Introduction
Colorectal cancer (CRC) is the third most common
type of cancer and one of the leading causes of cancer-associated
mortality worldwide. Due to the long asymptomatic preclinical
phase, the early diagnosis and treatment of CRC is critical for
reducing disease-associated morbidity and mortality (1). The commonly used CRC screening methods
include fecal occult blood testing (FOBT), barium enema, flexible
sigmoidoscopy and colonoscopy. Among these, FOBT and colonoscopy
are used most frequently. FOBT is relatively simple, however, it
exhibits low sensitivity and specificity. Colonoscopy is considered
the ‘gold standard’ for CRC screening, although, its invasive
nature and the complex preparation required (colonic lavage), leave
numerous patients reluctant to undergo the procedure (2). It is therefore imperative to develop
an accurate and noninvasive screening test for the early detection
of CRC.
CRC is the consequence of the accumulation of
genetic and epigenetic modifications in colonic mucosal cells,
culminating in the transformation of a benign neoplasm into a
malignant tumor. Epigenetic alterations are heritable changes in
gene activity and expression that occur without any alterations in
the DNA sequence (3). Aberrant
methylation of CpG islands in gene promoter regions are commonly
associated with gene silencing and have been found to be crucial in
CRC progression. Aberrant methylation often occurs during the early
phases of CRC carcinogenesis (4).
An increasing number of hypermethylated genes have been reported to
be suitable for use as biomarkers in the detection of CRC in fecal
DNA, indicating that fecal DNA methylation analysis may present a
promising, noninvasive approach for the screening of early CRC
(5–9). Previous studies investigating the
detection of a combination of O(6)-methylguanine-DNA methyltransferase,
human Mut L homolog 1 and vimentin (VIM) gene methylation in
fecal DNA from patients with CRC, adenoma and normal individuals,
reported a sensitivity of 75% in CRC and 60% in adenoma patients,
and a specificity of 86%, respectively (5). These studies indicated that
hypermethylated gene panels may improve the sensitivity of
noninvasive screening of CRC.
In the present study, to evaluate the feasibility of
fecal DNA methylation as a noninvasive CRC screening method, the
methylation status of five gene promoters was investigated in fecal
DNA from CRC and normal controls. The genes evaluated were secreted
frizzled-related protein gene 2 (SFRP2), GATA binding
protein 4/5 (GATA4/5), N-Myc downstream-regulated
gene 4 (NDRG4) and VIM.
Materials and methods
Patients and stool samples
Stool samples were obtained from 56 patients with
CRC undergoing surgery or colonoscopy and 40 endoscopically normal
individuals undergoing colonoscopy at Li Huili Hospital (Ningbo,
China) between July 2011 and May 2012. The mean age of patients in
the cancer and control groups was 60.60±12.19 years and 59.80±12.10
years, respectively. The ratio of male to female patients in the
cancer group was 21:35, and that of the controls was 24:16. All
subjects provided written informed consent for their participation
prior to enrollment in this study and ethical approval was obtained
from the ethics committee of Ningbo Medical Center, Li Huili
Hospital. Stool samples were collected from all normal subjects and
40 CRC patients during the week prior to colonic lavage for
colonoscopy or surgery. The remaining 16 CRC stool samples were
collected 7–14 days following the initial colonoscopy. Samples were
sent to the laboratory within 1 h of defecation and stored at
−80°C.
Isolation of DNA
DNA was isolated from frozen stool samples (180–220
mg) using the QiaAmp DNA Stool mini-kit (Qiagen, Hilden, Germany),
according to the manufacturer’s instructions. The purified DNA was
stored at −20°C for use in the experiments.
Sodium bisulfite conversion
The methylation status of a DNA sequence may be
determined using sodium bisulfite, whereby bisulfite converts
unmethylated cytosine residues to uracil, leaving the methylated
cytosines unchanged (10). Sodium
bisulfite conversion and DNA recovery were performed using the
EpiTect Bisulfite Kit (Qiagen) according to the manufacturer’s
instructions, using a total of 2 μg DNA obtained from the stools.
