Introduction
Lung cancer is a highly lethal and extremely common
cancer worldwide. A study of cancer statistics in 2011 reported
that the overall 5-year survival rate of lung cancer patients was
~16% (1). Non-small cell lung
cancer (NSCLC), of which adenocarcinoma and squamous cell carcinoma
account for the vast majority of cases, represents almost 80% of
primary lung cancer cases (2).
Prediction of survival is mainly based on tumor stage. Even for
patients diagnosed at stage I, the 5-year survival rate is <70%
(3). It is critically important to
identify robust, sensitive and specific biomarkers for prognosis in
NSCLC. Identification of novel biomarkers may enhance early
detection and effective treatment.
Never in mitosis gene A (NIMA)-related kinase 2
(NEK2) is a serine/threonine kinase located at the centrosome that
functions by regulating centrosome cohesion and separation via the
phosphorylation of its structural components. NEK2 exists in three
forms, NEK2A, NEK2B and NEK2C, in mammalian cells (4). It is known that the aberrant
regulation of NEK2 activity can lead to aneuploid defects and the
abnormal proliferation of cancer cells (5). The majority of previous studies on
NEK2 have been conducted in cell lines, but NEK2 has rarely been
investigated in NSCLC (6).
Numerous studies have shown that cellular
proliferative activity may provide valuable information for the
prognosis and clinical management of various types of tumors,
including NSCLC (7–12). Minichromosome maintenance complex
component 7 (Mcm7) and Ki67 are two well-known cell proliferation
markers. The former is expressed during the G1 to M
phase of the cell cycle, and the latter appears in early
G1 and persists in the S phase (13,14).
In the present study, the expression levels of Mcm7, Ki67 and novel
cell proliferation marker NEK2 were examined in NSCLC tissues, and
the prognostic ability of these three proteins was investigated and
compared.
Materials and methods
Clinical samples
A total of 270 patients who underwent a resection
for NSCLC between 2006 and 2008 at the Department of Thoracic
Surgery, The First Affiliated Hospital of China Medical University
(Shenyang, Liaoning, China), were included in the present study.
None of these patients received chemotherapy or radiotherapy prior
to surgery. The group was composed of 192 males and 78 females,
with a mean age of 62 years (range, 37–75 years) at the time of the
surgery. A summary of the patient characteristics and the
pathological characteristics is presented in Table I. Tumor specimens were either cut
immediately after removal from the resected lung tissues, frozen in
liquid nitrogen and then stored at −80°C, or collected in 10%
formalin and embedded in paraffin for histopathological analysis.
All 270 cases were independently classified as NSCLC by two
experienced pathologists according to the World Health Organization
histological typing criteria (15).
The criteria for the tumor-node-metastasis (TNM) staging system was
used to classify the clinicopathological factors and clinical
stages of lung cancer (defined by the International Union Against
Cancer TNM classification of malignant tumors, seventh edition,
2009) (15). All patients provided
written informed consent and were subject to close follow-up
observations. The median follow-up time subsequent to surgery was
60 months (range, 3 to 84 months). The study was approved by the
Human Research Ethics Committee of China Medical University, which
is accredited by the National Council on Ethics in Human
Research.
 | Table ICorrelation between NEK2, Mcm7 and
Ki67 expression and the clinicopathological features of NSCLC. |
Table I
Correlation between NEK2, Mcm7 and
Ki67 expression and the clinicopathological features of NSCLC.
| Total | NEK2 | Mcm7 | Ki67 |
|---|
|
|
|
|
|
|---|
| Characteristics | n | % | Positive case | % | P-value | Positive case | % | P-value | Positive case | % | P-value |
|---|
| Age |
| ≤60 | 112 | 41.5 | 25 | 35.7 | 0.255 | 33 | 34.7 | 0.097 | 23 | 34.8 | 0.208 |
| >60 | 158 | 58.5 | 45 | 64.3 | | 62 | 65.3 | | 43 | 65.2 | |
| Gender |
| Female | 78 | 28.9 | 47 | 67.1 | 0.395 | 29 | 30.5 | 0.662 | 24 | 36.4 | 0.123 |
| Male | 192 | 71.1 | 23 | 32.9 | | 66 | 69.5 | | 42 | 63.6 | |
| Histological
type |
| SCC | 162 | 60.0 | 42 | 60.0 | 1.000 | 57 | 60.0 | 1.000 | 45 | 68.2 | 0.119 |
| ADC | 108 | 40.0 | 28 | 40.0 | | 38 | 40.0 | | 21 | 31.8 | |
| Differentiation |
| Well | 59 | 21.9 | 14 | 20.0 | 0.277 | 23 | 24.2 | 0.729 | 16 | 24.2 | 0.600 |
| Moderate | 86 | 31.9 | 18 | 25.7 | | 28 | 29.5 | | 23 | 34.8 | |
| Poor | 125 | 46.3 | 38 | 54.3 | | 44 | 46.3 | | 27 | 40.9 | |
