Introduction
As a heterogeneous and complex disease, lung cancer
is a challenge to treat (1). The
change to personalized treatment based on appropriate patient
selection has been advanced by the identification of epidermal
growth factor receptor (EGFR) mutations and anaplastic lymphoma
kinase (ALK) rearrangements in non-small cell lung cancer (NSCLC)
(2). The incidence of echinoderm
microtubule-associated protein-like 4 (EML4)-ALK fusion and EGFR
mutation in patients with NSCLC is 7 and 15%, respectively.
Previous studies have indicated that functional ALK rearrangement
is mutually exclusive with other known activating mutations, such
as the EGFR and KRAS mutations (3).
However, the coexistence of EML4-ALK fusions and EGFR mutations has
been reported continuously in patient case studies (4–8). The
possibility of coexisting ALK fusions and EGFR or KRAS mutations
would have a profound impact on the choice of therapy and would
affect clinical laboratory workflow (3). Secondary mutations in kinases may be a
common mechanism of drug resistance to kinase inhibitors (TKIs)
(9). The aim of the present study
was to investigate the association between secondary mutations and
acquired resistance to TKIs.
Case report
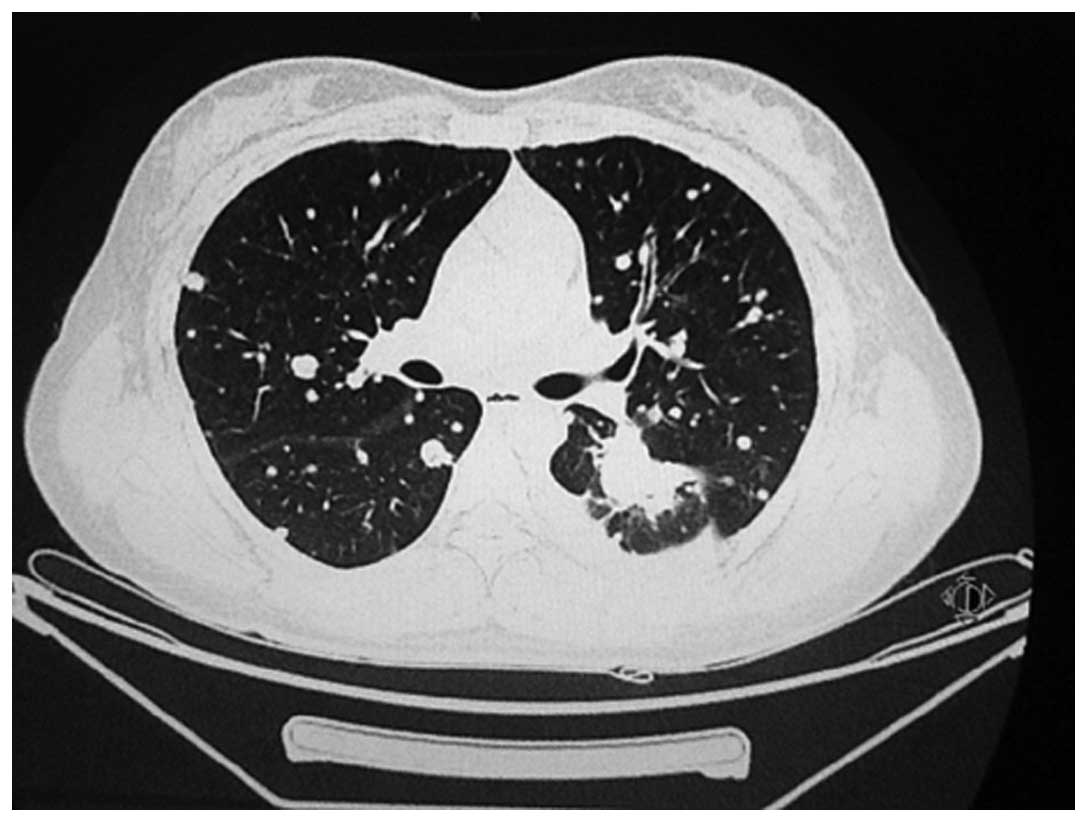
A 30-year-old female who had never smoked was
referred to the Chinese People’s Liberation Army General Hospital
(Beijing, China) for a persistent dry cough in July 2010. A chest
computed tomography (CT) scan revealed a mass of 31×26 mm in size
in the left lower lobe, and enlarged hilar lymph nodes and
metastases in each lung (Fig. 1). A