Briefly, the DNA was diluted in 40 μl RNase-free water, to which 85
μl Bisulfite Mix and 15 μl DNA Protect Buffer was added, in 200-μl
in polymerase chain reaction (PCR) tubes. The following cycles were
performed to convert the DNA: The DNA was denatured for 5 min at
95°C and incubated for 25 min at 60°C, then denatured again at 95°C
for 5 min and incubated at 60°C for 85 min, followed by 95°C for 5
min, 60°C for 175 min, and then held at 20°C indefinitely.
Following bisulfite treatment, DNA was ethanol-precipitated,
resuspended in 39 μl elution buffer and stored at −20°C.
Methylation-specific (MSP) PCR
The methylation of the SFRP2,
GATA4/5, NDRG4 and VIM promoters in the
bisulfite-modified DNA was investigated using MSP PCR and primer
pairs designed to discriminate between methylated and unmethylated
alleles. The nucleotide sequences of the primers are shown in
Table I.
 | Table ISummary of the primer sequences, PCR
product size obtained and annealing temperature used for MSP
assays. |
Table I
Summary of the primer sequences, PCR
product size obtained and annealing temperature used for MSP
assays.
| Gene | Primer | Sequence (5′-3′) | Annealing temperature
(°C) | PCR product size
(bp) |
|---|
| SFRP2 | M | F:
5′-TTTTTGTAGGGGCGTTTTTATAAC-3′ | 54 | 163 |
| | R:
5′-TATCGATATACTCCCCAATACCG-3′ | | |
| U | F:
5′-AGATTTTTGTAGGGGTGTTTTTATAAT-3′ | 52 | 163 |
| | R:
5′-ACCTATCAATATACTCCCCAATACCA-3′ | | |
| GATA4 | M | F:
5′-GTCGGGATAGTTTTTCGTTC-3′ | 52 | 134 |
| | R:
5′-CGATTTAAAACCGACAATCA-3′ | | |
| U | F:
5′-AAGGTTGGGATAGTTTTTTGTTT-3′ | 50 | 134 |
| | R:
5′-TCCCAATTTAAAACCAACAATCA-3′ | | |
| GATA5 | M | F:
5′-TTAGAAATCGAGGAAATCGC-3′ | 54 | 133 |
| | R:
5′-GTAAACCCCCTCGTTACGTA-3′ | | |
| U | F:
5′-TGTTTAGAAATTGAGGAAATTGT-3′ | 48 | 133 |
| | R:
5′-CCCATAAACCCCCTCATTACATA-3′ | | |
| NDRG4 | M | F:
5′-GGAGTTTAAATAAAGATTACGGTAGC-3′ | 50 | 103 |
| | R:
5′-ATACGCTACGAAACCCTACC-3′ | | |
| U | F:
5′-GGGAGTTTAAATAAAGATTATGGTAGT-3′ | 48 | 103 |
| | R:
5′-AATACACTACAAAACCCTACC-3′ | | |
| VIM | M | F:
5′-AGGAAAGTATAAATTTCGGGTGC-3′ | 52 | 173 |
| | R:
5′-ATAAACGACGTCTTTCACCCTTAC-3′ | | |
| U | F:
5′-AAAAGGAAAGTATAAATTTTGGGTGT-3′ | 48 | 173 |
| | R:
5′-TATAAACAACATCTTTCACCCTTACCT-3′ | | |
Each 50 μl PCR mix consisted of 2 μl of
bisulfite-modified DNA, 1X KAPA2G buffer (10 μl; Kapa Biosystems,
Inc., Wilmington, MA, USA), 0.2 mmol/l deoxynucleotide triphosphate
mix (1 μl; Kapa Biosystems), 0.5 μmol/l of each primer (1 μl) and
0.5 units of KAPA2GTM Robust Hotstart DNA Polymerase
(Kapa Biosystems). The thermocycler conditions were as follows:
95°C for 5 min, 10 cycles of 95°C for 30 sec, Tm
(−0.8°C) for 30 sec, 72°C for 60 sec, and then 38 cycles of 95°C
for 30 sec, Tm (°C) for 30 sec, and 72°C for 60 sec,
followed by a final extension step for 10 min at 72°C. PCR products
were electrophoresed on a 2.5% agarose gel and visualized under UV
light. Each sample was subjected to MSP for all genes, and all MSP
assays were performed in triplicate to validate the results. Those
who performed the assays were blinded to all clinical
information.