| Tumor size |
| T1 | 78 | 28.9 | 10 | 14.3 | 0.000a | 19 | 20.0 | 0.017a | 19 | 28.8 | 0.156 |
| T2 | 143 | 53.0 | 37 | 52.9 | | 52 | 54.7 | | 30 | 45.5 | |
| T3–4 | 49 | 18.1 | 23 | 32.9 | | 24 | 25.3 | | 17 | 25.8 | |
| Lymph node
metastasis |
| Negative | 143 | 53.0 | 27 | 38.6 | 0.011a | 42 | 44.2 | 0.057 | 31 | 47.0 | 0.053 |
| N1-positive | 72 | 26.7 | 27 | 38.6 | | 33 | 34.7 | | 25 | 37.9 | |
| N2–3-positive | 55 | 20.4 | 16 | 22.9 | | 20 | 21.1 | | 10 | 15.2 | |
| Metastasis |
| M0 | 265 | 98.1 | 68 | 97.1 | 0.469 | 91 | 95.8 | 0.034a | 63 | 95.5 | 0.062 |
| M1 | 5 | 1.9 | 2 | 2.9 | | 4 | 4.2 | | 3 | 4.5 | |
Immunohistochemistry and
immunohistochemical assessment
Immunohistochemical studies on NEK2, Mcm7 and Ki67
were performed on formalin-fixed, paraffin-embedded tissue sections
obtained from the aforementioned patients with NSCLC. Tissue
sections were deparaffinized and then boiled in 0.01 mol/l sodium
citrate buffer (pH 6.0) in a 1,000-watt microwave oven for 10 min
to retrieve cell antigens. The primary antibodies used were rabbit
polyclonal NEK2 antibody (1 to 200 dilution; Bioss, Beijing,
China), mouse monoclonal Mcm7 antibody (1 to 200 dilution; Bioss)
and mouse monoclonal Ki67 antibody (1 to 200 dilution; Maixin
Biotechnology Development Co., Ltd., Fuzhou, China). The
immunoco-expression of NEK2 with Mcm7 and Ki67 was analyzed using
contiguous slices. All tissue sections were immunohistochemically
stained using the avidin-biotin-peroxidase method and then
counterstained with hematoxylin (Shenyang Shuangding Pharmaceutical
Co., Ltd., Shenyang, China).
The staining was scored by three independent
investigators without knowledge of patient outcomes. The sections
were evaluated at low magnification (x100) to identify areas where
NEK2, Mcm7 and Ki67 were evenly stained. The percentage of
positively stained cells was calculated in >1, 000 tumor cells.
The expression levels of Mcm7 and Ki67 were assessed by the
labeling index, determined by counting the number of distinctly
stained malignant cells, regardless of the intensity, divided by
the total number of tumor cells. The two proteins were evaluated in
the areas of highest positivity, and at least 1,000 tumor cells
were counted. The average of the percentage of positive cells in
the three scores represented the final score of the sample,
yielding a continuous score from 0 to 100 for Mcm7 and Ki67. The
expression of NEK2 was determined on the basis of staining
intensity and the percentage of immunoreactive cells by reference
to the immunoreactivity score (16). Staining intensity was rated as
follows: 0, negative; 1, weakly positive; 2, moderately positive;
and 3, strongly positive. The average tumor cell staining intensity
score multiplied by the percentage of positive cells represented a
final score ranging from 0 to 300. All cases were divided into two
groups, a strongly-positive group (score range, 50–100 for Mcm7 and
Ki67; and 240–300 for NEK2). All cases with discrepancies were
jointly re-evaluated by the investigators and a consensus was
obtained.
Assessment and imaging of the immunohistochemistry
was performed using a Leica DM2000 microscope equipped with Leica
DFC Cameras-Image Acquisition System (software V3.5.0; Leica
Microsystems, Heerbrugg, Switzerland).
Immunofluorescence
The sections were deparaffinized in xylene,
rehydrated in graded alcohol series and boiled in 0.01 M citrate
buffer (pH 6.0) for 2 min in an autoclave. Double
immunofluorescence analysis was performed using rabbit polyclonal
NEK2 antibody (1 to 200 dilution), mouse monoclonal Mcm7 antibody
(1 to 200 dilution) and mouse monoclonal Ki67 antibody (1 to 200
dilution). Goat anti-rabbit (Alexa Fluor 488-labeled; Molecular
Probes) and goat anti-mouse (Alexa Fluor 594-labeled; Molecular
Probes, Invitrogen Life Technologies, Carlsbad, CA, USA) were used
as the secondary antibodies. Fluorescence signals were analyzed by
recording stained images using an Olympus FV1000 Laser Scanning
Confocal Microscope (Olympus, Tokyo, Japan).
Statistical analysis
The data were subject to statistical analysis using
the SPSS software package (version 13.0; SPSS, Inc., Chicago, IL,
USA). The correlation between the expression of NEK2 and Mcm7/Ki67
and the clinicopathological parameters was tested by χ2
test and bivariate analysis. Survival curves were calculated by the
Kaplan-Meier product-limit estimate method and then examined using
the log rank procedure. The significance of multiple predictors of
survival was assessed by the Cox regression analysis. P<0.05 was
considered to indicate a statistically significant difference.
