Introduction
Secretory breast carcinoma (SBC) is one of the
rarest types of breast cancer, accounting for <1% of all breast
cancers. It was first reported as ‘juvenile breast carcinoma’ by
McDivitt and Stewart in 1966 (1).
Subsequently, additional cases in children (2–6) and
adults (7–12) have been described. The original term
was replaced by the more appropriate ‘secretory breast cancer’ in
the 1980s.
The typical clinical presentation of SBC is a
slow-growing, painless, well-circumscribed, mobile, palpable mass
occurring anywhere in the breast. SBC ultrasound appearance shows a
solitary, microlobulated, hypoechoic mass resembling a benign
lesion, such as a fibroadenoma or other well-circumscribed
carcinomas (13). There are, at
present, no consensus guidelines for the treatment of SBC. Although
recommendations vary among authors, surgical excision is the
primary mode of treatment for secretory carcinoma. However,
preservation of pubertal breast tissue is important to ensure
correct breast development; although, this is not always possible
due to the location of the tumor. Occasionally, mastectomy is
required, and this may cause complex psychosocial difficulties in
the lives of adolescent females (14,15).
The present study describes the case of a 12-year-old female with
SBC and highlights the treatment options available for children
with this tumor type. Patient provided written informed
consent.
Case report
In June 2012, a 12-year-old female presented to the
Department of Breast Cancer Surgery, Tangshan People’s Hospital
(Tangshan, China) with a painless lump close to the left breast
areola. The patient had first noticed the lump two months prior to
presentation, during which time there had been no significant
increase in the sixe of the lump. There was no history of local
trauma, and no family history of relevant malignancy. Examination
revealed a 4.0×3.0-cm, firm, well-circumscribed, mobile mass
located eccentrically beside the areola at the 3 o’clock position.
No nipple discharge or inversion were observed, and no clinical
alterations were found in the ipsi- or contralateral lymph nodes.
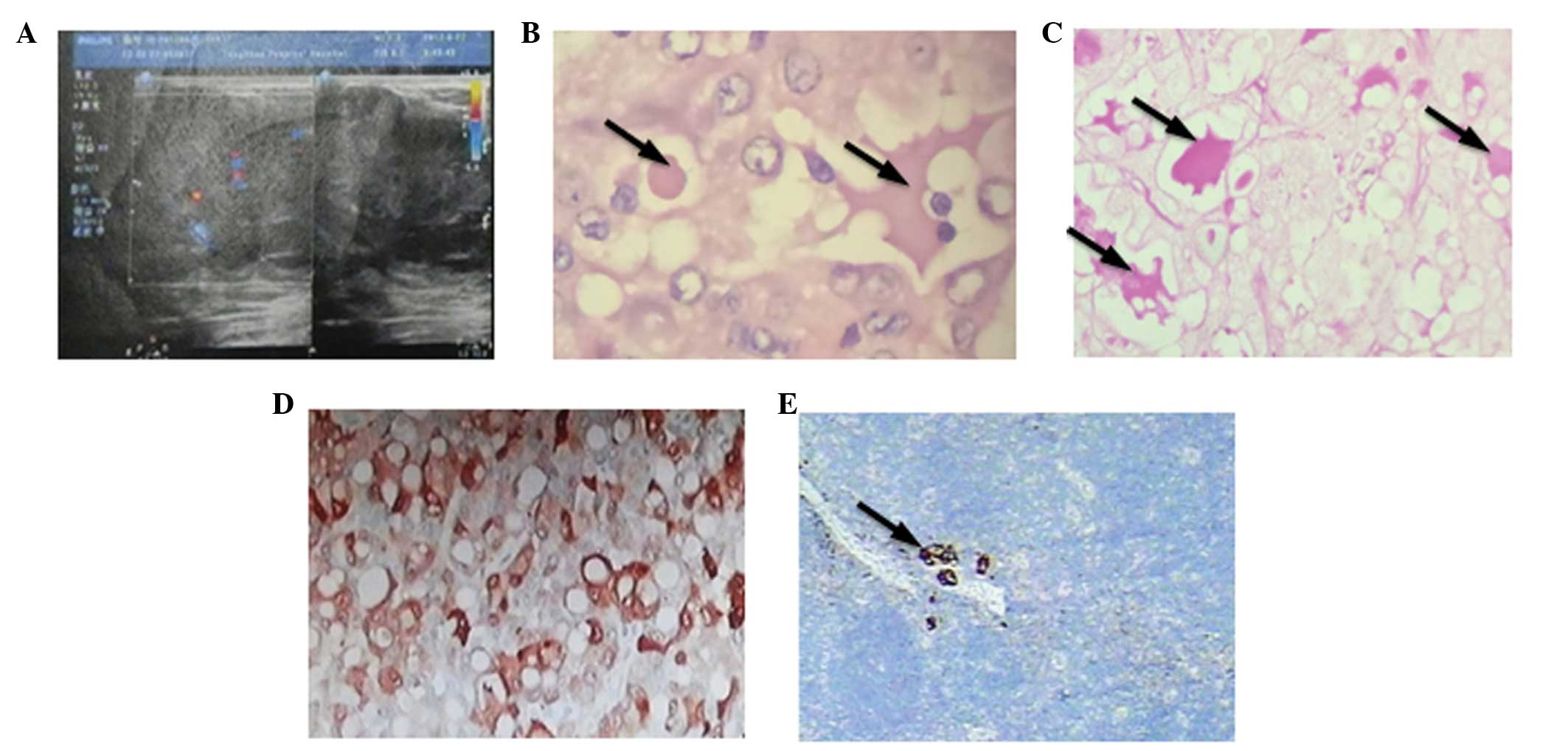
Ultrasound examination of the breast showed a well-defined
hypoechoic nodule measuring 4.0×3.9×2.5 cm in size, without
calcification or evidence of invasion (Fig. 1A). The mass was considered as benign
in appearance and diagnosed as a fibroadenoma of the breast.
Not only for this reason, but also at the patient’s
request, core biopsy of the tumor was not performed and the patient
therefore immediately underwent surgical removal of the nodule