Statistical analysis
The sensitivity and specificity [with 95% confidence
interval (CI)] of the fecal DNA assays were calculated. To compare
the characteristics of the different groups of patients,
χ2 tests and Fisher’s exact tests were used. Odds ratios
(OR) and the corresponding 95% CIs were used to assess the
association between DNA hypermethylation of SFRP2,
GATA4/5, NDRG4 and VIM. All statistical
tests were performed using SPSS version 11.0 software (SPSS, Inc.,
Chicago, IL, USA). All values were two-sided and P<0.05 was
considered to indicate a statistically significant difference.
Results
Stool samples were collected from 56 patients with
CRC (mean age, 59.8 years), and 40 endoscopically diagnosed healthy
controls (mean age, 60.6 years), MSP was performed on all 96
samples and each sample was subjected to MSP for all genes
(Fig. 1).
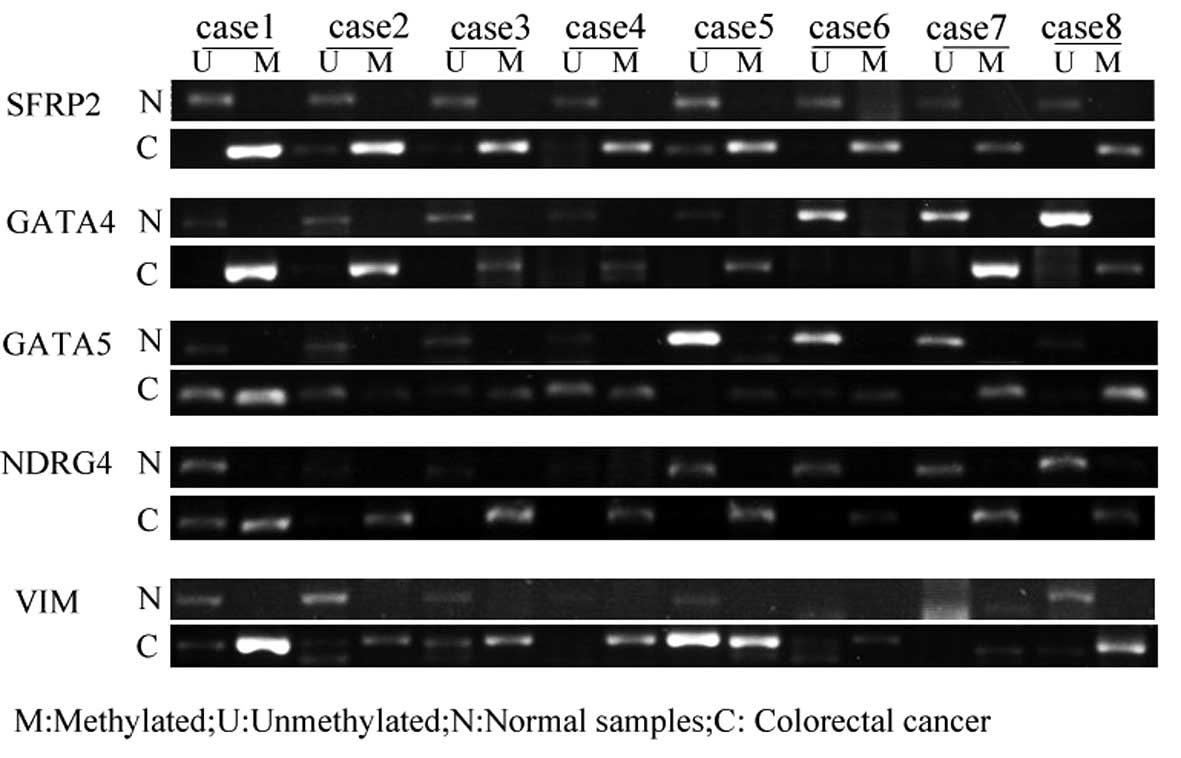 | Figure 1Methylation of SFRP2, GATA4/5, NDRG4
and VIM in fecal DNA obtained from colorectal cancer patients and
controls, as shown by methylation-specific polymerase chain
reaction using primers for methylated and unmethylated alleles of
bisulfite-modified DNA. SFRP2, secreted frizzled-related protein 2;
GATA4/5, GATA binding protein 4/5; VIM, vimentin; NDRG4, N-Myc
downstream-regulated gene 4; M, methylated; U, unmethylated; N,