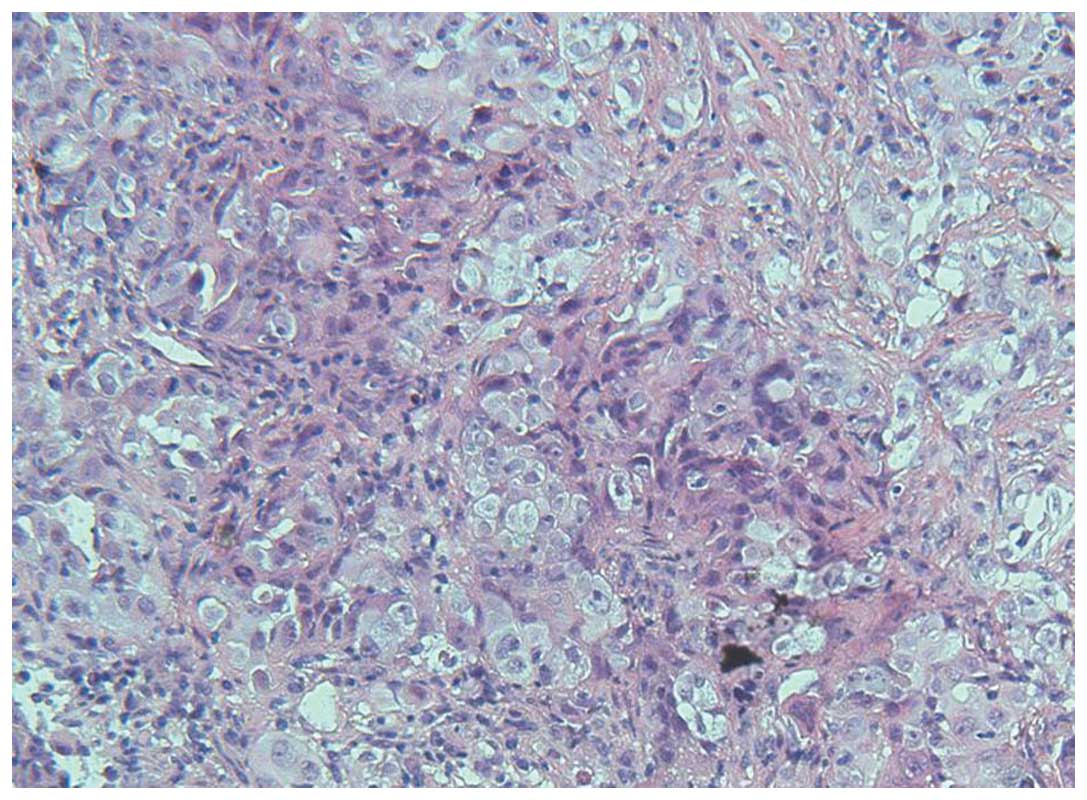
trans-bronchial lung biopsy (TBLB) was performed. The pathological
diagnosis of the TBLB specimen was of a poorly-differentiated
adenocarcinoma (Fig. 2). The
laboratory findings were within the normal ranges, with the
exception of a carcinoembryonic antigen level of 45.34 μg/l (normal
range, 0–5.0 μg/l) in the serum. According to the clinical and
histological findings, the patient was diagnosed with stage IV
pulmonary adenocarcinoma (cT4N1M1a).
The patient was treated with first-line chemotherapy
consisting of cisplatin (75 mg/m2) and pemetrexed (PEM)
(500 mg/m2) every three weeks, while simultaneous
mutation analysis of the epidermal growth factor receptor (EGFR)
gene was performed. However, no marked response was observed
following two cycles of treatment. The subsequent EGFR mutation
analysis revealed a L858R point mutation of exon 21 and a Q787Q
point mutation of exon 20. Therefore, erlotinib was administered
orally at a dose of 150 mg daily as the second-line therapy. A
partial response was obtained one month after this targeted therapy
and the prolonged overall tumor shrinkage lasted 25 months until
the patient went to Cuba for CIMAvax-EGF vaccine therapy. CIMAvax
EGF is a therapeutic anticancer vaccine developed entirely in Cuba
and licensed in Cuba for use in adult patients with stage IIIB/IV
NSCLC (10). The vaccine was
administered at 4 anatomical sites (in 2 deltoid and 2 gluteus
muscles), distributed at a dose equivalent to 2.4 mg of the
antigen, corresponding to 0.6 mg of EGF in 1.2 ml water in oil
emulsion per site on days 1, 7, 14 and 28, and monthly afterwards.
