Introduction
The gastrointestinal tract is the most common site
for primary extranodal lymphoma which accounts for ≤40% of all
cases (1,2). The most common location for GI tract
involvement is the stomach (1,2).
Gastric diffuse large B-cell lymphoma (DLBCL) is a common subtype.
Gastric DLBCL may be treated with surgical resection, chemotherapy
and radiotherapy either alone or in combination. Surgical
intervention may be reserved for treating complications such as
major bleeding, obstruction or perforation (2). Conservative treatment with
chemotherapy with or without radiotherapy is the preferred
treatment method (3,4). According to previous retrospective
studies, rituximab, in combination with chemotherapy, has a higher
complete response, event-free survival and overall survival rates
compared with conventional chemotherapy (5,6).
Lymphomas can directly, by neoplastic infiltration, or indirectly,
by a paraneoplastic or infectious cause, involve the peripheral and
central nerves (7,8). Multiple cranial nerve involvement is
not uncommon in lymphoma, but isolated neuropathy is rare. The
facial nerve is the most vulnerable to leptomeningeal disease
(9,10). Isolated oculomotor nerve palsy (ONP)
from lymphoma is also extremely rare (11,12).
The diagnosis and management of ONP are directed by the age of the
patient and by the degree to which the third nerve major functions
(pupillomotor, oculomotor) have been affected. The outcome of ONP
is related to its cause (13). The
involvement of the central nervous system (CNS) at the time of
diagnosis in DLBCL is uncommon and the majority of the events occur
during relapse, with an incidence ranging from 2–7% (14–16).
High-dose methotrexate with or without CNS-directed therapy is
normally used for disease control. The patient prognosis is poor,
despite treatment options being available (17,18).
The present study reports the case of a patient with gastric DLBCL
with isolated pupil-sparing ONP. Written informed consent was
obtained from the patient.
Case report
A 72-year-old female with a medical history of
hypertension presented with left ptosis and diplopia, easy-onset
fatigue and abdominal fullness that had persisted for two weeks.
Upon admission, the patient was afebrile with normal vital signs,
but appeared lethargic. Physical examination revealed pale
conjunctiva, mild upper abdominal tenderness and splenomegaly 2 cm
below the left costal margin. There was no overt lymphadenopathy.
In a neurological examination, the patient exhibited left ONP with
ptosis and external ophthalmoplegia (Fig. 1). There were no pupillary or visual
abnormalities. Other cranial nerves, muscle power, sensation,
coordination and reflexes were normal. Laboratory studies revealed
a white blood cell count of 2,460/μl (normal range,
4,500–11,000/μl), a hemoglobin level of 4.9 g/dl (normal range,
12–16 g/dl), a mean corpuscular volume of 80.7 fl (normal range,
80–100 fl) and a platelet count of 145×103/μl (normal
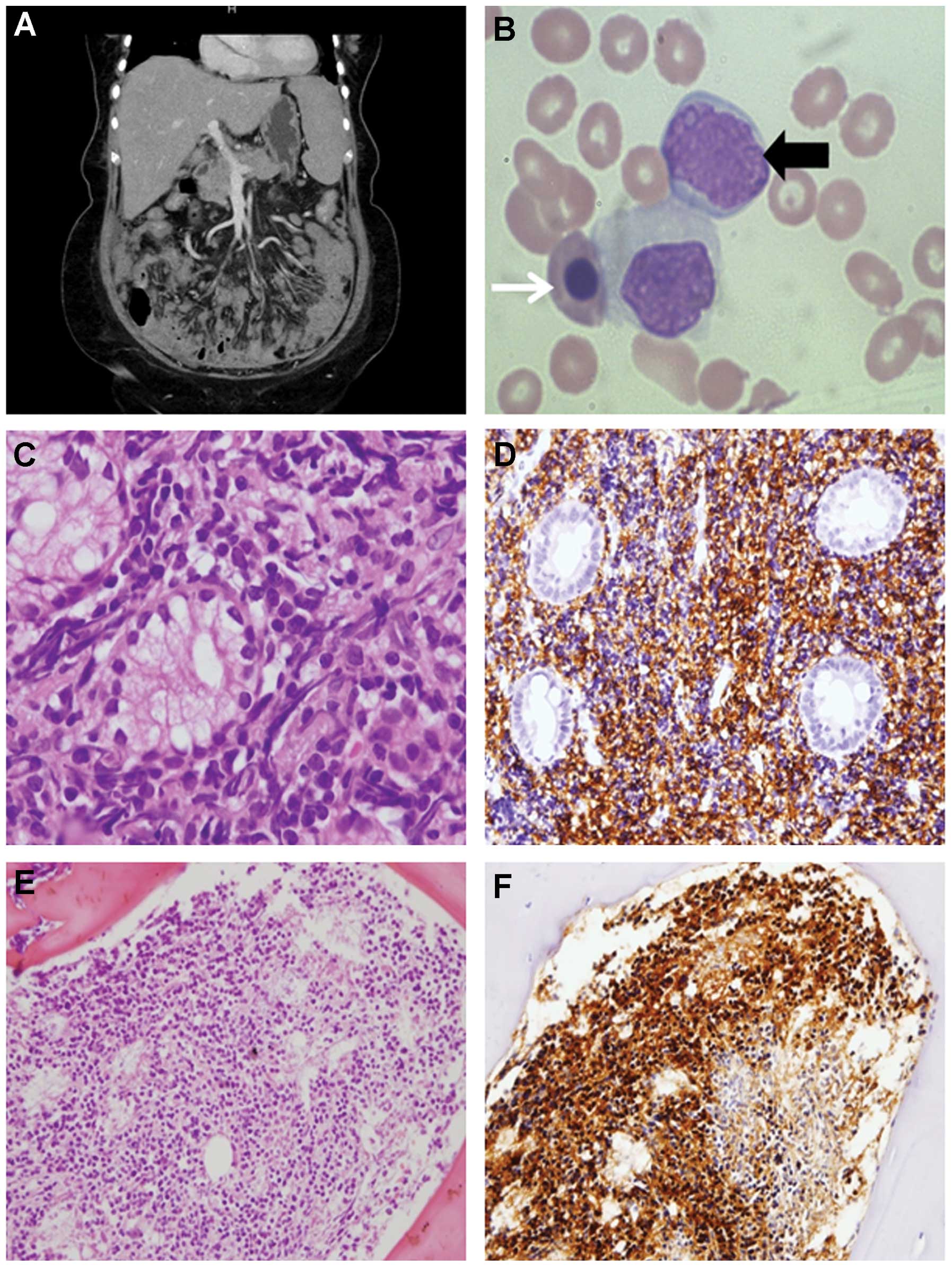
range, 150–400×103/μl), with myeloid precursors and
nucleated red blood cells in the peripheral smear (Fig. 2A). The patient also had a serum
ferritin level of 1,480 ng/ml (normal range, 20–300 ng/ml), a serum
lactic dehydrogenase level of 2,007 U/l (normal range, 115–245 U/l)
