Introduction
Colonic lipomas are an uncommon type of benign
gastrointestinal tumor. Although colonic lipomas are generally
asymptomatic, when the colonic lipoma measures >2 cm, certain
symptoms, such as abdominal pain, change in bowel habits, bleeding
and a mass that presents as a rectal prolapse may be observed
(1,2). While colonic lipomas are often
observed in the caecum and ascending colon, they may also be
observed in the transverse, descending, and sigmoid colon and in
the rectum (3). In the current
study, the case of a patient exhibiting a giant, rarely observed
lipoma of the sigmoid colon is presented with a description of its
external excision. Patient provided written informed consent.
Case report
A 39-year-old male patient was admitted to our
emergency clinic with a mass protruding from the anal canal. Other
symptoms included anal pain and rectal bleeding. During the
physical examination, the prolapsed mass was spontaneously reduced
through the rectum. The mass was initially diagnosed as a rectal
prolapse and the patient was transferred to the Department of
General Surgery, Buyukcekmece State Hospital (Istanbul, Turkey) in
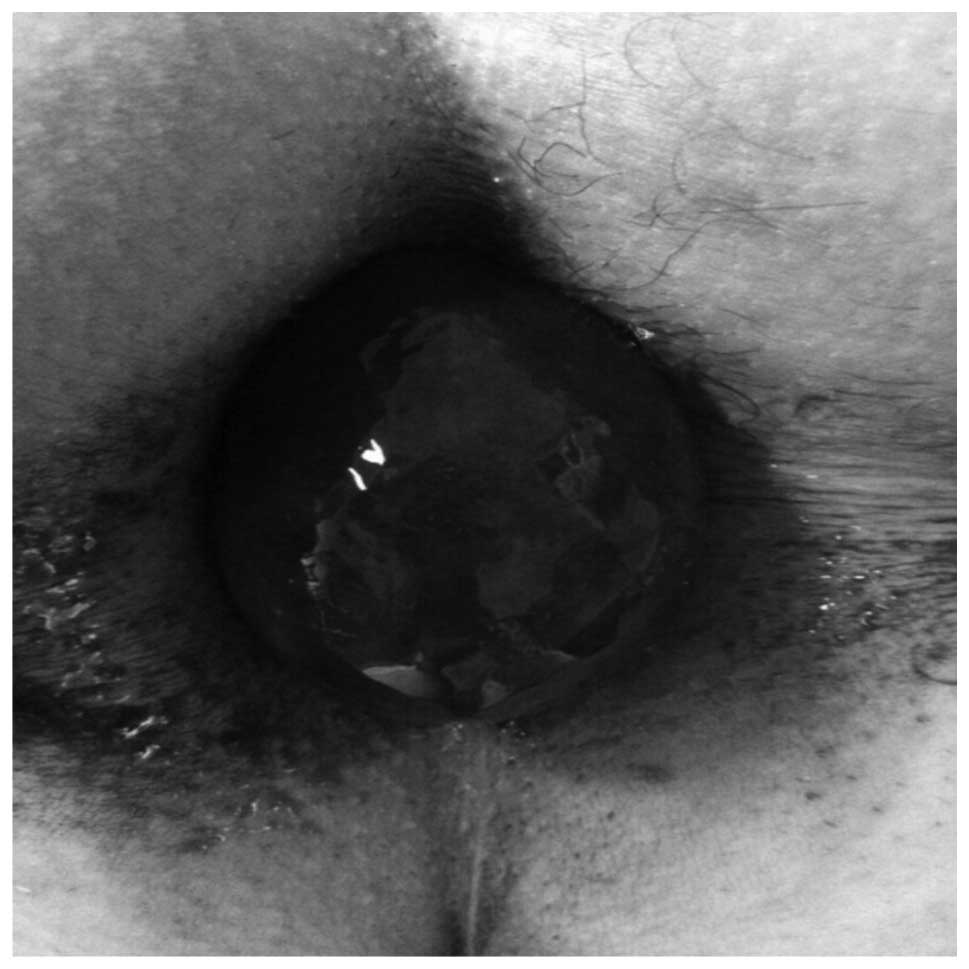
June 2012. During the physical examination, the mass was forced out
from the anal canal while the patient performed the Valsalva
maneuver under light sedation. The mass (size, 10×8 cm) had a shiny
surface and hyperemia was detected during the physical inspection
(Fig. 1). A smooth-surfaced soft
tissue with a pedicle (diameter, 3 cm) was detected on palpation.
