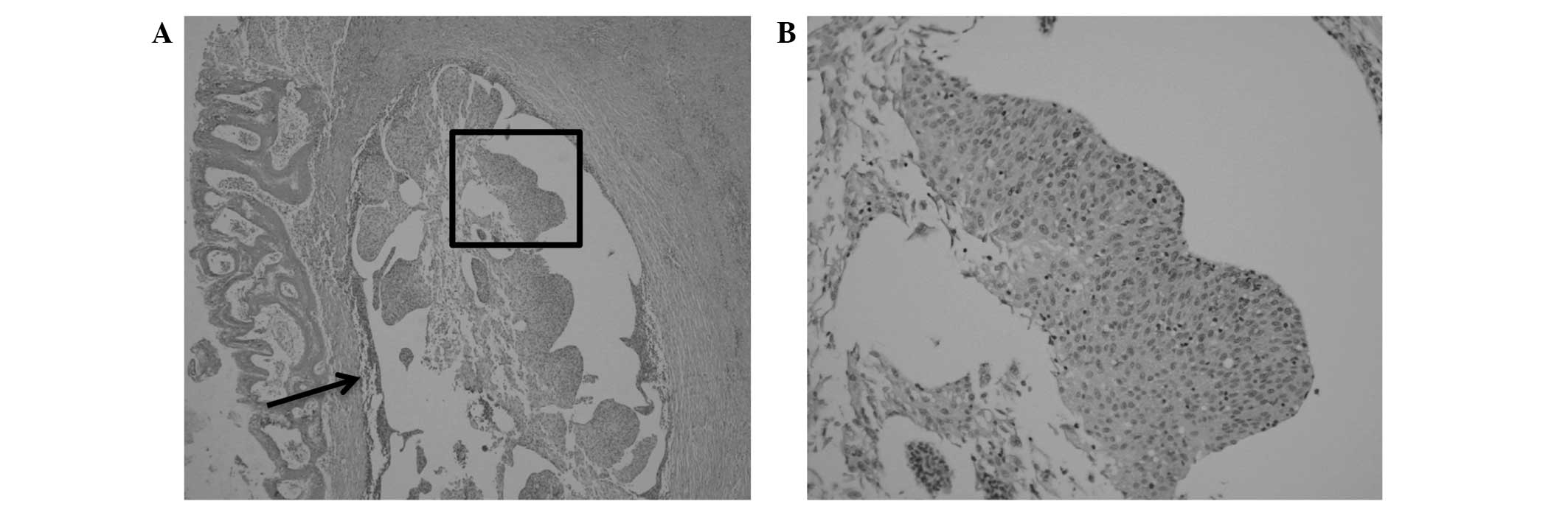
masseter and internal pterygoid muscles. In addition, pathological
examination of the surgical specimen revealed squamous cell
carcinoma with an intact squamous epithelium, which was observed to
be overlying the tumor (Fig. 2).
Lymph node metastasis was not observed in the neck lymph nodes. A
positive margin was present in the specimen at the end of the
inferior alveolar nerve, therefore the patient received
post-operative radiotherapy, and chemotherapy. External beam
irradiation was performed five times per week at 2 Gy per fraction
to a total of 60 Gy, while the doses of the oral administration of
tegafur, gimeracil and oteracil potassium were 60
mg/m2/day for two weeks followed by a two week rest for
a total of six months. The one-year post-operative follow-up
revealed no local recurrence or distant metastasis.
Discussion
PIOC is a rare carcinoma that arises from the direct
transformation of odontogenic epithelial rests in the jaw,
including the epithelial rests found within the alveolar bone and
periodontal ligament, a persistent dental lamina and the enamel
epithelium surrounding an impacted tooth (7,8).
The factors responsible for the malignant
transformation of the cystic lining of odontogenic cysts remains
unclear. The most common factor may be a chronic inflammatory
stimulus with or without a predisposing genetic cofactor, which
induces neoplastic transformation (11,12).