and occult blood was present in the stool. Gadolinium-enhanced
brain magnetic resonance imaging (MRI) displayed no abnormality of
the cavernous sinus and no leptomeningeal disease. The cranial
nerves were well delineated without abnormal enhancement. A
contrast-enhanced computed tomography scan of the abdomen revealed
thickening of the wall of the gastric antrum and diffuse
intra-abdominal lymphadenopathy (Fig.
2B). Panendoscopy revealed multiple polypoid lesions with
ulcers in the gastric antrum and body. These were biopsied and were
found to be consistent with DLBCL upon histopathological assessment
(Fig. 2C and D). A bone marrow
biopsy was performed that revealed lymphoma involvement (Fig. 2E and F), and
[18F]-fluorodeoxyglucose (FDG) positron emission
tomography revealed multiple FDG-avid lesions in the entire
skeleton, as well as within the abdomen. The patient was therefore
diagnosed with Ann Arbor stage IVB gastric DLBCL with involvement
of the bone marrow and left-sided isolated ONP. A lumbar puncture
was performed and revealed a negative finding. The patient received
systemic chemotherapy with 375 mg/m2 rituximab on day 1,
750 mg/m2 cyclophosphamide on day 1, 1.4
mg/m2 vincristine on day 1 and 100 mg prednisolone on
days 1–5, every three weeks. Anthracyclines were not administered
during the treatment due to the patient’s poor overall condition
and the high risk of toxicity. The symptom of left ONP was resolved
completely two weeks after the first cycle of chemotherapy.
Discussion
Lesions arising anywhere along the course of the
oculomotor nerve, including the nucleus, the fascicles in the
midbrain tegmentum and the spaces it passes through, including the
subarachnoid space, the cavernous sinus and the superior orbital
fissure, can lead to palsy of the nerve. The major causes of
isolated third nerve palsy include aneurysms of the posterior
communicating artery, microvascular ischemia, neoplasm,
inflammation and trauma (13).
Microvascular ischemia, which is often associated with diabetes
mellitus and hypertension, is believed to be the most common cause
of isolated pupil-sparing third nerve palsies. However, compression
by aneurysms or tumors can also lead to pupil-sparing ONP (19). Neuroimaging, such as brain MRI, is
suggested for patients with such presentation.
Sato et al (20) reviewed 14 lymphoma cases presenting
with ONP, and ten out of 14 were assessed by using brain MRI, which
detected eight patients with CNS involvement. The majority of the
patients with pupil-sparing ONP exhibited cavernous sinus
involvement rather than oculomotor nerve infiltration (16). Brain MRI combined with cerebrospinal
fluid (CSF) cytology examination is considered optimal for
evaluating the cause of ONP, but may not be diagnostic in every
case. In the present patient, brain MRI revealed no significant
cranial abnormality and the lumbar puncture examination
demonstrated a negative result. Since a diagnosis of lymphoma was
made based on gastric and bone marrow biopsies, the patient was
able to start systemic chemotherapy and exhibited a good response,
including total recovery of the ONP. The fact that the patient
recovered without the use of intrathecal or other CNS-directed
therapy makes it more likely that the ONP was a paraneoplastic
phenomenon and not from lymphomatous involvement of the CNS.