Results
Expression of NEK2, Mcm7 and Ki67 in
NSCLC, and clinicopathological features
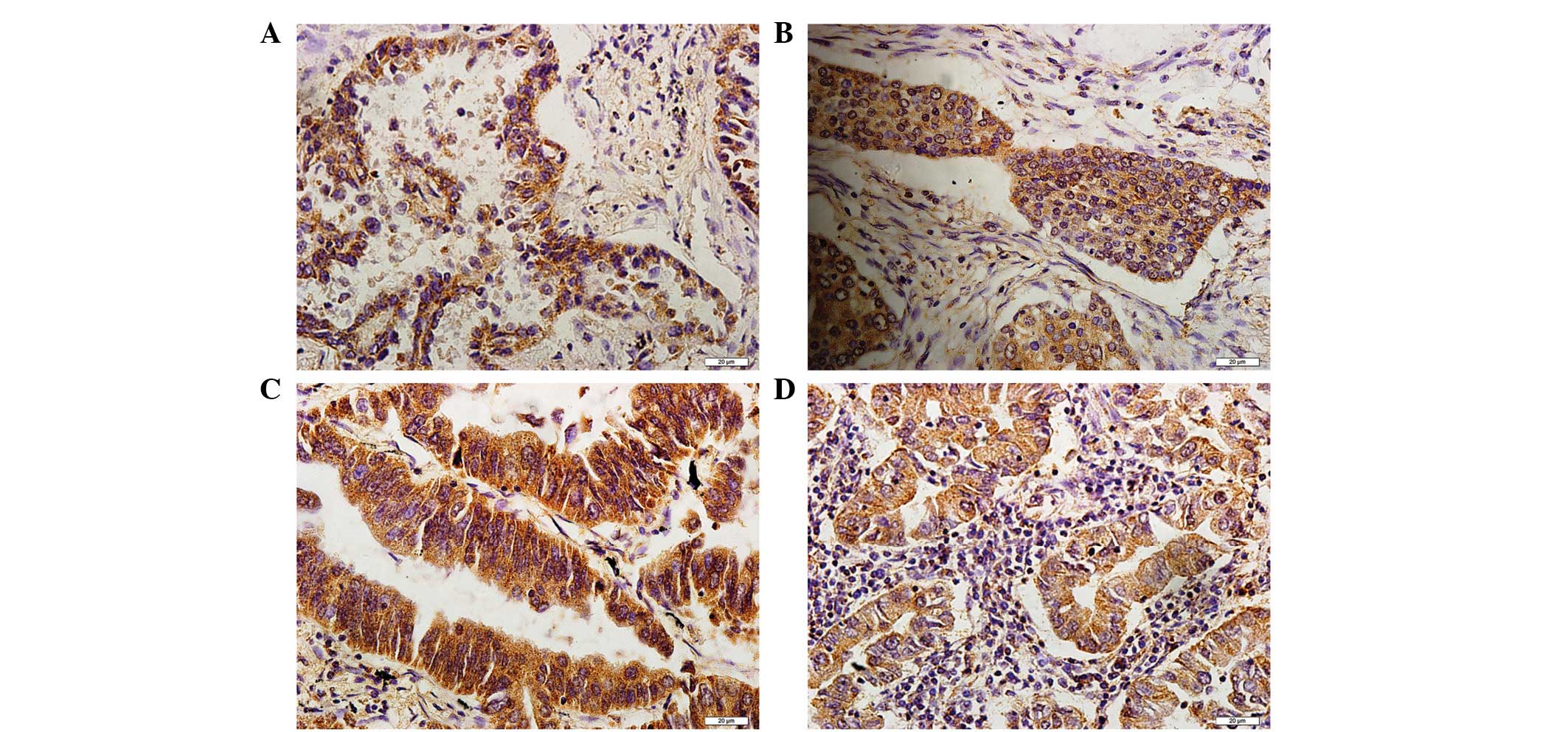
The immunohistochemistry staining for NEK2 was
mostly positive in the cytoplasm of the tumor cells (Fig. 1). Meanwhile, positive
immunohistochemical staining of Mcm7 and Ki67 was observed in the
nucleus of the tumor cells. However, NEK2, Mcm7 or Ki67 were not
expressed in normal bronchial epithelial cells. The correlation
between the expression of NEK2, Mcm7, Ki67 and the
clinicopathological characteristics of the patients with NSCLC is
summarized in Table I. The results
showed that the expression of the NEK2, Mcm7 and Ki67 proteins did
not correlate with age, gender or histological grade. However, the
expression of NEK2 was significantly correlated with the T stage
and lymph node status (P<0.0001 and P=0.011, respectively).