under local anesthetic. The macroscopic examination of breast
operative specimens revealed the presence of a nodule measuring
4.0×4.0×2.9 cm, and the lesion was void of an intact capsule. The
cut surface appeared solid and gray-white. Microscopic analysis of
hematoxylin and eosin-stained sections showed tumor cells arranged
in lobules separated by dense fibrous septa (Fig. 1B). The lobules showed a
tubuloalveolar and glandular pattern with abundant secretion, which
is usually pale pink (16). A
honeycomb pattern was also observed. The tumor consisted of cells
with minimal to middle nuclear atypia with abundant slightly
basophil cytoplasm, as well as intracytoplasmic vacuoles. The
presence of secretions which are strongly periodic
acid-Schiff-positive are a hallmark of SBC (Fig. 1C) (16). No nuclear division was observed in
the present case. Immunohistochemistry was also performed,
revealing that the tumor cells were negative for estrogen receptor
(ER), progesterone receptor (PR) and human epidermal growth factor
receptor-2, and showed positive staining for S100 (Fig. 1D). A diagnosis of secretory breast
cancer was then established. Axillary sentinel lymph node (SLN)
biopsy was also performed. The SLN was found to contain isolated
tumor cells (Fig. 1E), and
according to the NCCN Clinical Practice Guidelines in Oncology of
Breast Cancer (17), cases of no
metastases can be considered as SLN. Therefore, the patient could
avoid complete axillary dissection.
Since the mass was close to the breast areola and
the patient was younger than 35 years old, the patient seemed
better to receive a radical mastectomy. However, the patient wished
to undergo a partial resection for the tumor, rather than the
radical mastectomy. The breast magnetic resonance imaging revealed
no multiple lesions and the patient subsequently underwent a left
breast conservative surgery. The histopathology of operative
specimens revealed no evidence of residual neoplasia within the
breast. After multidisciplinary consultation (including with a
pediatric oncologist), adjuvant chemotherapy was administered to
the patient. This comprised doxorubicin (60 mg/m2, IV)
and cyclophosphamide (600 mg/m2, IV) on day one, cycled
every 21 days for four cycles, followed by docetaxel (100
mg/m2, IV) on day one, cycled every 21 days for four
cycles. No radiotherapy treatment was performed.
Periodic follow-up examinations after completion of
the surgical and chemotherapeutic treatment have shown no evidence
of either local regression or distant metastases to date and, one
year later, the patient remains free of disease.
