Introduction
Endometrial stromal sarcoma (ESS) is a rare
malignant tumor of the uterus, which accounts for <2% of all
uterine malignancies and approximately one-fifth of all uterine
sarcomas (1,2). ESS can be classified into low and high
grade according to the tumor characteristics. However, as
high-grade ESS neither shows endometrial stromal differentiation
nor expresses estrogen receptor (ER) or progesterone receptor (PR),
only low-grade ESS is currently considered as ESS, whereas
high-grade ESS is known as undifferentiated endometrial sarcoma
(3). In general, ESS occurs in
perimenopausal females (4). The
standard treatment is surgery, such as total hysterectomy with
bilateral salpingo-oophorectomy. The role of adjuvant treatment,
which includes chemotherapy, radiation therapy and endocrine
therapy, remains controversial. Additionally, the probability of
ESS relapse remains at ~50%.
Due to a significantly improved prognosis compared
to other uterus sarcomas, several cases of fertility-preserving
surgery have been reported for patients with ESS (4–7).
However, the majority were patients at stage I. The current study
presents a case of ESS at stage III that was treated by local mass
resection and uterine reconstruction, and subsequent adjuvant
treatment. To date, the patient has been followed up for 33 months
and there is no sign of recurrence. Patient provided written
informed consent.
Case report
A 19-year-old female (gravida 0, para 0) was
admitted to the Qilu Hospital of Shandong University (Jinan,
Shandong, China) following one day of acute hypogastralgia. A B
ultrasound examination demonstrated a heterogenous echo (9.1×7.5
cm) in the anterior wall of the uterus. The bilateral annex area
was normal. Upon physical examination, tenderness of the lower
abdomin was apparent, but with no rebound tenderness. A rectal
examination indicated an enlarged uterus (pregnant uterus of ~3
months gestation in size) with significant pain in the anterior
wall. No adnexal mass was palpatable. The patient was not sexually
active and presented with a normal menstrual history. The primary
diagnosis was of degeneration of a myoma of the uterus.
Subsequent to two days of adjuvant examinations, a
laparoscopy was performed. Upon surgical exploration, 200 ml of a
faint yellow effusion was found in the pelvic cavity, and an
enlarged uterus (pregnant uterus of ~3 months gestation in size)
and severe adhesion between the anterior wall of the uterus,
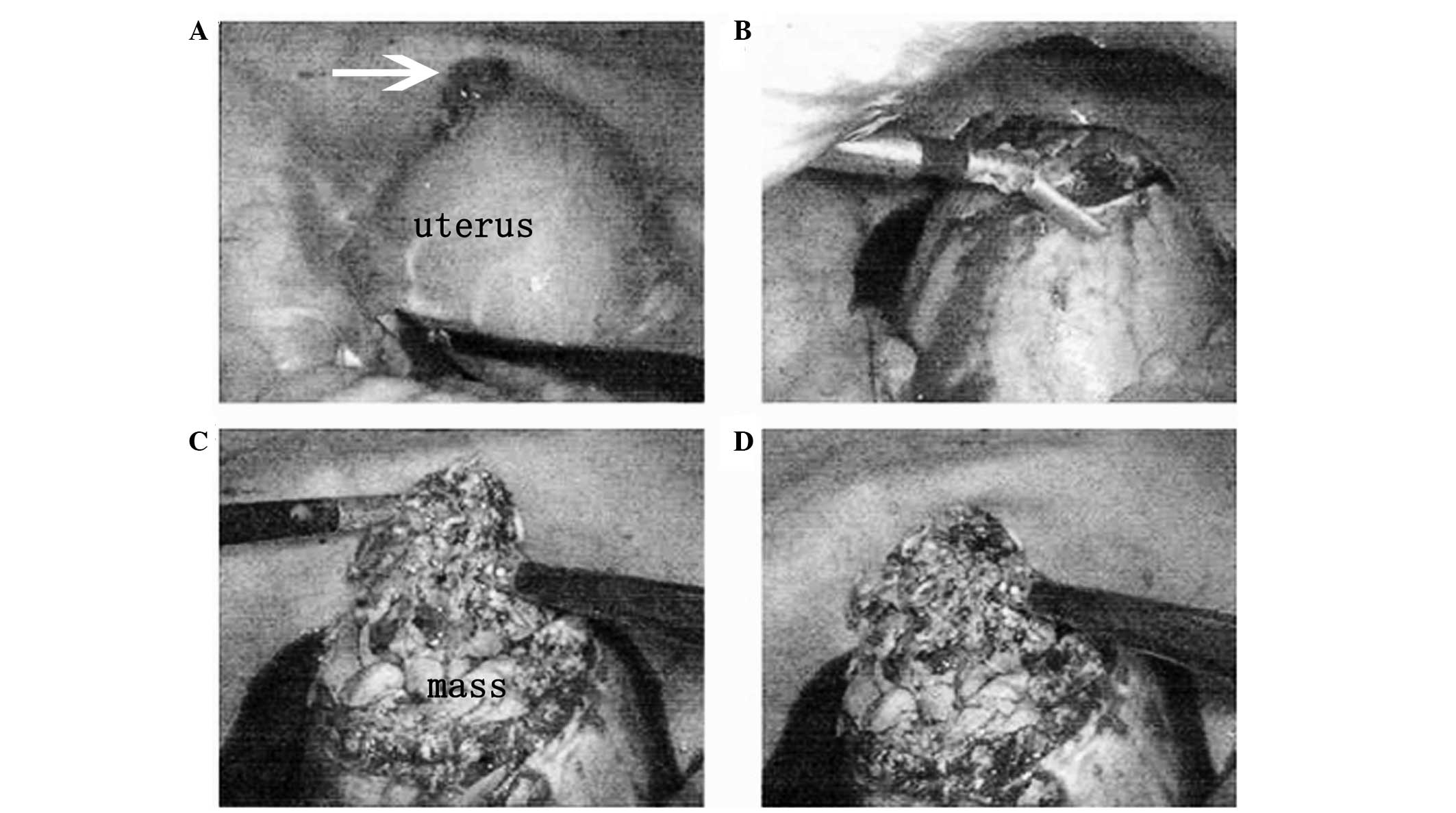