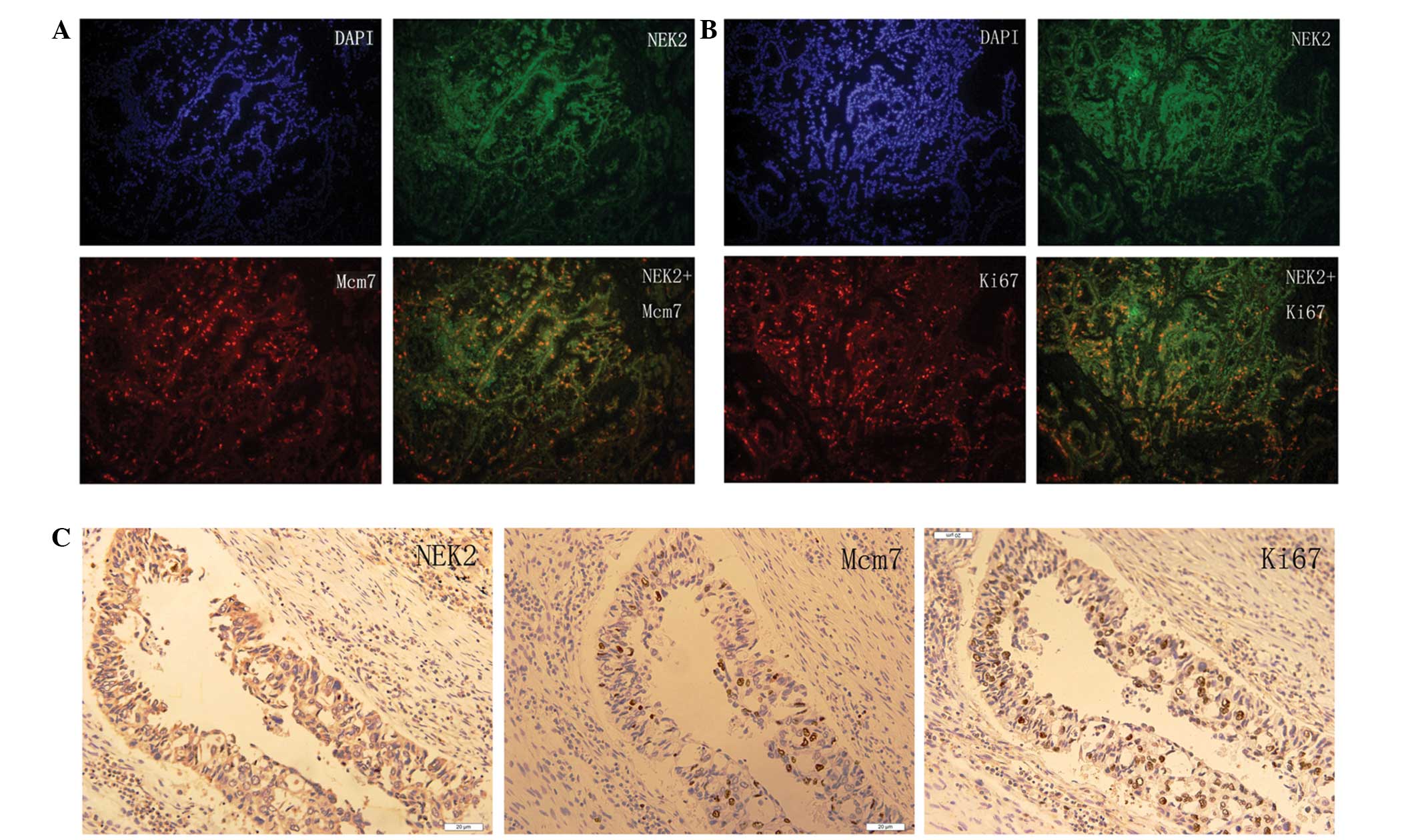
Correlation between the expression of
NEK2, Mcm7 and Ki67
NEK2 was located in the cytoplasm of the NSCLC cells
and co-located with Mcm7 and Ki67, which were located in nucleus of
the NSCLC cells. Fig. 2 presents
the co-expression and co-localization of the expression of NEK2 and
Mcm7/Ki67 in the NSCLC tissue. The correlation analysis between the
expression of NEK2 and Mcm7/Ki67 in the NSCLC tissues is summarized
in Table II. The results showed
that positive NEK2 expression was significantly associated with
positive Mcm7 and Ki67 expression (P<0.0001).
| Table IIAssociation between NEK2 and
Mcm7/Ki67 expression in NSCLC. |
Table II
Association between NEK2 and
Mcm7/Ki67 expression in NSCLC.