normal samples; C, colorectal cancer samples. |
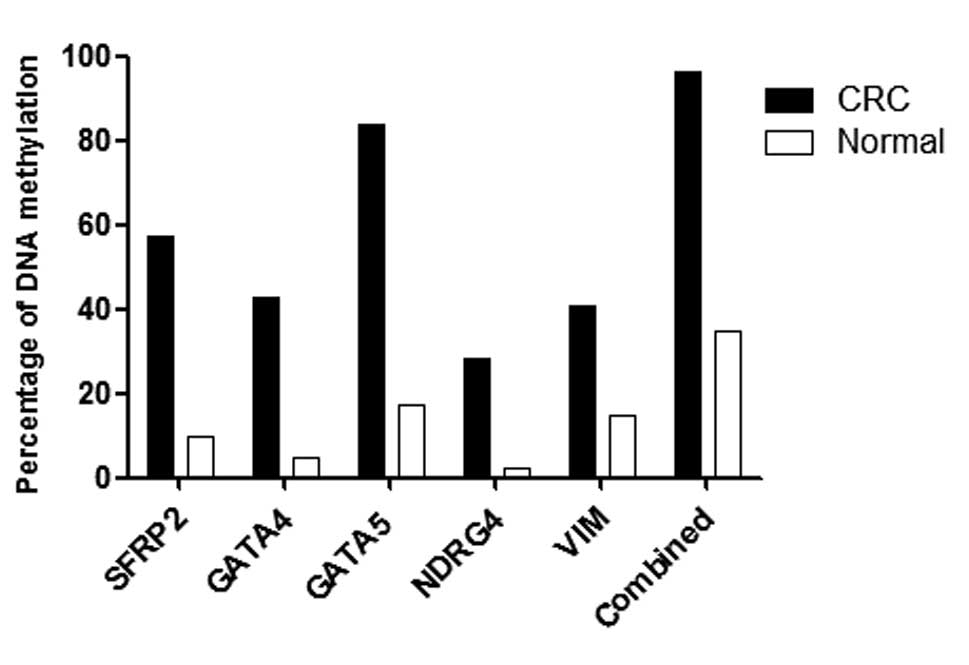
In CRC patients, SFRP2,
GATA4/5, NDRG4 and VIM were found to be
methylated at levels of 57.1% (95% CI, 44.14–69.23%), 42.9% (95%
CI, 30.77–55.86%), 83.9% (95%CI, 72.19–91.31%), 28.6% (95% CI,
18.42–41.48%) and 41.1% (95% CI, 29.17–54.12%), respectively. The
specificity of these genes was found to be 90.0% (95% CI,
76.95–96.04%), 95.0% (95% CI, 83.5–98.62%), 82.5% (95% CI,
68.05–91.25%), 97.5% (95% CI, 87.12–99.56%) and 85.0% (95% CI,
70.93–92.94%), respectively. The overall sensitivity of the
detection of fecal DNA exhibiting at least one methylated gene was
96.4% (95% CI, 87.88–99.02%) in CRC patients. By contrast, only 14
of the 40 normal individuals exhibited methylated DNA, with a
specificity of 65% (95% CI, 49.51–77.87%) (Fig. 2).
The ORs for predicting the presence of CRC using the
methylation of SFRP2, GATA4, GATA5,
NDRG4 and VIM were 12.00 (95% CI, 3.76–38.30;
P<0.01), 14.25 (95% CI, 3.13–64.97;P<0.01), 24.62 (95% CI,
8.33–72.74; P<0.01), 15.60 (95% CI, 1.97–123.36; P=0.001) and
3.95 (95% CI, 1.43–10.93; P=0.006), respectively. With the combined
analysis of the five methylation markers, the odds ratio was 50.14
(95% CI, 10.60–237.12; P<0.01)(Table II).