Coussens and Werb proposed a potential association
between sites of chronic inflammation and the development of cancer
as early as 1863, and this has proven to be fairly accurate
(13). A number of cancers have
been presumed to originate in tissues that are chronically
inflamed, and the inflammatory microenvironment is considered to
promote the progression of malignancy, including initiation,
growth, angiogenesis, invasion and metastasis, however, the precise
mechanisms have not yet been established (5).
PIOC occurs in a wide age range of individuals,
having been identified in patients between 1.3 and 90 years, with
an estimated mean age of 60.2 years. Furthermore, the incidence of
PIOC is much higher in males than females (14).
PIOC has most frequently been found in the
molar-ramus region of the mandible (15,16).
The recurrent clinical symptoms are swelling, pain/toothache and
lesion growth. These early symptoms are commonly followed by trimus
and numbness of the mandibular nerve and muscle invasion. In the
present case, the patient exhibited right buccal swelling and
paresthesia of the mental nerve.
Although the diagnostic criteria of PIOC remains
unclear, the following criteria have been suggested: i) The tumor
must be a histopathologically-based squamous cell carcinoma without
the involvement of any other odontogenic cysts or metastatic tumor
cells; ii) it must exhibit intact mucosa; and iii) no other distant
primary tumor must be present at the time of diagnosis, with at
least a six-month absence of malignancy during the follow-up period
(9). The patient in the present
case met all of these criteria.
Radiographical examination is an effective method
for the diagnosis of PIOC. PIOC usually exhibits marked variation
in the appearance of its border (17), and thus, it is worth considering as
a differential diagnosis of jaw radiolucency. While panoramic
radiography is useful for obtaining an overall view of the disease,
it may be limited by not providing an evaluation of bone
destructive lesions with a ragged border, the margin, or the degree
of extension and invasion of the surrounding tissue of the tumor
mass. Similarly, panoramic radiography does not sufficiently show
soft masses. In certain cases, PIOC mimicks periapical and
periodontal lesions, which leads to misdiagnosis (9). CT provides detailed information
regarding the location, size and shape of the lesion, and allows
for the visualization of the cited feature as an indicator of the
aggressiveness that is common in cases of potentially malignant
maxillofacial tumors (18,19).
Radical surgery with adequate resection appears to
be the most significant factor in the successful treatment of PIOC
(20). Without an initial biopsy,
the radiolucent lesion may simulate an odontogenic cyst, leading to
the enucleation of the lesion without adequate free margins. Thus,
for the correct treatment, a histopathological diagnosis must be
made during the surgical intervention. For metastatic lymph node
lesions, a neck dissection may be recommended in cases of PIOC
arising from odontogenic cysts. Suspected lymph node metastasis
prior to surgery requires a block dissection with the primary
lesion (6,16). Radiotherapy and chemotherapy are
only used as palliative therapy, or as adjuvant therapy in cases
where nerve infiltration is diagnosed (20). In the present case, the tumor was
found to extend along the inferior alveolar nerve and thus, the
patient received subsequent post-operative radiotherapy.
The present study documents a case of PIOC arising
from an odontogenic cyst. Due to its rarity, it should be
considered as a differential diagnosis of radiolucency of the
jawbone, particularly in older patients with a history of cystic
lesions in the jawbone. Not only is a biopsy recommended, but also
the removal of the entire cyst wall, since malignant changes in the
epithelial lining may not be visible in all sections of the lesion.
The validity of this recommendation is supported by the low rate of
regional lymph node metastasis, with only six reported cases and
the poor survival rate reported for these patients (14). Future studies must strictly adhere
to a well-delineated classification that will thus provide further
comparative and confirmatory data on PIOC.
References
|
1
|
Loos D: Central epidermoid carcinoma of
the jaw. Dtsch Monatschr Zahnheik. 31:3081913.
|
|
2
|
Pindborg J, Kramer I and Torloni H:
Histological Typing of Odontogenic Tumours, Jaw Cysts, and Allied
Lesions. International Histological Classification of Tumours.