The disease was stable for 6 months until a chest CT scan showed an
enlarged primary lesion and increased pulmonary metastases. A
combination of erlotinib (150 mg/day) treatment and cisplatin (75
mg/m2) + pemetrexed (500 mg/m2) chemotherapy
were suggested subsequently. Subsequent to the completion of three
cycles of treatment, no evident changes were documented on the
chest CT, but a grade 4 (according to the Common Terminology
Criteria for Adverse Events version 4.0) increase in alanine
aminotransferase (ALT) and aspartate aminotransferase (AST)
developed (11). The erlotinib
treatment and chemotherapy were stopped, and the hepatoprotective
agents, magnesium isoglycyrrhizinate, polyene phosphatidylcholine
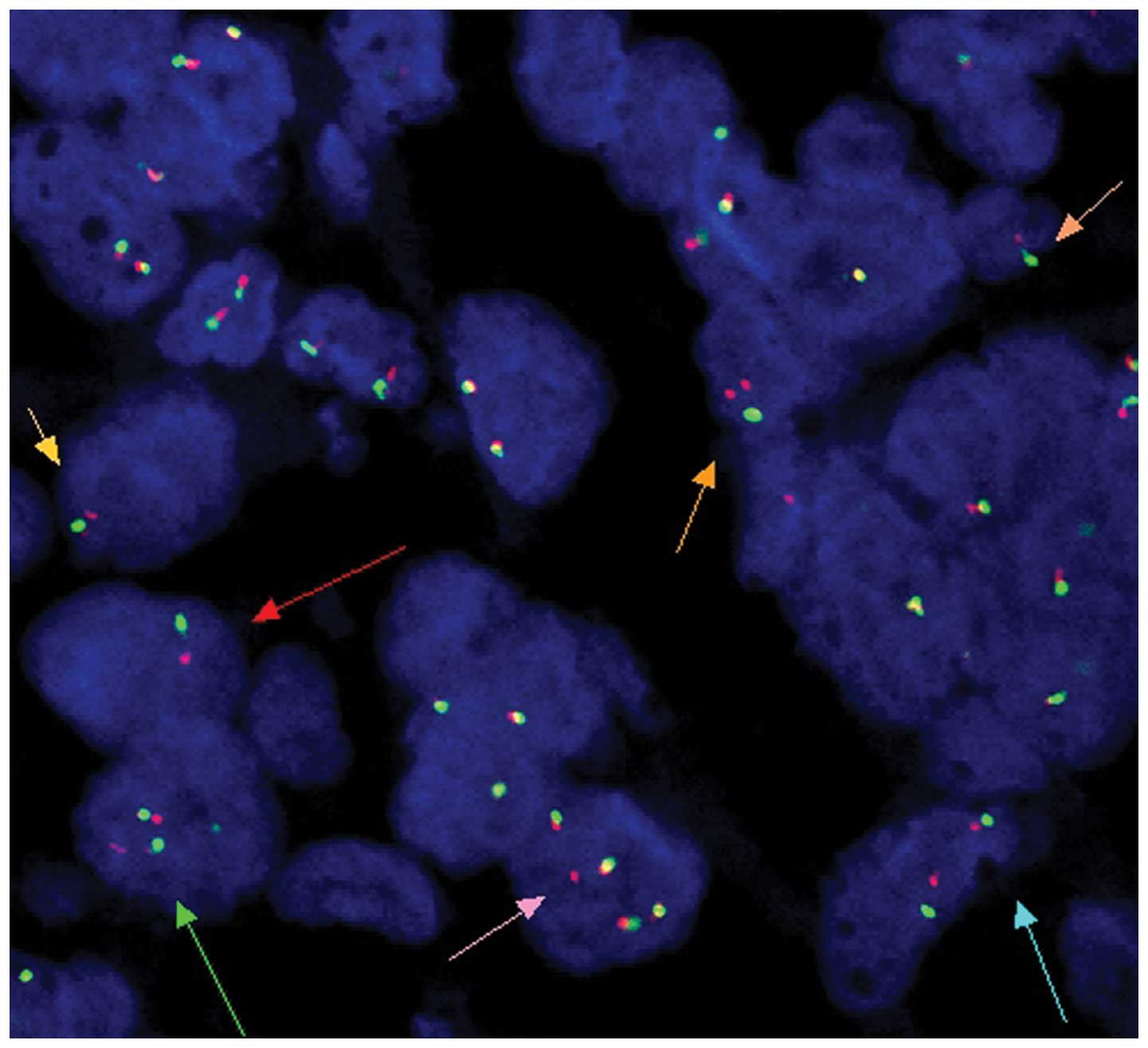
and reduced glutathione, were administered to the patient. A repeat
biopsy was also conducted. DNA sequencing and fluorescence in
situ hybridization analysis were used to detect the presence of
EGFR and KRAS mutations and the ALK gene, respectively. The result
revealed the wild-type KRAS and EGFR genes and ALK rearrangements
(Fig. 3). Considering the shift in
mutation status of the EGFR gene and the ALK rearrangements, the
patient was treated with crizotinib (250 mg, twice a day) when the
AST and ALT levels returned to normal. Slow progress was observed
after 30 days, but the patient maintained a stable disease (SD)
state according to the response evaluation criteria in solid tumors
(12). Crizotinib treatment was
continued until the last follow-up. Written informed consent was
obtained from the patient for publication of this case study and
the accompanying images.
Discussion
EGFR-TKIs demonstrate efficacy in the treatment of
patients with NSCLC who harbor activating EGFR mutations. These
patients develop disease progression following a median response
time of 10–14 months (13). The
acquired resistance is unavoidable due to a number of different
mechanisms, including c-Met amplification, activation of
alternative pathways, T790M and tumor heterogeneity (14). The inconsistent status of EGFR