| Mcm7 | Ki67 |
|---|
|
|
|
|---|
|
Characteristics | Positive case | Negative case | κ-value | P-value | Positive case | Negative case | κ-value | P-value |
|---|
| NEK2-positive
case | 48 | 22 | 46.188 | <0.0001a | 32 | 38 | 23.148 | <0.0001a |
| NEK2-negative
case | 47 | 153 | | | 34 | 166 | | |
Survival analysis and prognostic
significance of the expression of NEK2, Mcm7 and Ki67
The correlation between survival and the expression
of NEK2, Mcm7 and Ki67 was evaluated in the 270 patients diagnosed
with NSCLC. A significant difference was observed when the patient
cohort was stratified by the level of the expression of NEK2, Mcm7
and Ki67. It was notable that the patients with NSCLC who had
positive NEK2 and Mcm7/Ki67 expression had a lower survival rate
than patients with NEK2- and Mcm7/Ki67-negative expression,
indicating that NEK2 is a better prognostic factor than Mcm7/Ki67
(Fig. 3). Multivariate Cox
regression analysis showed NEK2 expression was an independent
prognostic factor for overall survival in patients with NSCLC
(hazard ratio, 2.234; 95% confidence interval, 1.104–4.523;
P=0.025), which was an improvement on the expression of Mcm7
(P=0.034) and Ki67 (P=0.026). However, the combined expression of
NEK2 and Mcm7/Ki67 was an even more effective prognostic predictor
(P<0.0001) (Table III).
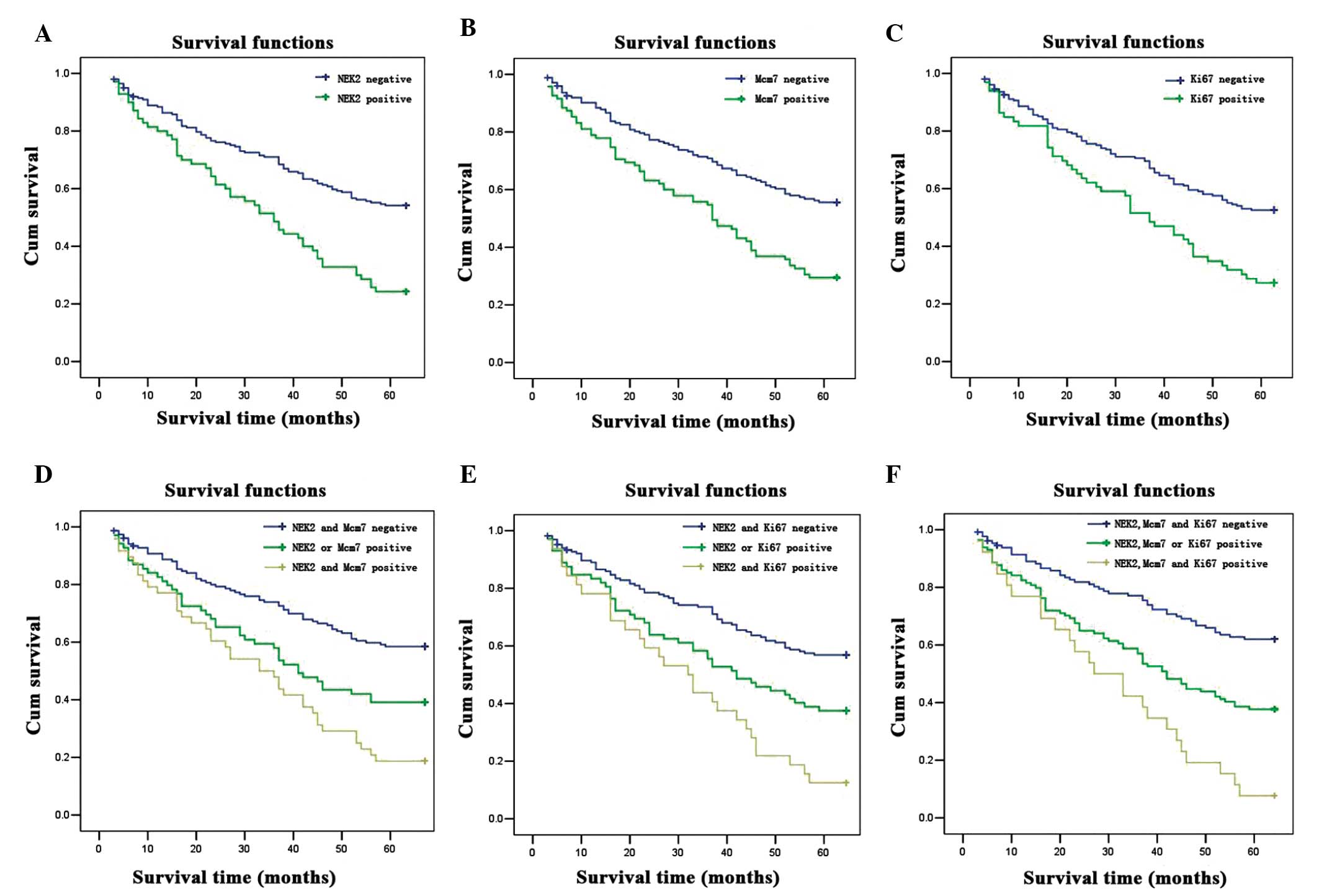 | Figure 3Kaplan-Meier curves of overall
survival in NSCLC patients. (A) The 5-year overall survival rates
were 55.0 and 24.3% in the patients with NSCLC with NEK2-negative
expression (n=200) and NEK2-positive expression (n=70). (B) The
5-year overall survival rates were 56.6 and 29.5% in the patients
with NSCLC with Mcm7-negative expression (n=175) and Mcm7-positive
expression (n=95). (C) The 5-year overall survival rates were 53.4
and 27.3% in the patients with NSCLC with Ki67-negative expression
(n=204) and Ki67-positive expression (n=66). (D) The 5-year overall
survival rates were 59.5, 39.1 and 18.8% in the patients with NSCLC
with NEK2- and Mcm7-negative expression (n=153), NEK2- or
Mcm7-positive expression (n=69), and NEK2- and Mcm7-positive
expression (n=48). (E) The 5-year overall survival rates were 57.8,
37.5 and 12.5% in the patients with NSCLC with NEK2- and
Ki67-negative expression (n=166), NEK2- or Ki67-positive expression
(n=72), and NEK2- and Mcm7-positive expression (n=32). (F) The
5-year overall survival rates were 63.1, 37.7 and 7.7% in the
patients with NSCLC with NEK2-, Mcm7- and Ki67-negative expression
(n=130), NEK2-, Mcm7- or Ki67-positive expression (n=114) and
NEK2-, Mcm7- and Ki67-positive expression (n=26). There were
significant differences between NEK2- and Mcm7/Ki67-positive, NEK2-
or Mcm7/Ki67-positive, and NEK2- and Mcm7/Ki67-negative expression
groups (P<0.0001). |
| Table IIIUnivariate and multivariate analysis
of survival in 270 patients with NSCLC. |
Table III
Univariate and multivariate analysis
of survival in 270 patients with NSCLC.