Discussion
Since very few cases of SBC have been described in
the literature, it is imperative to report any new cases observed
in order to establish the most suitable therapeutic approach. SBC
has a better prognosis than the more usual form of ductal carcinoma
(18). There is no consensus of
opinion as to how SBC should be treated, as there are so few case
reports of SBC in the literature (19). However, surgery is the primary mode
of treatment for this pathology. A previous study described the
case of a 50-year-old woman who had undergone a breast conservative
surgery for SBC (14). However,
there are few case reports on conservative surgery treatment in
adolescents, according to Costa’s study, as for children, local
excision with sentinel lymph node mapping is the preferred initial
treatment (14). This unusual
breast cancer subtype generally has a favorable prognosis, although
several cases have been described in adults with increased
aggressiveness and a risk of metastases. The clinical course of SBC
is characterized by a tendency for late local recurrence and
prolonged survival, even with lymph node metastases, and mortality
due to metastatic secretory carcinoma is extremely rare (20). The present study describes a case
whereby breast-conserving therapy was used to treat secretory
breast cancer in a 12-year-old female. The lack of secure data
regarding the potential of secretory carcinoma to bring about local
relapse leads us to the conclusion that a conventional,
conservative approach, such as quadrantectomy followed by
radiotherapy and/or chemotherapy, used for all other types of
infiltrating breast carcinomas, should also be used for this type
of tumor (20). There is
insufficient evidence to recommend post-operative radiotherapy
and/or chemotherapy for this pathology (9,21–23).
However, in one case report, a patient with a single positive lymph
node responded to traditional chemotherapy consisting of six cycles
of cyclophosphamide, methotrexate and 5-fluorouracil, with no
evidence of local or distant disease after seven years of follow-up
(24). Although chemotherapy can
cause potential reproductive risks, according to NCCN guidelines,
even favourable histologies of breast cancer which are ER- and
PR-negative should be treated as typical breast cancer. In the
present case, considering the mass was 4.0 cm in diameter, adjuvant
chemotherapy was administered, consisting of doxorubicin and
cyclophophamide, followed by docetaxel. In consideration of no
pronounced evidence demonstrates that ovarian suppression or other
interventions decrease the toxicity of cytotoxic chemotherapy on
the premenopausal ovary (25), no
gonadotrophin-releasing hormone agonist treatment was administered.
Postoperative radiotherapy should be proposed following
conservative surgery in adult patients, but is not advised for
children due to the possible secondary effects, such as fibrosis of
the lung, rib damage and the consequent asymmetry of the rib cage,
as well as a risk for future development of neoplasia (22,26).
Due to this, no radiotherapy treatment was performed in the present
case.
As for adolescents, fibroadenomata predominate
(27); in the younger age group,
more insidious pathology must be excluded. As studies in the
literature have shown optimal results regarding the value of
bioptic staging of the sentinel lymph gland (24,28,29),
we believe that this treatment choice is particularly valid in
order to avoid axillary lymphadenectomy. Given the uncertainty
regarding the latency and dormancy of the tumor, close clinical
follow-up of the present patient for an indefinite period was
considered mandatory. We propose that it is useful to report every
case of this rare tumor, in order to increase the knowledge of its
biology and management.
Abbreviations:
|
SBC
|
secretory breast cancer
|
|
SLN
|
sentinel lymph node
|
|
ER
|
estrogen receptor
|
|
PR
|
progesterone receptor
|
References
|
1
|
McDivitt RW and Stewart FW: Breast
carcinoma in children. JAMA. 195:338–390. 1966.
|
|
2
|
Oberman HA and Stephens PJ: Carcinoma of
the breast in childhood. Cancer. 30:470–474. 1972.
|
|
3
|
Byrne MP, Fahey MM and Gooselaw JG: Breast
cancer with axillary metastasis in an eight and one-half-year-old
girl. Cancer. 31:726–728. 1973.
|
|
4
|
Masse SR, Rioux A and Beauchesne C:
Juvenile carcinoma the breast. Hum Pathol. 12:1044–1046. 1981.
|
|
5
|
Karl SR, Ballantine TVN and Zaino R:
Juvenile secretory carcinoma of the breast. J Pediatr Surg.
20:368–371. 1985.
|
|
6
|
Fergunson TB Jr, Mc Carty KS Jr and
Filston HC: Juvenile secretory carcinoma and juvenile
papillomatosis: diagnosis and treatment. J Pediatr Surg.
22:637–640. 1987.
|
|
7
|
Tavassoli FA and Norris HJ: Secretory
carcinoma of the breast. Cancer. 45:2404–2413. 1980.
|
|
8
|
Oberman HA: Secretory carcinoma of the
breast in adults. Am J Surg Pathol. 4:465–470. 1980.
|
|
9
|
Akhtar M, Robinson C, Ali MA and Godwin
JT: Secretory carcinoma of the breast in adults. Light and electron
microscipic study of three cases with review of the literature.