mutations, also called heterogeneity, is believed to be associated
with the secondary mutation of tumor cells, or to have existed
during the transformation of a normal cell to a cancerous cell. A
study by Shimizu et al (15)
demonstrated the difference on the distribution of EGFR mutations
between primary tumors and metastatic lymph nodes (MLNs) in
patients with resected NSCLC, and indicated that the EGFR mutation
status of MLN is a predictive marker of the response to EGFR-TKI
therapy. Bai et al (16)
provided evidence that chemotherapy may affect EGFR mutation status
in tissue and peripheral blood samples. It was also reported that
genetic changes associated with crizotinib resistance are
heterogeneous in NSCLC patients with ALK rearrangements who respond
to crizotinib and subsequently develop resistance (17). Therefore, secondary biopsies of
growing tumors at the onset of clinical progression are crucial for
guiding the subsequent treatment, although this is often not easy
in clinical practice (18).
In the present case, the patient benefited from
targeted therapy for more than two years and the EGFR mutation
status changed following a series of treatments and disease
progression. However, confirmation is required to assess whether
the shift was derived from the chemotherapy, immunotherapy or the
ALK rearrangements. The patient showed a good response to the
erlotinib treatment initially, but not to the crizotinib. This
indicates an association between the secondary mutations in kinases
and the drug resistance to TKIs. The case should also highlight the
fact that repeat biopsies for genomic evolution are necessary to
aid in the clarification of the mechanism behind the development of
the acquired drug resistance to TKIs, and that this may pave the
way for the selection of appropriate treatments (19).
References
|
1
|
Hensing T, Chawla A, Batra R and Salgia R:
A personalized treatment for lung cancer: molecular pathways,
targeted therapies, and genomic characterization. Adv Exp Med Biol.