| Table IIComparison of predictive power between
SFRP2, GATA4/5, NDRG4, Vimentin and combined for colorectal
cancer. |
Table II
Comparison of predictive power between
SFRP2, GATA4/5, NDRG4, Vimentin and combined for colorectal
cancer.
| Gene | Sensitivity, % (95%
CI) | Specificity, % (95%
CI) | Odds ratio (95%
CI) | P-value |
|---|
| SFRP2 | 57.14
(44.14–69.23) | 90.0
(76.95–96.04a) | 12.00
(3.76–38.30) |
2.55×10−6 |
| GATA4 | 42.86
(30.77–55.86) | 95.0
(83.5–98.62a) | 14.25
(3.13–64.97) |
3.9×10−5 |
| GATA5 | 83.93
(72.19–91.31) | 82.5
(68.05–91.25a) | 24.60
(28.33–72.74) |
9.91×10−4 |
| NDRG4 | 28.57
(18.42–41.48) | 97.5
(87.12–99.56a) | 15.60
(1.97–123.36) | 0.001 |
| VIM | 41.07
(29.17–54.12) | 85.0
(70.93–92.94) | 3.95
(1.43–10.93) | 0.006 |
| Combined | 96.43
(87.88–99.02a) | 65.0
(49.51–77.87a) | 50.14
(10.60–237.12) |
6.65×10−11 |
To compare the characteristics of the different
groups of patients, χ2 and Fisher’s exact tests were
used. The associations between clinicopathological characteristics
of the CRC patients and the methylation statuses of SFRP2,
GATA4, GATA5, NDRG4 and VIM are shown
in Table III. No statistically
significant differences were identified with respect to patient
gender, age, tumor-node-metastasis (TNM) stage or tumor
location.
| Table IIIAssociation between DNA
hypermethylation and clinicopathological characteristics of
colorectal cancer. |
Table III
Association between DNA
hypermethylation and clinicopathological characteristics of
colorectal cancer.
|
Characteristics | Cases, n | SFRP2 | GATA4 | GATA5 | NDRG4 | VIM | Combined |
|---|
| Colorectal
cancer | 56 | 32/56 (57.1) | 24/56 (42.9) | 47/56 (83.9) | 16/56 (28.6) | 23/56 (41.1) | 54/56 (96.4) |
| Gender |
| Male | 21 | 10/21 (47.6) | 12/21 (57.1) | 17/21 (81.0) | 6/21 (28.6) | 7/21 (33.3) | 20/21 (95.2) |
| Female | 35 | 22/35 (62.9) | 12/35 (34.3) | 30/35 (85.7) | 10/35 (28.6) | 16/35 (45.7) | 34/35 (97.1) |
| P-value | | 0.265 | 0.094 | 0.925 | 1 | 0.362 | 1 |
| Age, years |
| ≤50 | 10 | 6/10 (60.0) | 4/10 (40.0) | 9/10 (90.0) | 2/10 (20.0) | 5/10 (50.0) | 10/10 (1.0) |
| >50 | 46 | 26/46 (56.5) | 20/46 (43.5) | 38/46 (82.6) | 14/46 (30.4) | 18/46 (39.1) | 44/46 (95.7) |
| P-value | | 1 | 1 | 0.919 | 0.783 | 0.781 | 1 |
| TNM stage |
| I/II | 32 | 16/32 (50.0) | 12/32 (37.5) | 25/32 (78.1) | 7/32 (21.9) | 13/32 (40.6) | 30/32 (93.8) |
| III/IV | 24 | 16/24 (66.7) | 12/24 (50.0) | 22/24 (91.7) | 9/24 (37.5) | 10/24 (41.7) | 24/24 (1.0) |
| P-value | | 0.212 | 0.35 | 0.318 | 0.2 | 0.938 | 0.5 |
| Location |
| Rectum | 38 | 23/38 (60.5) | 13/38 (34.2) | 29/38 (76.3) | 10/38 (26.3) | 16/38 (42.1) | 36/38 (94.7) |
| Right colon | 6 | 3/6 (50.0) | 3/6 (50.0) | 6/6 (1.0) | 2/6 (33.3) | 2/6 (33.3) | 6/6 (1.0) |
| Left colon | 12 | 6/12 (50.0) | 8/12 (66.7) | 12/12 (1.0) | 4/12 (33.3) | 5/12 (41.7) | 12/12 (1.0) |
| P-value | | 0.768 | 0.131 | 0.079 | 0.865 | 0.92 | 0.6123 |
| Normal control | 40 | 4/40 (10.0) | 2/40 (5.0) | 7/40 (17.5) | 1/40 (2.5) | 6/40 (15.0) | 14/40 (35.0) |
Discussion
Although screening for CRC in individuals aged
>50 years has been shown to reduce the incidence and mortality
of CRC, numerous patients do not undergo colonoscopy-based
screening due to its invasive nature (11,12).