Cancer. 51:2245–2254. 1983.
|
|
10
|
Krausz T, Jenkins D, Grontoft O, Pollock
DJ and Azzopardi JG: Secretory carcinoma of the breast in adults:
emphasis on late recurrence and metastasis. Histopathology.
14:25–36. 1989.
|
|
11
|
Rosen PP and Cranor ML: Secretory
carcinoma of the breast. Arch Pathol Lab Med. 115:141–144.
1991.
|
|
12
|
Mies C: Recurrent secretory carcinoma in
residual mammary tissue after mastectomy. Am J Surg Pathol.
17:715–721. 1993.
|
|
13
|
Vasudev P and Onuma K: Secretory breast
carcinoma: unique, triple-negative carcinoma with a favorable
prognosis and characteristic molecular expression. Arch Pathol Lab
Med. 135:1606–1610. 2011.
|
|
14
|
Costa NM, Rodrigues H, Pereira H, Pardal F
and Matos E: Secretory breast carcinoma - case report and review of
the medical literature. Breast. 13:353–355. 2004.
|
|
15
|
Tixier H, Picard A, Guiu S, Coudert B,
Loustalot C, Depret O, Arnold l and Cuisenier J: Long-term
recurrence of secretory breast carcinoma with metastatic sentinel
lymph nodes. Arch Gynecol Obstet. 238(Suppl 1): S77–S78
|
|
16
|
Rosen PP: Secretory carcinoma. Rosen’s
Breast Pathology. Lippincott Williams & Wilkins; Philadelphia,
PA: pp. 563–570. 2008
|
|
17
|
Francissen CM, van la Parra RF, Mulder AH,
et al: Evaluation of the benefit of routine intraoperative frozen
section analysis of sentinel lymph nodes in breast cancer. ISRN
Oncol. 2013:8437932013.
|
|
18
|
Gallager HS: Pathologic types of breast
cancer: their prognoses. Cancer. 53:623–629. 1984.
|
|
19
|
Arce C, Cortes-Padilla D, Huntsman DG,
Miller MA, Dueñnas-Gonzales A, Alvarado A, Pérez V, Gallardo-Rincón
D and Lara-Medina F: Secretory carcinoma of the breast containing
the ETV6-NTRK3 fusion gene in a male: case report and review of the
literature. World J Surg Oncol. 3:352005.
|
|
20
|
Kavalakat AJ, Covilakam RK and Culas TB:
Secretory carcinoma of breast in a 17-year-old male. Worl J Surg
Oncol. 2:17–22. 2004.
|
|
21
|
Herz H, Cooke B and Goldstein D:
Metastatic secretory breast cancer. Non-responsiveness to
chemotherapy: case report and review of the literature. Ann Oncol.
11:1343–1347. 2000.
|
|
22
|
Szántó J, András C, Tsakiris J, Gomba S,
Szentirmay Z, Bánlaki S, Szilágyi I, Kiss C, Antall P, Horváth A,
Lengyel L and Castiglione-Gertsch M: Secretory breast cancer in a
7.5-year old boy. Breast. 13:439–442. 2004.
|
|
23
|
Serour F, Gilad A, Kopolovic J and Krispin
M: Secretory breast cancer in childhood and adolescence: report of
a case and review of the literature. Med Pediatr Oncol. 20:341–344.
1990.
|
|
24
|
Vieni S, Cabibi D, Cipolla C, Fricano S,
Graceffa G and Latteri MA: Secretory breast carcinoma with
metastatic sentinel lymph node. World J Surg Oncol. 4:882006.
|
|
25
|
Lobo RA: Potential options for
preservation of fertility in women. N Engl J Med. 353:64–73.
2005.
|
|
26
|
Ferguson TB JR, McCarty KS Jr and Filston
HC: Juvenile secretory carcinoma and juvenile papillomatosis:
diagnosis and treatment. J Pediatr Surg. 22:637–639. 1987.
|
|
27
|
Basu S, Nair N, Thorat M and Shet T:
Uptake characteristics of FDG in multiple juvenile cellular
fibroadenomata of the breast: FDG-PET and histopathologic
correlation. Clin Nucl Med. 32:203–204. 2007.
|
|
28
|
Jena M and Shariff S: Cytodiagnosis of
secretory carcinoma of the breast: a report on two cases. Diagn
Cytopathol. 38:912–924. 2010.
|
|
29
|
Lombardi A, Maggi S, Bersigotti L,
Lazzarin G, Nuccetelli E and Amanti C: Secretory breast cancer.
Case report. G Chir. 34:125–127. 2013.
|