The mass was reduced manually by gentally pushing it through the
anus. The routine laboratory examination results were normal and no
abnormalities were noted in the patient’s background or family
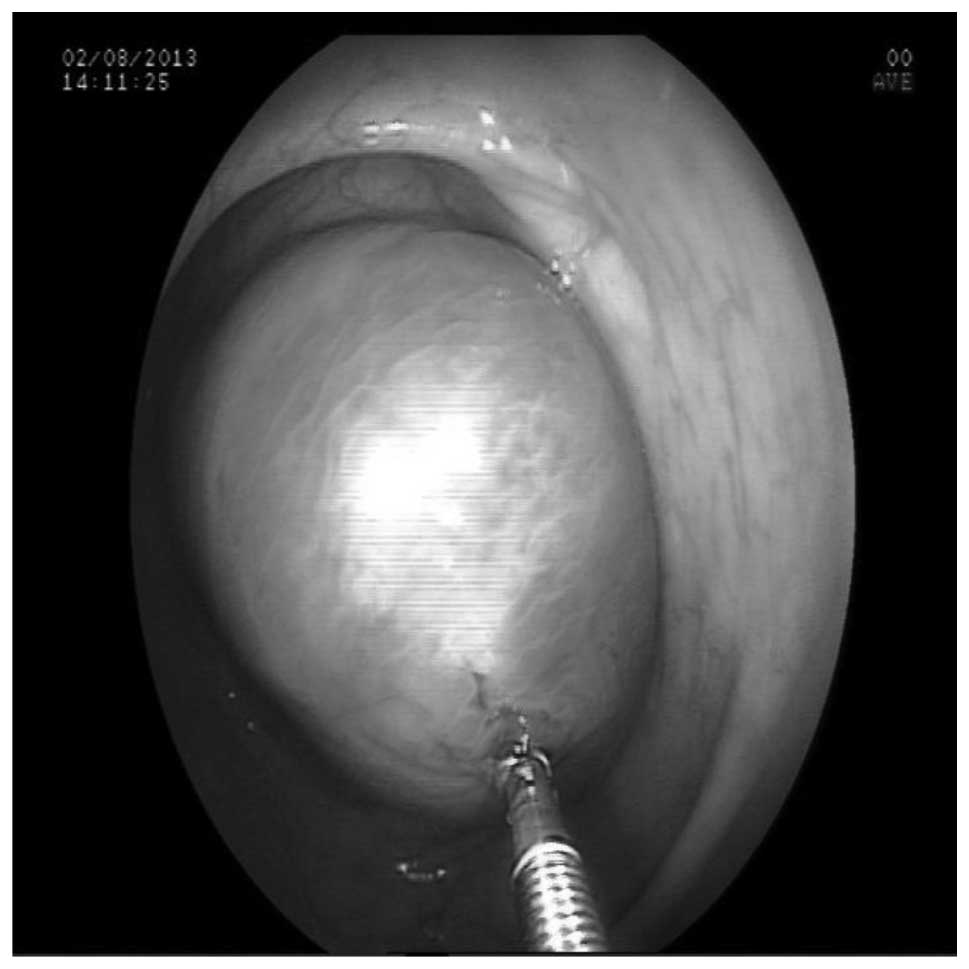
history. A colonoscopy was performed, and at the 35th cm of the
anal canal, a mobile, shiny, hyperemic, smooth-surfaced, giant
polyp (size, 10×8×7.5 cm), which was covered by a mucosa and a
pedicle (diameter, 3 cm) was occluding almost all of the lumen
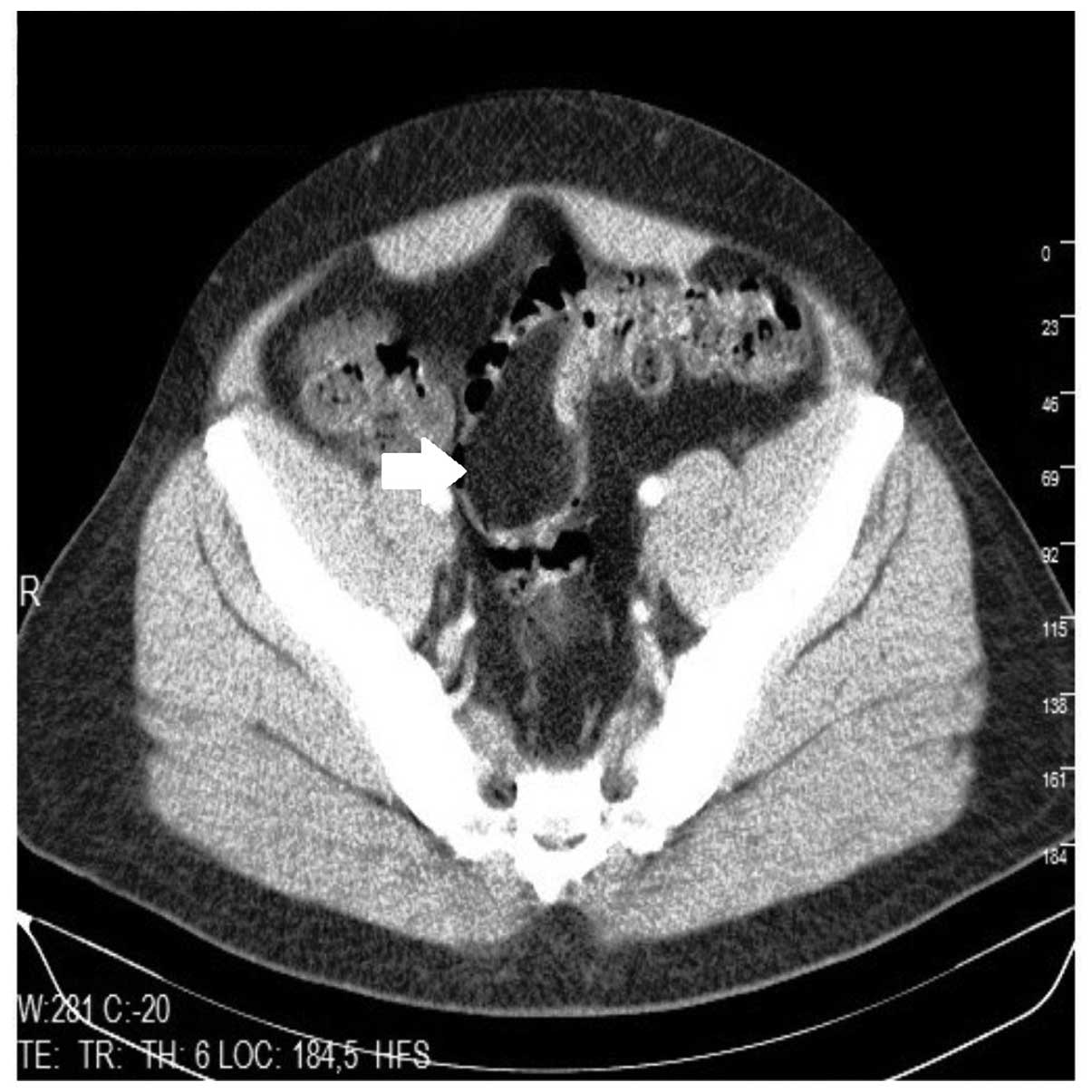
(Fig. 2). At the sigmoid colon, an
8×6-cm fat-density lesion (representing the lipoma) was observed
via abdominal computed tomography (CT; Fig. 3). An endoscopic polypectomy was
attempted, however, it was unsuccessful due to the size of the
lesion measuring ~10 cm in its maximum diameter making it difficult
to manipulate the lesion. As a result, an external excision was
scheduled. Under light sedation the patient performed the Valsalva
maneuver and the mass was forced out from the anal canal. In order
to perform an easy removal of the mass from the anus, the pedicle
at the exit of the anal canal was tied and the patient’s depth of
anesthesia was strengthened. The mass was pulled out, and the
distal end of the pedicle was tied and excised. The resected
specimen underwent histopathological examination (Fig. 4), which revealed the mass to be a
submucosal lipoma with a normal mucosa. The patient was discharged
on the first postoperative day on which he did not experience any
complications. The colonoscopy, which was performed two weeks
later, was considered to be normal.
Discussion
Colonic lipomas are rarely observed, and are an
asymptomatic, benign, submucosal and nonepithelial type of
