Introduction
Gastric cancer presents a worldwide health issue,
which accounts for ~934,000 (8.6%) of newly diagnosed cancer cases
and 700,349 mortalities annually. Almost two-thirds of cases occur
in Eastern Europe, South America and Asia, with 42% of cases
occurring in China alone (1). The
mean age of gastric carcinoma patients is 60 years, with a
relatively infrequent occurrence in individuals aged <40 years.
In addition, gastric cancer is more common in males than females,
with a ratio of 1.7:1 (2). Only
0.1% of all cases of gastric carcinoma occur during pregnancy
(3). In Japan, the rate of gastric
cancer during pregnancy is reported to be just 0.016% (4); however, in China, it exhibits a
frequency of 0.67%, which is significantly higher than that of
other countries (5). The diagnosis
of this type of cancer is difficult due to the high frequency of
benign gastrointestinal symptoms that are presented during normal
pregnancies, which results in a poor prognosis, resulting in 88% of
females succumbing to the disease within one year (6).
Gastric cancer metastasis invade the surrounding
tissues and distant organs, affecting cancer cell motility,
intravasation, transit in the blood or lymph and extravasation.
Friedreich (7) reported the first
case of carcinoma metastasis to the fetus in 1866; however,
metastasis to the placenta or fetus is extremely rare with <100
cases reported (8). The most common
among these are malignant melanomas, accounting for 30% of cases.
Lung, hematological and breast malignancies are the second most
common malignancies involved and gastric cancer accounts for <5%
of the cases reported (3,9). To date, to the best of our knowledge,
only six cases of metastasis from gastric cancer to the placenta or
fetus have been reported. In the current study the seventh case is
presented, which was the first case identified in China. The
patient provided written informed consent.
Case report
A 35-year-old female (gravida, 2; para, 0) was
admitted to Beijing Chaoyang Hospital (Beijing, China) at 34 weeks
of gestation and was diagnosed with preeclampsia due to high blood
pressure and a recent occurrence of proteinuria. The patient
experienced occasional nausea and epigastric pain during the second
trimester, however, did not receive adequate medical treatment.
Physical examination revealed that the uterus was
normal for the gestational stage, without abdominal tenderness or
peritoneal symptoms. In addition, the generalized superficial lymph
nodes were found to be of normal size.
Laboratory test results revealed a white blood cell
count of 13.94×109 cells/l, a red blood cell count of
2.86×1012 cells/l, a hemoglobin level of 94 g/l, a
platelet count of 125×109 cells/l, a D-Dimer level of
22.55 mg/l, a fasting blood glucose (Fbg) level of 121.1 mg/dl,
aspartate aminotransferase levels of 14 U/l, alanine
aminotransferase levels of 13 U/l and albumin levels of 27.6
g/l.
An abdominal ultrasound revealed a 34-week single
pregnancy. Two days later the patient developed a coagulation
disorder, which resulted in a decrease in serum Fbg to 94.3 mg/dl.
An emergency cesarean section under spinal anesthesia was
performed. The surgery revealed chylous ascites (100 ml) and the
placenta was pathologically analyzed. A premature female infant
(weight, 2,210 g) with an Apgar score (10) of 10 at 1, 5 and 10 min,
respectively, was delivered in a stable condition and was
transferred to the neonatal intensive care unit of Beijing Chaoyang
Hospital.