omentum majus and intestinal canal was observed. As shown in
Fig. 1A and B, following the
separation of the adhesion, the anterior wall of the uterus looked
full and convex, and a 2-cm broken sore with endometrioid necrosis
inside existed in the anterior serosa. The ovaries were normal.
Subsequent to resecting the serosa on the anterior wall of the
uterus, an intramural mass was found with unclear margins. The
tumor was fragile, with a yellow and ropy appearance, with
hemorrhage and necrosis inside (Fig. 1C
and D). The mass (10×9 cm) was resected from the anterior wall
of the uterus body, and histological examination of a frozen
section of the resected mass obtained during the surgery indicated
a low-grade ESS. As the patient’s family was adamant with regard to
preserving the fertility of the patient, a decision was made to
preserve the uterus, and a subsequent laparotomy was performed. A
fusiform incision of the myometrium was created ~1 cm lateral to
the former uterus incision. Total resection of the mass was
achieved and the uterus was reconstructed. A 5×4-cm sheet and
thickened region of the intestinal canal was adherent to the
anterior wall of the uterus, with a 2×1-cm hemorrhagic and necrotic
nodule on the surface. Therefore, the surface nodule and partial
adhesive omentum majus were removed. No other abnormalities were
found during the following abdominal and pelvic exploration.
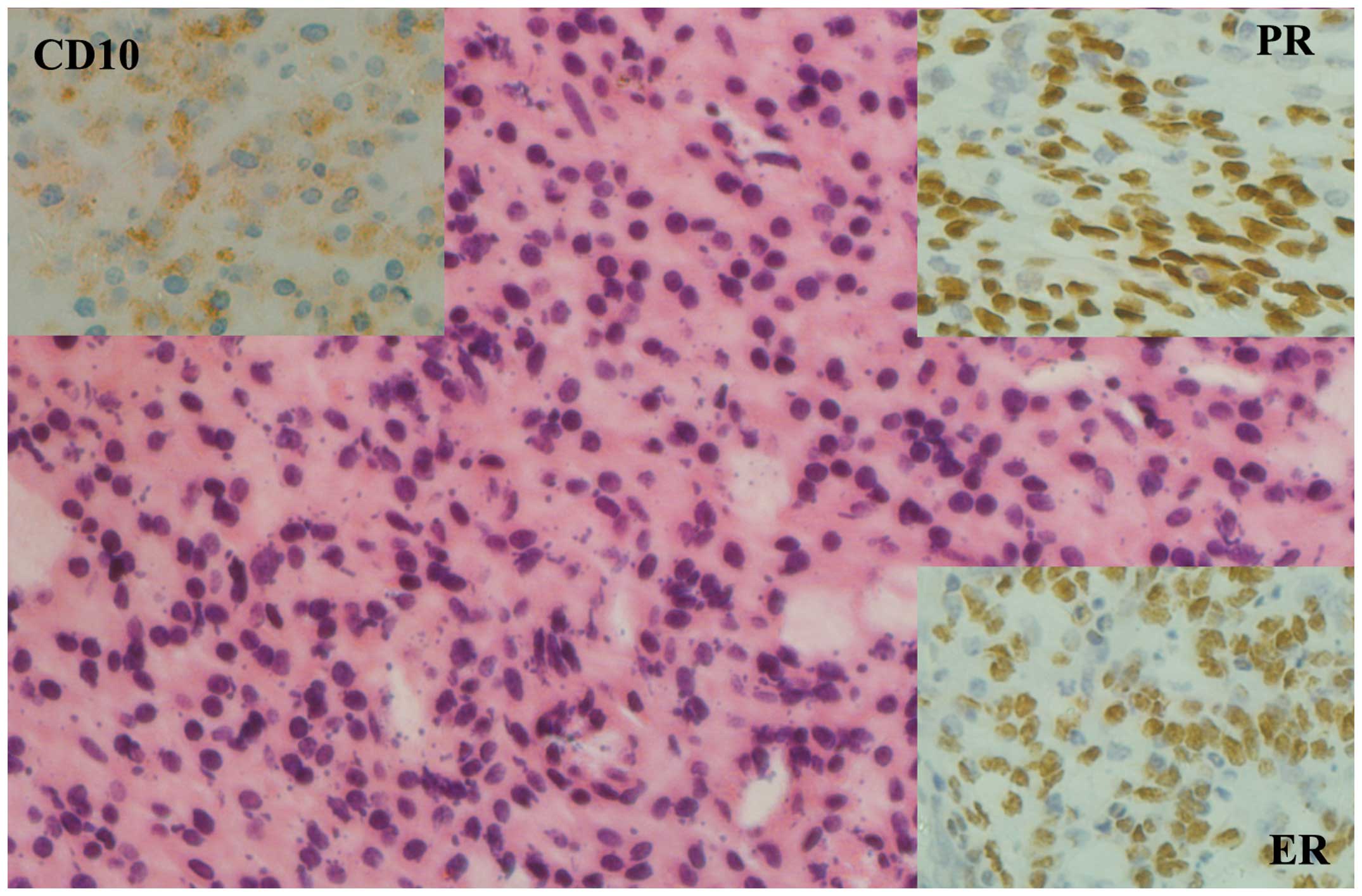
The post-operative pathohistological analysis of a
paraffin-embedded section showed a low-grade ESS in accordance with
the previous pathological diagnosis of the frozen section. Nodules
from the surface of the intestine had a small quantity of
endometrial stromal sarcoma cells. No sarcoma cells were found in
the omentum majus. The staining intensity was defined as follows:
−, negative; +, weak; ++, moderate; and +++, strong. As shown in
Fig. 2, the immunohistochemistry
assay showed the following results: Cluster of differentiation
(CD)10(+), α-inhibin(−), CD34(−), smooth muscle actin(+/−), ER(++)
and PR(+++).
Post-operatively, the patient was administered 250
mg medroxyprogesterone acetate daily for 1 year to inhibit tumor
recurrence. Sequential clinical examinations and radiographical
studies have been used in post-operative surveillance, and a
33-month follow-up examination showed no signs of recurrent
disease.
Discussion
ESS is divided into two subtypes, high-grade ESS and
low-grade ESS, with totally different prognoses. High-grade ESS has