gastrointestinal tumor. In general, this type of lipoma is <2
cm, sessile or pedunculated and often located in the right colon.
These lesions are more common in women, observed in the fifth and
sixth decades of life and are usually detected during an autopsy,
colonoscopy or surgery (2). Lipomas
that are >2 cm may be symptomatic, however, in cases where the
lipoma is large, it may result in abdominal pain, change in bowel
habits, intestinal obstruction and rectal bleeding (4,5). The
current case is considered to be rare due to the location of the
lesion, its size and the symptom of external prolapse.
Colonic lipomas are generally submucosal lesions
with a smooth mucosal surface, which are composed of lobular
adipose tissues (2). The
colonoscopic properties are distinguished by the lesion’s soft and
smooth surface, which is covered by a yellow-colored mucosa
(6). Typical characteristics of
this type of lipoma include tenting of the tissue (when the mucosa
covering the lesion is removed using forceps), collapse of the
lesion when pressure is applied to it, in addition to
yellow-colored adipose tissue, which may be observed during biopsy
(1,2,7). The
colonoscopy in the present study revealed a giant polyp that was
mobile, shiny, hyperemic, smooth-surfaced, covered by a mucosa and
exhibited the abovementioned characteristics. The mass measured
10×8×7.5 cm and the pedicle diameter was 3 cm, which occluded
almost all of the lumen. Endoscopic biopsies for colonic lipomas
provide only a limited diagnosis, and the pathology results are
generally normal or demonstrate an ulcerated mucosa (2). A biopsy was not necessary in the
present case as the mass was externally prolapsed.