| Univariate analysis
(n=270) | Multivariate
analysis (n=270) |
|---|
|
|
|
|---|
| Variable | Hazard ratio (95%
CI) | P-value | Hazard ratio (95%
CI) | P-value |
|---|
| NEK2-positive
expression alone |
| Negative vs.
positive | 3.810
(2.064–7.036) | <0.0001a | 2.234
(1.104–4.523) | 0.0250a |
| Mcm7-positive
expression alone |
| Negative vs.
positive | 3.117
(1.830–5.310) | <0.0001a | 1.920
(1.050–3.512) | 0.0340a |
| Ki67-positive
expression alone |
| Negative vs.
positive | 3.060
(1.667–5.617) | <0.0001a | 2.179
(1.096–4.333) | 0.0260a |
| NEK2- and
Mcm7-positive expression |
| NEK2- and
Mcm7-negative vs. NEK2 | 6.360
(2.877–14.062) | <0.0001a | 5.218
(2.264–12.026) | <0.0001a |
| Mcm7-positive vs.
NEK2- and Mcm7-positive | 2.786
(1.166–6.658) | | 2.402
(0.965–5.977) | |
| NEK2- and
Ki67-positive expression |
| NEK2- and
Ki67-negative vs. NEK2 | 9.600
(3.221–28.610) | <0.0001a | 7.836
(2.494–24.625) | <0.0001a |
| Ki67-positive vs.
NEK2- and Ki67-positive | 4.200
(1.328–13.280) | | 3.401
(1.026–11.276) | |
| Age |
| <60 vs.
≥60 | 1.225
(0.754–1.991) | 0.4120 | 1.136
(0.662–1.948) | 0.6430 |
| Gender |
| Female vs.
male | 1.023
(0.604–1.733) | 0.9330 | 1.076
(0.596–1.943) | 0.8070 |
| Histological
type |
| SCC vs. ADC | 0.742
(0.454–1.211) | 0.2330 | 0.663
(0.382–1.154) | 0.1460 |
| Tumor
differentiation |
| Poor vs. well or
moderate | 1.211
(0.750–1.957) | 0.4340 | 1.359
(0.793–2.328) | 0.2640 |
| T stage |
| I or II vs. III or
IV | 3.345
(1.657–6.754) | 0.0010a | 2.228
(1.020–4.867) | 0.0440a |
| Lymph node
status |
| Negative vs.
N1-positive vs. N2-positive | 2.236
(1.370–3.649) | 0.0010a | 1.781
(1.038–3.054) | 0.0360a |
| M stage |
| M0 vs. M1 | 10×109
(0.000) | 0.9990 | 5×108
(0.000) | 0.9990 |
Discussion
During the past two decades, due to the histological
and phonotypical heterogeneity of NSCLC, identification of more
effective novel prognostic markers has become of vital importance
in the selection of high-risk patients with NSCLC (15). Effective genetic markers can further
stratify NSCLC into effective treatment subgroups. Prognosis may
improve with a focus on the molecular markers of risk, which may
lead to improved detection or treatment strategies (17,18).
It is known that the majority of tumor cells in
human malignancies exhibit centrosome abnormalities. The
deregulation of centrosome function may be a major contributory
factor to cancer cell proliferation and progression (19). NEK2 is an important centrosome
regulatory factor that was believed to be significant in finding a
molecular mechanism for tumorigenesis and may now present a novel
target for therapeutic intervention.