FOBT, which is a noninvasive form of CRC screening, is currently
widely used. However, the sensitivity of FOBT is only 15–35%, and a
substantial proportion of tumors that are not associated with
bleeding remain undetected (13).
Since colon cancer cells are continuously shed into the colonic
lumen and released into the stool, including cells from early-stage
cancer growths, molecular tests for genetic and epigenetic
alterations in fecal DNA have been proposed as feasible screening
methods for the early detection of colorectal neoplasias (14). Previous studies have demonstrated
the potential feasibility of detecting DNA mutations in the feces
of CRC patients. Ahlquist et al (15) analyzed freezer-archived stools from
22 patients with CRC, 11 of which with adenomas of >1 cm, and 28
normal subjects. The assay targets included point mutations at any
of the 15 commonly mutated sites on the K-ras, p53
and APC genes. Sensitivity was 91% for cancer and 82% for
adenomas, with a specificity of 93%. However, due to the high cost
of the multitarget panels and a difficult collection process, the
clinical application of CRC screening using DNA mutation detection
has been limited. Detecting epigenetic alterations in fecal DNA has
increasingly been considered as an effective approach for the
detection of colorectal neoplasias (16). Currently, an increasing number of
hypermethylated genes in stool samples have been reported as
potential biomarkers for the detection of colorectal neoplasias.
Using methylated genes in the feces of CRC patients, a
meta-analysis demonstrated an overall sensitivity of 62% and a
specificity of 80% for colorectal neoplasia (17).
In the present study, the feasibility of detecting
methylated DNA in stool samples was evaluated as a noninvasive
screening tool. The evaluation of five methylation markers,
SFRP2, GATA4/5, NDRG4 and VIM,
revealed that >96% of patients with CRC and only 35% of normal
controls exhibited at least one methylated allele in their fecal
samples. Among the five genes, two demonstrated >50% sensitivity
in fecal DNA from CRC patients and all five genes exhibited >60%
specificity in controls. The GATA5 methylation marker
demonstrated the highest sensitivity (83.9%) in stool samples from
individuals with CRC. No association was identified between the
presence of methylated fecal DNA and patient gender, age, TNM stage
or tumor location. Overall, these results indicated a correlation
between early-stage and later-stage CRC, and that this method of
detection may have equivalent sensitivity in proximal and distal
cancers. Thus, the analysis of fecal DNA methylation may present a
useful and noninvasive method of screening for colorectal
neoplasia.
All five methylation markers of the genes selected
for this study have been identified in CRC previously. The
SFRP2 gene belongs to a recently established category of
tumor suppressor genes, SFRPs, and silencing of SFRPs
via promoter methylation causes constitutive activation of the
Wnt/β-catenin signaling pathway, which is associated with multiple
tumors, including CRC (18). Müller
et al (19) reported that SFRP2 hypermethylation
exhibits a sensitivity of 77–90% with regard to identifying
patients with CRC. Huang et al (20) reported that methylation of SFRP2
occurs in 94.2% of patients with CRC, with occurrences of 52.4,
37.5 and 16.7% in adenomas, hyperplastic polyps and ulcerative
colitis, respectively. In this study, methylated SFRP2 was
detected in the stool samples of Chinese patients with CRC and
normal individuals, indicating that it is an effective marker
suitable for detecting CRC, with a sensitivity of 57.1% and
specificity of 70%. However, these values were lower than those
reported in previous studies (18,19).