Imaging techniques facilitate diagnosis; however, as
the results are not definitive, the final diagnosis may only be
obtained following excision of the tissue (1,2,6,8).
A smooth oval filling defect may be observed via barium X-rays,
while non-vascular, hyperechoic, submucosal lesions that are
observed using endoscopic ultrasonography may supplement the
diagnosis, however, are not specific to the diagnosis (8,9). For
large colonic lipomas (>2 cm), CT is able to detect masses by
demonstrating sharp margins in the homogeneous fat density and
magnetic resonance imaging distinguishes lesions in the adipose
tissue intensity (6,8). In the present case, CT was adopted as
the imaging method and an 8×6-cm fat-density lesion (representing
the lipoma) was observed in the sigmoid colon.
Endoscopic polypectomy, local excision,
hemicolectomy, or segmental resections are performed for the
treatment of colonic lipomas, depending on the popularity and
reliability of the particular technique. Endoscopic polypectomy is
the preferred treatment strategy, particularly for small lipomas
(<2 cm). Although, the risk of bleeding and perforation is high
when performing an endoscopic polypectomy on polyps >2 cm
(4,9). Kim et al (4) demonstrated that it was possible to
excise lipomas <3.8 cm, following a submucosal saline injection,
without the patient experiencing any complications. Jiang et
al (2) proposed that surgical
procedures are required in the following instances: i) when the
lipoma is sessile or has a pedicle >4 cm; ii) the lipoma is
malignant; iii) the patient exhibits symptoms, such as
intussusception; iv) a muscular layer or serosal attachment is
present; or v) the lesion cannot be removed by colonoscopy. There
are various surgical procedures that may be conducted for lipomas,
including hemicolectomy, segmental resection or local excision
(8). In the present case, since the
mass occurred as an external prolapse and had a pedicle, external
resection was performed to obtain the final diagnosis, thus, no
major surgical procedure was required.
In conclusion, colonic lipoma should be considered
in the differential diagnosis of anorectal diseases, such as
hemorrhoids and rectal prolapse. An external excision may be
performed for the treatment of a prolapsed colonic lipoma, as this
procedure is considered to be safe and reliable. Furthermore, it
may be performed as an alternative to major surgery in certain
patients.
References
|
1
|
Mnif L, Amouri A, Masmoudi MA, Mezghanni
A, Gouiaa N, Boudawara T and Tahri N: Giant lipoma of the
transverse colon: a case report and review of the literature. Tunis
Med. 87:398–402. 2009.
|
|
2
|
Jiang L, Jiang LS, Li FY, Ye H, Li N,
Cheng NS and Zhou Y: Giant submucosal lipoma located in the
descending colon: a case report and review of the literature. World
J Gastroenterol. 13:5664–5667. 2007.
|
|
3
|
Mayo CW, Pagtalunan RJ and Brown DJ:
Lipoma of the alimentary tract. Surgery. 53:598–603. 1962.
|
|
4
|
Kim CY, Bandres D, Tio TL, Benjamin SB and
Al-Kawas FH: Endoscopic removal of large colonic lipomas.
Gastrointest Endosc. 55:929–931. 2002.
|
|
5
|
Tony J, Saji S, Sandesh K, Sunilkumar K,
Ramachandran TM and Thomas V: External resection of a giant sigmoid
lipoma causing colonic intussusception and prolapse through the
anal canal. Trop Gastroenterol. 28:127–128. 2007.
|
|
6
|
Zhang X, Ouyang J and Kim YD: Large
ulcerated cecal lipoma mimicking malignancy. World J Gastrointest
Oncol. 2:304–306. 2010.
|
|
7
|
Martin P, Sklow B and Adler DG: Large
colonic lipoma mimicking colon cancer and causing colonic
intussusception. Dig Dis Sci. 53:2826–2827. 2008.
|
|
8
|
Arora R, Kumar A and Bansal V: Giant
rectal lipoma. Abdom Imaging. 36:545–547. 2011.
|
|
9
|
Ryan J, Martin JE and Pollock DJ: Fatty
tumours of the large intestine: a clinicopathological review of 13
cases. Br J Surg. 76:793–796. 1989.
|