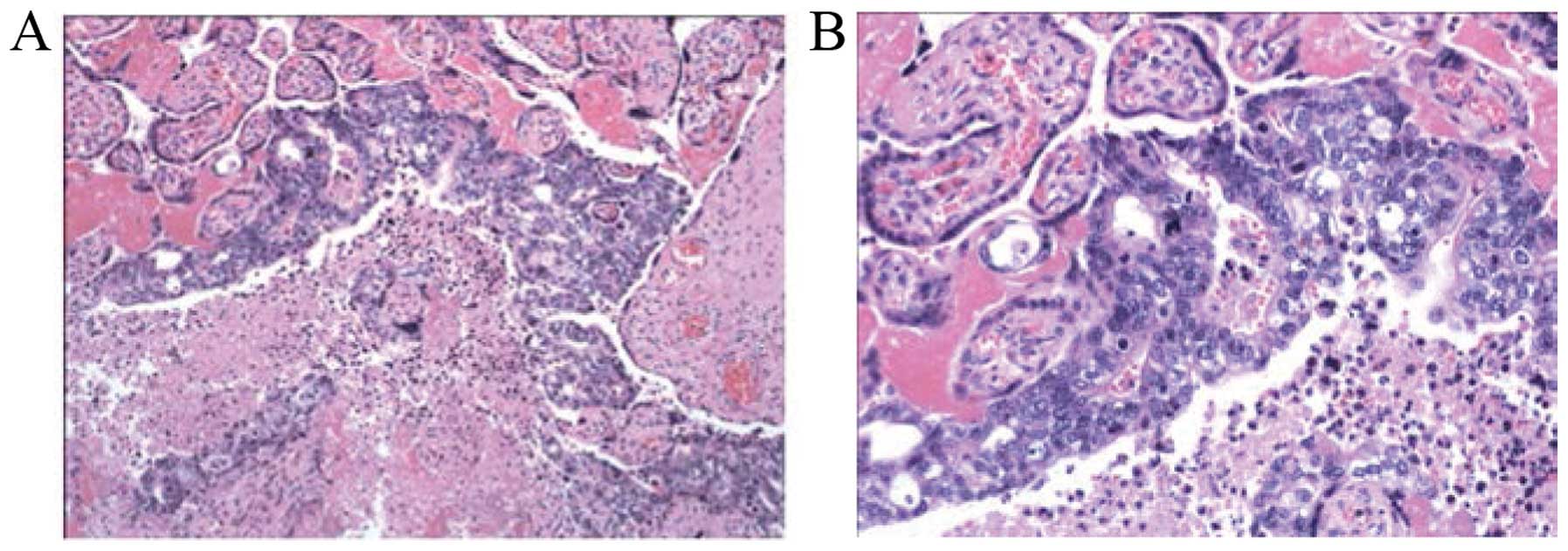
Macroscopic examination of the placenta revealed no
gross metastasis. However, microscopic analysis revealed gastric
primary malignant cells within the intervillous space with villous
invasion (Fig. 1). The umbilical
cord and membranes appeared normal. Computed tomography scan
revealed fundus thickening and enlarged retroperitoneal lymph
nodes. Gastroendoscopy was performed and revealed linitis plastica
with hypertrophic rugae and ulceration. In addition, a gastric
biopsy revealed an intermediate differentiated gastric
adenocarcinoma. The patient survived and has received chemotherapy.
Furthermore, the infant has been reported to be well six months
following delivery, with no evidence of fetal metastasis.
Discussion
There is often a delay in the diagnosis of gastric
cancer during pregnancy as the digestive symptoms are common and
commonly considered to be a benign response that is induced by the
pregnancy itself. This delay in diagnosis results in a poor
prognosis resulting in 88% of females succumbing to the disease
within one year (6).
Of the 92 cases of gastric cancer reviewed by
Jaspers et al (11), almost
all were found to be at an advanced stage of gastric cancer with
only two cases diagnosed with early stage cancer. Early gastric
cancer is difficult to detect during pregnancy, as the digestive
symptoms of pregnancy, including nausea and vomiting, are common
and do not usually require medical attention. Yoshida et al
(4) reported a case of a patient
with vomiting and epigastric pain in the second trimester. The
obstetricians diagnosed the patient with early stage gastric
cancer, which may have facilitated a favorable prognosis for the
mother and infant. Thus, patients with unusual digestive symptoms
subsequent to the first trimester require examination.
Gastroendoscopy has been identified as an effective method for the
detection of early gastric cancer and is regarded as a relatively
safe procedure that may be performed, when clinically required,
during gestation (12,13).