The methylation of GATA4 is also a frequent
and specific event in CRC. GATA4 is a regulatory
transcription factor that suppresses upstream Dab2. Methylation of
the CpG islands of the promoters of this tumor suppressor gene may
lead to gene silencing. Hellebrekers et al (21) investigated GATA4 methylation
in the fecal DNA of CRC patients and controls, and found it to
exhibit a sensitivity of 59% and specificity of 88% for CRC
detection. The results of the present study identified methylated
GATA4 in 42.9% of CRC fecal samples.
NDRG4 has been investigated as a possible
tumor suppressor, and NDRG4 mRNA and protein expression were
found to be lower in CRC than in control samples, which was
observed to correlate with the methylation status of the promoters
of this gene. Melotte et al (22) investigated NDRG4 promoter
methylation as a biomarker for the early detection of CRC in fecal
samples, whereby it demonstrated a sensitivity of 56% and a
specificity of 96%. However, the present study revealed a lower
sensitivity (28.57%) in CRC detection.
In the present study, the three aforementioned
methylated genes were used to investigate the utility of fecal DNA
in CRC detection. The results revealed that the specificity and
sensitivity of SFRP2 (90.0 and 57.1%, respectively), GATA4 (95 and
42.9%, respectively) and NDRG4 (97.5 and 28.57%) were lower than
those reported in previous studies. These differences may be due to
the different methods of detecting methylation, differences in
technical personnel and differences in patient populations.
The VIM gene, a marker of mesenchymal cells,
encodes a protein constituent of intermediate filaments and has
been demonstrated to be transcriptionally silent in normal
colorectal epithelial crypt cells (23). Aberrant VIM methylation may
be detected in the fecal DNA of CRC patients; however, it is rarely
identified in normal subjects. Furthermore, using the VIM
gene methylation marker as a noninvasive method for early CRC has
been commercialized (23). Chen
et al (24) observed 46%
sensitivity with 90% specificity for CRC detection in the aberrant
VIM exon 1 and methylation of fecal DNA, indicating
hypermethylation. In the present study, results associated with
VIM (methlyation levels of 41.1%)were comparable to those of
previous studies.
Among the five genes investigated in this study,
GATA5 demonstrated the most potential as a methylation
marker for CRC screening, as it exhibited the highest sensitivity
(83.9%) for CRC in individual fecal samples. To evaluate the
potential of GATA5 as a methylation marker for CRC
detection, Hellebrekers et al (21) analyzed large groups of CRC patients
and controls, and observed a high frequency of GATA5
methylation in CRC (79%) and low levels in normal colorectal mucosa
(13%). In the present study, the methylation of GATA5 in
fecal DNA for CRC detection exhibited a higher sensitivity (83.9%)
than in the study by Hellebrekers et al (79%) (21). Although the sensitivities were
different, the two studies indicated that the methylation of
GATA5 in fecal DNA may present a potential biomarker for
colorectal tumors.
In conclusion, the results of the present study
demonstrated the feasibility of using multiple methylation markers
as a noninvasive method for detecting early CRC. Further studies
are required to refine the panel of potential methylation markers
for CRC.
Acknowledgements
This study was supported by the Social Development
Foundation of Ningbo (grant no. 2011C50022) and the Scientific
Innovation Team Project of Ningbo (grant no. 2013B82010).
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012.
|
|
2
|
Jenkinson F and Steele RJ: Colorectal
cancer screening-methodology. Surgeon. 8:164–171. 2010.
|
|
3
|
Kim MS, Lee J and Sidransky D: DNA
methylation markers in colorectal cancer. Cancer Metastasis Rev.
29:181–206. 2010.
|
|
4
|
Kondo Y and Issa JP: Epigenetic changes in
colorectal cancer. Cancer Metastasis Rev. 23:29–39. 2004.
|
|
5
|
Baek YH, Chang E, Kim YJ, et al: Stool
methylation-specific polymerase chain reaction assay for the
detection of colorectal neoplasia in Korean patients. Dis Colon
Rectum. 52:1452–1459; discussion 1459–1463. 2009.
|
|
6
|
Leung WK, To KF, Man EP, et al: Detection
of hypermethylated DNA or cyclooxygenase-2 messenger RNA in fecal
samples of patients with colorectal cancer or polyps. Am J
Gastroenterol. 102:1070–1076. 2007.
|
|
7
|
Petko Z, Ghiassi M, Shuber A, et al:
Aberrantly methylated CDKN2A, MGMT, and MLH1 in colon polyps and in
fecal DNA from patients with colorectal polyps. Clin Cancer Res.