NEK2 is a serine/threonine kinase located at the
centrosome and involved in mitotic regulation. NEK2 overexpression
causes the induction of premature centrosome separation and nuclear
defects, which are indicative of mitotic errors (20). NEK2 is involved in cell division and
proliferation and mitotic regulation by centrosome splitting
(21,22). Previous studies have also found that
NEK2 protein expression is elevated 2–5 fold in cell lines derived
from a variety of human tumors, including those of the ovary,
breast and prostate (23). The
present study showed that NEK2 expression was significantly
upregulated in NSCLC. NEK2 expression was found to be correlated
with T stage and lymph node metastasis. We have also found
significant upregulated NEK2 expression in human breast cancer
(unpublished data), which is indicated similarly in another
previous study (24).
The Mcm7 protein is a type of licensing protein that
can regulate DNA replication and indicates the presence of cell
proliferation. The protein family includes 6 subunits, with Mcm7 as
one of them; in vivo and in vitro experiments showed
that once any member of the protein family becomes inactivated or
missed, DNA replication will be repressed. They also have duplicate
activity and play a crucial role in duplicate fork elongation
(25–28). Abnormal Mcm7 expression is observed
in numerous tumor types and correlates with a poor prognosis.
Fujioka et al previously showed that Mcm7 in the tissues of
lung adenocarcinomas could have prognostic implications (29). High MCM7 expression is also an
adverse prognostic factor for overall survival in patients with
Hodgkin lymphoma (HL) (30).
Moreover, increasing MCM7 expression was observed from normal to
cervical intraepithelial neoplasia III (CIN III) samples, with the
highest MCM7 expression values detected in CIN III cases (31). Ki67 is a proliferation-associated
nuclear antigen, whose expression can be observed in all cycling
cells, with the exception of resting cells in the G0
phase, and expressed in cells in the S/G2 and M phase in
particular. Ki67 has been widely identified as a parameter of tumor
proliferation.
The present study demonstrated that NEK2, Mcm7, Ki67
and their combined expression appears to be associated with a
poorer prognosis in patients with NSCLC. These proteins are
independent prognostic factors for survival in patients with
resected NSCLC, however, compared with Mcm7 and Ki67, NEK2 is a
more effective proliferative factor for NSCLC prognosis. Moreover,
a significant correlation was observed between the expression of
the three proteins and the clinical pathological features. These
results indicated that NEKs, Mcms and Ki67 may be involved in a
relevant pathway in the tumor cell proliferation process, which
requires further study. To the best of our knowledge, no study has
previously been published concerning the association between NEK2
expression and patient prognosis in NSCLC cases; neither has a
comparison been performed for the three cell proliferative
proteins, NEK2, Mcm7 and Ki67.
In summary, the present study data revealed that
NEK2, Mcm7 and Ki67 may all be independent prognostic factors in
patients with NSCLC. NEK2 is a better factor for determining the
prognosis of NSCLC. The evaluation of NEK2 expression may provide
useful information for doctors to make optimal clinical decisions,
and may be a novel potential target for NSCLC therapy, which will
require analysis by further validation studies.
References
|
1
|
Siegel R, Ward E, Brawley O and Jemal A:
Cancer Statistics, 2011: the impact of eliminating socioeconomic
and racial disparities on premature cancer deaths. CA Cancer J
Clin. 61:212–236. 2011.
|
|
2
|
Herbst RS, Heymach JV and Lippman SM: Lung
Cancer. N Engl J Med. 359:1367–1380. 2008.
|
|
3
|
Hotta K, Matsuo K, Ueoka H, Kiura K,
Tabata M and Tanimoto M: Role of adjuvant chemotherapy in patients
with resected non-small cell lung cancer: reappraisal with a
meta-analysis of randomized controlled trials. J Clin Oncol.
22:3860–3867. 2004.
|
|
4
|
Wu W, Baxter JE, Wattam SL, et al:
Alternative splicing controls nuclear translocation of the cell
cycle-regulated NEK2 kinase. J Biol Chem. 282:26431–26440.
2007.
|
|
5
|
Sankaran S and Parvin JD: Centrosome
functions in normal and tumor cells. J Cell Biochem. 99:1240–1250.
2006.
|
|
6
|
Tsunoda N, Kokuryo T, Oda K, et al: Nek2
as a novel molecular target for the treatment of breast carcinoma.
Cancer Sci. 100:111–116. 2009.
|
|
7
|
Rees M, Stahl M, Klump B, Willers R,
Gabbert HE and Sarbia M: The prognostic significance of
proliferative activity, apoptosis and expression of DNA
topoisomerase II alpha in multimodally-treated esophageal squamous
cell carcinoma. Anticancer Res. 21:3637–3642. 2001.
|
|
8
|
Pugsley JM, Schmidt RA and Vesselle H: The
KI-67index and survival in non-small cell lung cancer: a review and
relevance to position emission tomography. Cancer J. 8:222–233.