a relatively poor prognosis, whereas the prognosis of low-grade ESS
is relatively favorable. The significant factors affecting the
treatment outcome include clinical stage, histological subtype,
cell differential degree, tumor size and expression of sexual
hormone receptors (8). The common
clinical manifestation is abnormal vaginal bleeding. In the current
case, the patient presented with acute hypogastralgia as the
initial symptom, which was believed to be caused by the large tumor
size and uterus perforation on the basis of previous surgical
situations.
The main surgery for ESS is total abdominal
hysterectomy with adnexectomy. However, with regard to the surgical
options for young patients, further studies are required to analyze
the feasibility of fertility preservation. Several cases have
previously reported that fertility-preserving treatment for ESS is
feasible (4–7). However, the majority of these patients
were at stage I. In the present case, the local mass was as large
as 10 cm with a broken sore on the surface, and the adhesion with
the omentum majus and intestine was confirmed to exhibit
metastasis. Taking all these facts into account, the tumor was
classified as clinical stage III. As the patient was only
19-years-old, a local mass resection and uterine reconstruction
were performed to preserve fertility. Post-operatively, endocrine
treatment was commenced. To date, the patient is well without any
evidence of recurrence following a 33-month follow-up period. It
has been reported that the median time to recurrence is 65 months
for stage I ESS and 9 months for stages III–IV (9). Therefore, follow-up is necessary for
those patients with ESS who have undergone fertility-preserving
treatment in order to identify and treat recurrence at an early
stage. To date, there have been three reported cases of patients
with ESS who experienced a successful pregnancy following
fertility-preserving treatment (4–6).
Koskas et al reported the case of a 34-year-old female
treated conservatively for low-grade ESS (LGESS) who conceived
rapidly following hysteroscopic resection of the tumor. However, in
the postpartum period, pelvic pain motivated a laparoscopic
exploration, which revealed severe peritoneal recurrence (6). It is postulated that changes in
hormone levels during pregnancy enhanced the process of ESS. This
case indicated that pregnancy may contribute to the development of
LGESS. Therefore, the decision to preserve fertility and undergo
pregnancy should be taken into consideration.