Gastric carcinoma diagnosed in pregnancy is rare,
occurring in only 0.1% of all cases of gastric carcinoma. Maternal
malignancy with metastasis to the placenta or fetus is extremely
rare with <100 cases reported, of which only ~20% cases were
reported to exhibit fetal metastasis (3). Gastric carcinoma accounts for <5%
of the reported cases. The majority of the reported cases were
identified in the intervillous space without villous invasion;
villous invasion is a significant risk factor for fetal
involvement, which was present in the current case. Previous
studies have recommended that a close follow-up of the healthy
infant should be performed, including a physical examination, chest
X-ray and liver function tests every six-months for the first two
years of life. For cases exhibiting placental and fetal metastasis,
further immunohistochemical examination of the mother and fetus is
also advised (12).
In conclusion, the potential of gastric cancer
during pregnancy must not be ignored, particularly in females
exhibiting unusual digestive symptoms. Further investigation must
be performed promptly for such patients, as early detection and
intervention are essential for improving the prognosis of the
mother and fetus. Histopathological examination of the placenta
with precise examination of the intravillous spaces and villous is
considered to be essential in every case of malignancy during
pregnancy.
References
|
1
|
Power DG, Kelsen DP and Shah MA: Advanced
gastric cancer - slow but steady progress. Cancer Treat Rev.
36:384–392. 2010.
|
|
2
|
Parkin DM, Pisani P and Ferlay J:
Estimates of the worldwide incidence of eighteen major cancers in
1985. Int J Cancer. 54:594–606. 1993.
|
|
3
|
Khatib F, Shaya M and Samueloff A: Gastric
carcinoma with metastasis to the placenta and amniotic fluid: case
report and review of the literature. Eur J Obstet Gynecol Reprod
Biol. 107:208–209. 2003.
|
|
4
|
Yoshida M, Matsuda H and Furuya K:
Successful treatment of gastric cancer in pregnancy. Taiwan J
Obstet Gynecol. 48:282–285. 2009.
|
|
5
|
Nv ZH: Clinical characteristics of gastric
cancer during pregnancy and the reasons for misdiagnosis. Zhonghua
Fu Chan Ke Za Zhi. 11:701–702. 2003.(In Chinese).
|
|
6
|
Hirabayashi M, Ueo H, Okudaira Y, et al:
Early gastric cancer and a concomitant pregnancy. Am Surg.
53:730–732. 1987.
|
|
7
|
Friedreich N: Review of the pathology of
cancer. Virchows Arch Path Anat. 36:465–482. 1866.(In German).
|
|
8
|
Baker AM, Haeri S, Shafer A and
Moldenhauer JS: Maternal gastric carcinoma metastatic to the
placenta. Eur J Obstet Gynecol Reprod Biol. 153:225–226. 2010.
|
|
9
|
Al-Adnani M, Kiho L and Scheimberg I:
Maternal pancreatic carcinoma metastatic to the placenta: a case
report and literature review. Pediatr Dev Pathol. 10:61–65.
2007.
|
|
10
|
Hacker NF, Gambone JC and Hobel CJ: Hacker
& Moore’s Essentials of Obstetrics and Gynecology. 5th edition.
Saunders; Philadelphia, PA: pp. 115–116. 2009
|
|
11
|
Jaspers VK, Gillessen A and Quakernack K:
Gastric cancer in pregnancy: do pregnancy, age or female sex alter
the prognosis? Case reports and review. Eur J Obstet Gynecol Reprod
Biol. 87:13–22. 1999.
|
|
12
|
Pentheroudakis G and Pavlidis N: Cancer
and pregnancy: poena magna, not anymore. Eur J Cancer. 42:126–140.
2006.
|
|
13
|
Offerhaus GJ, Tersmette AC, Giardiello FM,
et al: Evaluation of endoscopy for early detection of gastric-stump
cancer. Lancet. 340:33–35. 1992.
|