11:1203–1209. 2005.
|
|
8
|
Ausch C, Kim YH, Tsuchiya KD, et al:
Comparative analysis of PCR-based biomarker assay methods for
colorectal polyp detection from fecal DNA. Clin Chem. 55:1559–1563.
2009.
|
|
9
|
Abbaszadegan MR, Tavasoli A, Velayati A,
et al: Stool-based DNA testing, a new noninvasive method for
colorectal cancer screening, the first report from Iran. World J
Gastroenterol. 13:1528–1533. 2007.
|
|
10
|
Frommer M, McDonald LE, Millar DS, et al:
A genomic sequencing protocol that yields a positive display of
5-methylcytosine residues in individual DNA strands. Proc Natl Acad
Sci USA. 89:1827–1831. 1992.
|
|
11
|
Jemal A, Siegel R, Ward E, et al: Cancer
statistics, 2009. CA Cancer J Clin. 59:225–249. 2009.
|
|
12
|
Vernon SW: Participation in colorectal
cancer screening: a review. J Natl Cancer Inst. 89:1406–1422.
1997.
|
|
13
|
Winawer S, Fletcher R, Rex D, et al;
Gastrointestinal Consortium Panel. Colorectal cancer screening and
surveillance: clinical guidelines and rationale-update based on new
evidence. Gastroenterology. 124:544–560. 2003.
|
|
14
|
Ahlquist DA and Shuber AP: Stool screening
for colorectal cancer: evolution from occult blood to molecular
markers. Clin Chim Acta. 315:157–168. 2002.
|
|
15
|
Ahlquist DA, Skoletsky JE, Boynton KA, et
al: Colorectal cancer screening by detection of altered human DNA
in stool: feasibility of a multitarget assay panel.
Gastroenterology. 119:1219–1227. 2000.
|
|
16
|
Wu GH, Wang YM, Yen AM, et al:
Cost-effectiveness analysis of colorectal cancer screening with
stool DNA testing in intermediate-incidence countries. BMC Cancer.
6:1362006.
|
|
17
|
Luo YX, Chen DK, Song SX, et al: Aberrant
methylation of genes in stool samples as diagnostic biomarkers for
colorectal cancer or adenomas: a meta-analysis. Int J Clin Pract.
65:1313–1320. 2011.
|
|
18
|
Suzuki H, Gabrielson E, Chen W, et al: A
genomic screen for genes upregulated by demethylation and histone
deacetylase inhibition in human colorectal cancer. Nat Genet.
31:141–149. 2002.
|
|
19
|
Müller HM, Oberwalder M, Fiegl H, et al:
Methylation changes in faecal DNA: a marker for colorectal cancer
screening? Lancet. 363:1283–1285. 2004.
|
|
20
|
Huang Z, Li L and Wang J: Hypermethylation
of SFRP2 as a potential marker for stool-based detection of
colorectal cancer and precancerous lesions. Dig Dis Sci.
52:2287–2291. 2007.
|
|
21
|
Hellebrekers DM, Lentjes MH, van den Bosch
SM, et al: GATA4 and GATA5 are potential tumor suppressors and
biomarkers in colorectal cancer. Clin Cancer Res. 15:3990–3997.
2009.
|
|
22
|
Melotte V, Lentjes MH, van den Bosch SM,
et al: N-Myc downstream-regulated gene 4 (NDRG4): a candidate tumor
suppressor gene and potential biomarker for colorectal cancer. J
Natl Cancer Inst. 101:916–927. 2009.
|
|
23
|
Lodish H, Baltimore D, Berk A, Zipursky
SL, Mastudaira P and Darnell J: Molecular cell biology. 3rd
Edition. Scientific American Books; New York, NY: 1995
|
|
24
|
Chen WD, Han ZJ, Skoletsky J, et al:
Detection in fecal DNA of colon cancer-speciic methylation of the
nonexpressed vimentin gene. J Natl Cancer Inst. 97:1124–1132.
2005.
|