Adjuvant treatments for LGESS consist of
chemotherapy, radiotherapy and endocrine therapy. Based on
experience from clinical practice that has shown that LGESS is
generally a hormonally-sensitive tumor with indolent growth,
adjuvant progestin treatment is currently the most effective
treatment for treatment of LGESS and should be considered as a
routine adjuvant therapy for the treatment of ESS or recurrent ESS,
particularly for those with strong positivity for PR staining
(10,11). The present study patient with stage
III ESS showed no signs of recurrence following conservative
treatment, including fertility-preserving surgery and high-dose
progestin treatment. Additionally, it is known that adjuvant
aromatase inhibitors may also aid in the treatment of ESS, and that
the combined application of progestin and aromatase inhibitors may
have future development potential for ESS treatment; these topics
have already been the subject of studies and reviews (12–14).
As the prognosis of LGESS is usually favorable,
conservative surgery is a logical intervention for young
nulliparous females. However, the significant prognostic factors
affecting treatment must be taken into consideration. Conservative
treatment for LGESS has not been experienced a great deal
clinically and is problematic, as no randomized trials are
available to offer a reliable theoretical basis. Overall, the
decision of whether to administer conservative management for young
females with LGESS should be taken according to the individual
clinical condition, and further studies are required.
References
|
1
|
Nam JH: Surgical treatment of uterine
sarcoma. Best Pract Res Clin Obstet Gynaecol. 25:751–760. 2011.
|
|
2
|
Tropé CG, Abeler VM and Kristensen GB:
Diagnosis and treatment of sarcoma of the uterus. A review. Acta
Oncol. 51:694–705. 2012.
|
|
3
|
Amant F, Vergote I and Moerman P: The
classification of a uterine sarcoma as ‘high-grade endometrial
stromal sarcoma’ should be abandoned. Gynecol Oncol. 95:412–413.
2004.
|
|
4
|
Yan L, Tian Y, Fu Y and Zhao X: Successful
pregnancy after fertility-preserving surgery for endometrial
stromal sarcoma. Fertil Steril. 93:269.e1–269.e3. 2010.
|
|
5
|
Delaney AA, Gubbels AL, Remmenga S, Tomich
P and Molpus K: Successful pregnancy after fertility-sparing local
resection and uterine reconstruction for low-grade endometrial
stromal sarcoma. Obstet Gynecol. 120:486–489. 2012.
|
|
6
|
Koskas M, Morice P, Yazbeck C, Duvillard
P, Walker F and Madelenat P: Conservative management of low-grade
endometrial stromal sarcoma followed by pregnancy and severe
recurrence. Anticancer Res. 29:4147–4150. 2009.
|
|
7
|
Dong R, Pang Y, Mao H, Yang N and Liu P:
Successful pregnancy following conservative management of low-grade
endometrial stromal sarcoma: A case report. Oncol Lett.
7:1039–1042. 2014.
|
|
8
|
Yalman D, Ozsaran Z, Baltalarli B, Demir
O, Ozdemir N and Aras A: Results of postoperative radiotherapy in
the treatment of uterine sarcomas: a retrospective analysis of 46
patients. Eur J Gynaecol Oncol. 29:46–51. 2008.
|
|
9
|
Chang KL, Crabtree GS, Lim-Tan SK, Kempson
RL and Hendrickson MR: Primary uterine endometrial stromal
neoplasms. A clinicopathologic study of 117 cases. Am J Surg
Pathol. 14:415–438. 1990.
|
|
10
|
Amant F, Coosemans A, Debiec-Rychter M,
Timmerman D and Vergote I: Clinical management of uterine sarcomas.
Lancet Oncol. 10:1188–1198. 2009.
|
|
11
|
Chu MC, Mor G, Lim C, Zheng W, Parkash V
and Schwartz PE: Low-grade endometrial stromal sarcoma: hormonal
aspects. Gynecol Oncol. 90:170–176. 2003.
|
|
12
|
Sylvestre VT and Dunton CJ: Treatment of
recurrent endometrial stromal sarcoma with letrozole: a case report
and literature review. Horm Cancer. 1:112–115. 2010.
|
|
13
|
Leiser AL, Hamid AM and Blanchard R:
Recurrence of prolactin-producing endometrial stromal sarcoma with
sex-cord stromal component treated with progestin and aromatase
inhibitor. Gynecol Oncol. 94:567–571. 2004.
|
|
14
|
Spano JP, Soria JC, Kambouchner M, et al:
Long-term survival of patients given hormonal therapy for
metastatic endometrial stromal sarcoma. Med Oncol. 20:87–93.
2003.
|