799:85–117. 2014.
|
|
2
|
Kaneda H, Yoshida T and Okamoto I:
Molecularly targeted approaches herald a new era of non-small-cell
lung cancer treatment. Cancer Manag Res. 5:91–101. 2013.
|
|
3
|
Gainor JF, Varghese AM, Ou SH, et al: ALK
rearrangements are mutually exclusive with mutations in EGFR or
KRAS: an analysis of 1,683 patients with non-small cell lung
cancer. Clin Cancer Res. 19:4273–4281. 2013.
|
|
4
|
Kuo YW, Wu SG, Ho CC and Shih JY: Good
response to gefitinib in lung adenocarcinoma harboring coexisting
EML4-ALK fusion gene and EGFR mutation. J Thorac Oncol.
5:2039–2040. 2010.
|
|
5
|
Popat S, Vieira de Araújo A, Min T, et al:
Lung adenocarcinoma with concurrent exon 19 EGFR mutation and ALK
rearrangement responding to erlotinib. J Thorac Oncol. 6:1962–1963.
2011.
|
|
6
|
Miyanaga A, Shimizu K, Noro R, et al:
Activity of EGFR-tyrosine kinase and ALK inhibitors for
EML4-ALK-rearranged non-small-cell lung cancer harbored coexisting
EGFR mutation. BMC Cancer. 13:2622013.
|
|
7
|
Tanaka H, Hayashi A, Morimoto T, et al: A
case of lung adenocarcinoma harboring EGFR mutation and EML4-ALK
fusion gene. BMC Cancer. 12:5582012.
|
|
8
|
Toyokawa G, Taguchi K, Ohba T, et al:
First case of combined small-cell lung cancer with adenocarcinoma
harboring EML4-ALK fusion and an exon 19 EGFR mutation in each
histological component. J Thorac Oncol. 7:e39–e41. 2012.
|
|
9
|
Sasaki T, Koivunen J, Ogino A, et al: A
novel ALK secondary mutation and EGFR signaling cause resistance to
ALK kinase inhibitors. Cancer Res. 71:6051–6060. 2011.
|
|
10
|
Rodríguez PC, Rodríguez G, González G and
Lage A: Clinical development and perspectives of CIMAvax EGF, Cuban
vaccine for non-small-cell lung cancer therapy. MEDICC Rev.
12:17–23. 2010.
|
|
11
|
National Cancer Institute (NCI). Common
Terminology Criteria for Adverse Events (CTCAE), version 4.03. June
14–2010
|
|
12
|
Eisenhauer EA, Therasse P, Bogaerts J, et
al: New response evaluation criteria in solid tumours: revised
RECIST guideline (version 1.1). Eur J Cancer. 45:228–247. 2009.
|
|
13
|
Oxnard GR, Arcila ME, Chmielecki J,
Ladanyi M, Miller VA and Pao W: New strategies in overcoming
acquired resistance to epidermal growth factor receptor tyrosine
kinase inhibitors in lung cancer. Clin Cancer Res. 17:5530–5537.
2011.
|
|
14
|
Lee JC, Jang SH, Lee KY and Kim YC:
Treatment of non-small cell lung carcinoma after failure of
epidermal growth factor receptor tyrosine kinase inhibitor. Cancer
Res Treat. 45:79–85. 2013.
|
|
15
|
Shimizu K, Yukawa T, Hirami Y, et al:
Heterogeneity of the EGFR mutation status between the primary tumor
and metastatic lymph node and the sensitivity to EGFR tyrosine
kinase inhibitor in non-small cell lung cancer. Target Oncol.
8:237–242. 2013.
|
|
16
|
Bai H, Wang Z, Chen K, et al: Influence of
chemotherapy on EGFR mutation status among patients with
non-small-cell lung cancer. J Clin Oncol. 30:3077–3083. 2012.
|
|
17
|
Kim S, Kim TM, Kim DW, et al:
Heterogeneity of genetic changes associated with acquired
crizotinib resistance in ALK-rearranged lung cancer. J Thorac
Oncol. 8:415–422. 2013.
|
|
18
|
Ji W, Choi CM, Rho JK, et al: Mechanisms
of acquired resistance to EGFR-tyrosine kinase inhibitor in Korean
patients with lung cancer. BMC Cancer. 13:6062013.
|
|
19
|
Murtaza M, Dawson SJ, Tsui DW, et al:
Non-invasive analysis of acquired resistance to cancer therapy by
sequencing of plasma DNA. Nature. 497:108–112. 2013.
|