In conclusion, this case demonstrates that isolated
ONP associated with gastric DLBCL may represent a paraneoplastic
feature of the disease. As such, if brain imaging and CSF
examination do not reveal involvement of lymphoma, it may be
reasonable to forgo CNS-directed therapy and only treat with
appropriate systemic therapy for the underlying disease.
Acknowledgements
The authors extend their thanks to Dr Vivek R.
Sharma, Division of Medical Oncology/Hematology, University of
Louisville, School of Medicine (Louisville, KY, USA) for providing
a critical review and comments on the original manuscript.
References
|
1
|
d’Amore F, Brincker H, Grønbaek K, et al:
Non-Hodgkin’s lymphoma of the gastrointestinal tract: a
population-based analysis of incidence, geographic distribution,
clinicopathologic presentation features, and prognosis. Danish
Lymphoma Study Group. J Clin Oncol. 12:1673–1684. 1994.
|
|
2
|
Psyrri A, Papageorgiou S and Economopoulos
T: Primary extranodal lymphomas of stomach: clinical presentation,
diagnostic pitfalls and management. Ann Oncol. 19:1992–1999.
2008.
|
|
3
|
Coiffier B and Salles G: Does surgery
belong to medical history for gastric lymphomas? Ann Oncol.
8:419–421. 1997.
|
|
4
|
Raderer M, Chott A, Drach J, et al:
Chemotherapy for management of localised high-grade gastric B-cell
lymphoma: how much is necessary? Ann Oncol. 13:1094–1098. 2002.
|
|
5
|
Tanaka T, Shimada K, Yamamoto K, et al:
Retrospective analysis of primary gastric diffuse large B cell
lymphoma in the rituximab era: a multicenter study of 95 patients
in Japan. Ann Hematol. 91:383–390. 2012.
|
|
6
|
Zhang J, Li G, Yang H, Liu X and Cao J:
Rituximab in treatment of primary gastric diffuse large B-cell
lymphoma. Leuk Lymphoma. 53:2175–2181. 2012.
|
|
7
|
Hughes RA, Britton T and Richards M:
Effects of lymphoma on the peripheral nervous system. J R Soc Med.
87:526–530. 1994.
|
|
8
|
Recht LD: Neurologic complications of
systemic lymphoma. Neurol Clin. 9:1001–1015. 1991.
|
|
9
|
Law IP, Dick FR, Blom J and Bergevin PR:
Involvement of the central nervous system in non-Hodgkin’s
lymphoma. Cancer. 36:225–231. 1975.
|
|
10
|
Levitt LJ, Dawson DM, Rosenthal DS and
Moloney WC: CNS involvement in the non-Hodgkin’s lymphomas. Cancer.
45:545–552. 1980.
|
|
11
|
MacKintosh FR, Colby TV, Podolsky WJ, et
al: Central nervous system involvement in non-Hodgkin’s lymphoma:
an analysis of 105 cases. Cancer. 49:586–595. 1982.
|
|
12
|
Woodruff MM and Edlow JA: Evaluation of
third nerve palsy in the emergency department. J Emerg Med.
35:239–246. 2008.
|
|
13
|
Bruce BB, Biousse V and Newman NJ: Third
nerve palsies. Semin Neurol. 27:257–268. 2007.
|
|
14
|
Feugier P, Virion JM, Tilly H, et al:
Incidence and risk factors for central nervous system occurrence in
elderly patients with diffuse large-B-cell lymphoma: influence of
rituximab. Ann Oncol. 15:129–133. 2004.
|
|
15
|
Kumar A, Vanderplas A, LaCasce AS, et al:
Lack of benefit of central nervous system prophylaxis for diffuse
large B-cell lymphoma in the rituximab era: findings from a large
national database. Cancer. 118:2944–2951. 2012.
|
|
16
|
Tomita N, Yokoyama M, Yamamoto W, et al:
Central nervous system event in patients with diffuse large B-cell
lymphoma in the rituximab era. Cancer Sci. 103:245–251. 2012.
|
|
17
|
van Besien K, Gisselbrecht C, Pfreundschuh
M and Zucca E: Secondary lymphomas of the central nervous system:
risk, prophylaxis and treatment. Leuk Lymphoma. 49:52–58. 2008.
|
|
18
|
Kim SJ, Oh SY, Kim JS, et al: Secondary
central nervous system (CNS) involvement in patients with diffuse
large B-cell lymphoma: a therapeutic dilemma. Ann Hematol.
90:539–546. 2011.
|
|
19
|
Jacobson DM: Relative pupil-sparing third
nerve palsy: etiology and clinical variables predictive of a mass.
Neurology. 56:797–798. 2001.
|
|
20
|
Sato H, Hashimoto T, Yoneda S, Hirabayashi
K, Oguchi K and Higuchi K: Lymphoma as a cause of isolated
oculomotor nerve palsy. J Clin Neurosci. 18:1256–1258. 2011.
|