2002.
|
|
9
|
Daidone MG and Silvestrini R: Prognostic
and predictive role of proliferation indices in adjuvant therapy of
breast cancer. J Natl Cancer Inst Monogr. 2001.27–35
|
|
10
|
Lara PC, Rey A, Santana C, Afonso JL, Diaz
JM, Gonzalez GJ, et al: The role of Ki67 proliferation assessment
in predicting local control in bladder cancer patients treated by
radical radiation therapy.
|
|
11
|
Shepherd NA, Richman PI and England J:
Ki67 derived proliferative activity in colorectal adenocarcinoma
with prognostic correlations. J Pathol. 155:213–219. 1988.
|
|
12
|
Toyokawa G, Masuda K, Daigo Y, Cho HS,
Yoshimatsu M, Takawa M, et al: Mini chromosome maintenance protein
7 is a potential therapeutic target in human cancer and a novel
prognostic marker of non-small cell lung cancer. Mol Cancer.
10:652011.
|
|
13
|
Scholzen T and Gerdes J: The Ki67 protein:
from the known and the unknown. J Cell Physiol. 182:311–322.
2000.
|
|
14
|
Lei M and Tye BK: Initiating DNA
synthesis: from recruiting to activating the MCM complex. J Cell
Sci. 114:1447–1454. 2001.
|
|
15
|
Zhong X, Li M, Nie B, et al:
Overexpression of RACK1 and CD147 associated with poor prognosis in
stage T1 pulmonarey adenocarcinoma. Ann Surg Oncol. 20:1044–1052.
2013.
|
|
16
|
Remmele W and Schicketanz KH:
Immunohistochemical determination of estrogen and progesterone
receptor content in human breast cancer. Computer-assisted image
analysis (QIC score) vs subjective grading (IRS). Patho Res Pract.
189:862–866. 1993.
|
|
17
|
Ganem NJ, Godinho SA and Pellman D: A
mechanism linking extra centrosomes to chromosomal instability.
Nature. 460:278–282. 2009.
|
|
18
|
Niu Y, Liu T, Tse GM, et al: Increased
expression of centrosomal alpha, gamma-tubulin in atypical ductal
hyperplasia and carcinoma of the breast. Cancer Sci. 100:580–587.
2009.
|
|
19
|
Bahmanyar S, Kaplan DD, Deluca JG, et al:
Beta-catenin is a Nek2 substrate involved in centrosome separation.
Genes Dev. 22:91–105. 2008.
|
|
20
|
Hayward DG, Newbatt Y, Pickard L, et al:
Identification by high throughput screening of viridian analogs as
biochemical and cell based inhibitors of the cell cycle regulated
NEK2 kinase. J Biomol Screen. 15:918–927. 2010.
|
|
21
|
Fry AM: The NEK2 protein kinase: a novel
regulator of centrosome structure. Oncogene. 21:6184–6194.
2002.
|
|
22
|
Fletcher L, Cerniglia GJ, Nigg EA, Yend TJ
and Muschel RJ: Inhibition of centrosome separation after DNA
damage: a role for NEK2. Radiat Res. 162:128–135. 2004.
|
|
23
|
Hayward DG, Clarke RB, Faragher AJ, Pillai
MR, Hagan IM and Fry AM: The centrosomal kinase NEK2 displays
elevated levels of protein expression in human breast cancer.
Cancer Res. 64:7370–7376. 2004.
|
|
24
|
Shuling W, Weidong L, Shuhua L, Yahong W,
Ziyu L, Jing Z, Tieju L and Yun N: Abnormal expression of Nek2 and
β-catenin in breast carcinoma: clinicopathological correlations.
Histopathology. 59:631–642. 2011.
|
|
25
|
Gozuacik D, Chami M, Lagorce D, et al:
Identification and functional characterization of a new member of
the human Mcm protein family. Nucleic Acids Res. 2:570–579.
2003.
|
|
26
|
Labib K, Tercero JA and Diffley JF:
Uninterrupted Mcm2–7 function required for DNA replication fork
progression. Science. 288:1643–1647. 2000.
|
|
27
|
Crevel C, Ivetic A, Ohno K, et al: Nearest
neighbor analysis of Mcm protein complexes in drosophila
melanogaster. Nucl Acids Res. 29:4834–4842. 2001.
|
|
28
|
Lee JK and Hurwitz J: Possessive DNA
helices activity of the mini chromosome maintenance protein 4, 6
and 7 complexes requires forked DNA structures. Proc Natl Acad Sci
USA. 98:54–59. 2001.
|
|
29
|
Fujioka S, Shomori K, Nishihara K, Yagama
K, Nosaka K, Araki K, Araki K, et al: Expression of minichromosome
maintenance 7 (Mcm7) in small lung adenocarcinomas (pT1):
prognostic implication. Lung Cancer. 65:223–229. 2009.
|
|
30
|
Marnerides A, Vassilakopoulos TP,
Boltetsou E, et al: Immunohistochemical expression and prognostic
significance of CCND3, Mcm2 and Mcm7 in Hodgkin lymphoma.
Anticancer Res. 31:3585–3594. 2011.
|
|
31
|
Lobato S, Tafuri A, Fernandes PA, Caliari
MV, et al: Mini chromosome maintenance 7 protein is a reliable
biological marker for human cervical progressive decease. J Gyneco
Oncol. 23:11–15. 2012.
|