World Health Organization; Geneva: pp. 32–34. 1971
|
|
3
|
Elzay RP: Primary intraosseous carcinoma
of the jaws. Review and update of odontogenic carcinomas. Oral Surg
Oral Med Oral Pathol. 54:299–303. 1982.
|
|
4
|
Slootweg PJ and Müller H: Malignant
ameloblastoma or ameloblastic carcinoma. Oral Surg Oral Med Oral
Pathol. 57:168–176. 1984.
|
|
5
|
Waldron CA and Mustoe TA: Primary
intraosseous carcinoma of the mandible with probable origin in an
odontogenic cyst. Oral Surg Oral Med Oral Pathol. 67:716–724.
1989.
|
|
6
|
Müller S and Waldron CA: Primary
intraosseous squamous carcinoma. Report of two cases. Int J Oral
Maxillofac Surg. 20:362–365. 1991.
|
|
7
|
Barnes L, Eveson J, Reichart P and
Sidransky D: World Health Organization classification of tumours:
Pathology and genetics of head and neck tumours. IARC Press; Lyon:
2005
|
|
8
|
Eversole LR: Malignant epithelial
odontogenic tumors. Semin Diagn Pathol. 16:317–324. 1999.
|
|
9
|
Suei Y, Tanimoto K, Taguchi A and Wada T:
Primary intraosseous carcinoma: review of the literature and
diagnostic criteria. J Oral Maxillofac Surg. 52:580–583. 1994.
|
|
10
|
Scheer M, Koch AM, Drebber U and Kübler
AC: Primary intraosseous carcinoma of the jaws arising from an
odontogenic cyst - a case report. J Craniomaxillofac Surg.
32:166–169. 2004.
|
|
11
|
Anneroth G and Hansen LS: Variations in
keratinizing odontogenic cysts and tumors. Oral Surg Oral Med Oral
Pathol. 54:530–546. 1982.
|
|
12
|
Jain M, Mittal S and Gupta DK: Primary
intraosseous squamous cell carcinoma arising in odontogenic cysts:
an insight in pathogenesis. J Oral Maxillofac Surg. 71:e7–e14.
2013.
|
|
13
|
Coussens LM and Werb Z: Inflammation and
cancer. Nature. 420:860–867. 2002.
|
|
14
|
Bodner L, Manor E, Shear M and van der
Waal I: Primary intraosseous squamous cell carcinoma arising in an
odontogenic cyst: a clinicopathologic analysis of 116 reported
cases. J Oral Pathol Med. 40:733–738. 2011.
|
|
15
|
Dimitrakopoulos I, Psomaderis K, Asimaki
A, Papaemanouel S and Karakasis D: Primary de novo intraosseous
carcinoma: report of two cases. J Oral Maxillofac Surg.
63:1227–1230. 2005.
|
|
16
|
Chaisuparat R, Coletti D, Kolokythas A,
Ord RA and Nikitakis NG: Primary intraosseous odontogenic carcinoma
arising in an odontogenic cyst or de novo: a clinicopathologic
study of six new cases. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 101:194–200. 2006.
|
|
17
|
Kaffe I, Ardekian L, Peled M, Machtey E
and Laufer D: Radiological features of primary intra-osseous
carcinoma of the jaws. Analysis of the literature and report of a
new case. Dentomaxillofac Radiol. 27:209–214. 1998.
|
|
18
|
Cavalcanti MG, Veltrini VC, Ruprecht A,
Vincent SD and Robinson RA: Squamous-cell carcinoma arising from an
odontogenic cyst - the importance of computed tomography in the
diagnosis of malignancy. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 100:365–368. 2005.
|
|
19
|
Gallego L, Junquera L, Villarreal P and
Fresno MF: Primary de novo intraosseous carcinoma: report of a new
case. Med Oral Patol Oral Cir Bucal. 15:e48–e51. 2010.
|
|
20
|
Lo Muzio L, Mangini F, De Falco V,
Pennella A and Farronato G: Primary intraosseous carcinoma of the
mandible: a case report. Oral Oncol. 36:305–307. 2000.
|